EndoTODAY ���ð� ����
EndoTODAY ���ð� ����
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [����. ������. gastric adenoma. gastric dysplasia)] - ��
[����. ������. gastric adenoma. gastric dysplasia)] - ��
2017�� 4�� 15�� ��õ�����ð漼�̳�
The Most 2026�� 4��ȣ. PDF 1.6M
1) ����
4) ���ð� ����
5) �ӻ��� ����
6) ġ��
7) �������� ���ð� ġ�� �� ������ ���ܵ� ����
8) �������� ���ð� ġ�� �� ������ ���ܵ� ����
9) 2014 Konkuk symposium lecture on adenoma
10) ���� ESD �� ������ CT���� �߰ߵ� �����
11) FAQ - ������������ ���� ���ɼ��� �����ϱ�?
12) References
![]() 1. What is adenoma and dysplasia? ������ �����̰� �������� �����ΰ�
1. What is adenoma and dysplasia? ������ �����̰� �������� �����ΰ�
| Adenoma | ���� |
| Dysplasia | ������ |
| Atypia | ������ |
Doland ���л������� dysplasia(������)�� ��abnormality of development; in pathology, alteration in size, shape, and organization of adult cells����, adenoma(����)�� ��a benign epithelial tumor in which the cells form recognizable glandular structures or in which the cells are derived from glandular epithelium������ ���ǵǰ� �ִ�.
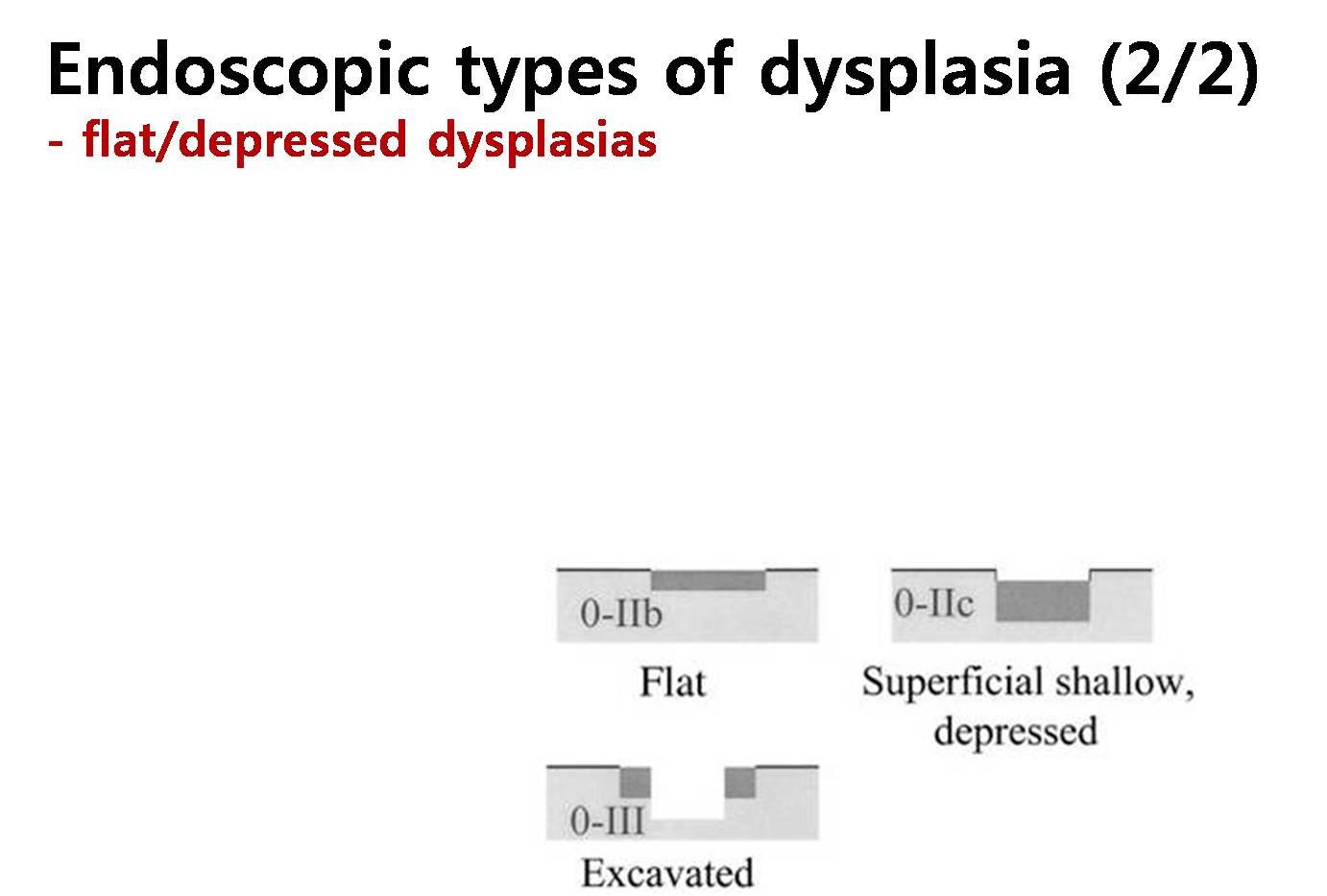
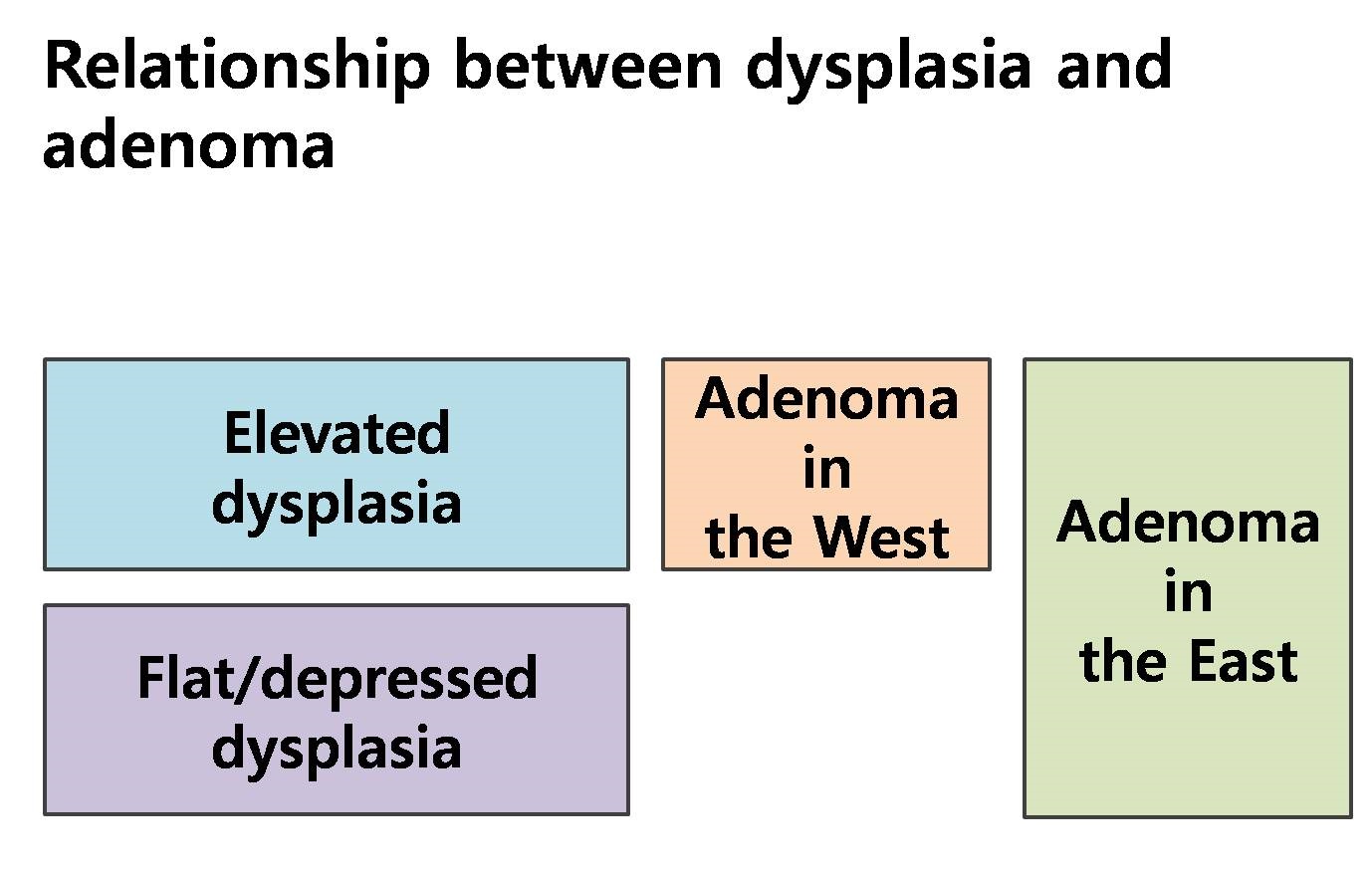
���������� �� ������ (gastric dysplasia)�� flat/depressed dysplasia�� elevated dysplasia�� �����µ� elevated dysplasia���� adenoma�� �θ���. �Ϻ��� �츮������ dysplasia�� adenoma�� ���� ���� ������ �����. ���� �Ϻ��� �츮������ flat/depressed adenoma�� elevated adenoma�� ��� �����ϴ�.
���翡���� ������ dysplasia�� �����̶�� �θ����� �츮�� ������ dysplasia�� �Ը��� dysplasia�� ��� �����̶�� �θ���. �� �츮����� �Ϻ������� "gastric dysplasia = gastric adenoma"�̴�.
�ֱ� ���� �ϰ� �������� ���� �������ڵ��� �� ������ �Ϻ����� ������ ���̸� ���δٴ� ���� ��������, �̸� �غ��ϱ� ���� �پ��� ����� ����ǰ� �ִ�. ���� ���� 1-2�⸶�� ���ο� �з����� ���õǰ� ������, �� ���� �� ��Ȯ�ϰ� �̷������ �������ν� ȥ���� ��ä���ϰ� �ִ�. Ư�� ���ſ��� ��������ۿ� �� �� ������ ������ ���ҿ� ���� ���ð� ġ�ᰡ ���ԵǸ鼭, �з� �� ���������� �ʿ伺�� ���� ����ǰ� �ִ�.
���� ȥ�������� ���� Revised Vienna �з��̴�. �̴� ���忡���� �������� ������ �������� ���� Ÿ������ �ʴ�. �ؾ������ ���� ���ٰ� �����ȴ�.
Revised Vienna�� �ؾ������.
* ����: EndoTODAY Opinion difference between Korea and Japan on gastric adenoma
![]() 2. Pathologic diagnosis. ����/�������� �������� ����
2. Pathologic diagnosis. ����/�������� �������� ����
�Ϲ������� �������� �������� ������ ������(gastric epithelial dysplasia)�� ��Ī�Ѵ�. ������ �̿��� ���������� �������� ���� �� �ִµ�, �̿� ���� ���� ��ü������ ������ ����� �����ִ� ���� �Ϲ����̴� (��: enterochromaffin-like dysplasia).
�������� �����ϱ� ����� ������ �����̴�. ���������� ���� �������� ������ ������(flat dysplasia)�� ������ ������(polypoid dysplasia)���� �����Ͽ� �������� ����� ���������� �������� �����Ͽ� �θ�� �Ѵ�. ���� �Ϲ������δ� ���� �������� ������ ȥ���Ͽ� ����ϰ� �ְ�, ��쿡 ���� adenoma/dysplasia�� ���� �Բ� ��������ν� ȥ���� ���ϰ��� �õ��DZ �Ѵ�.
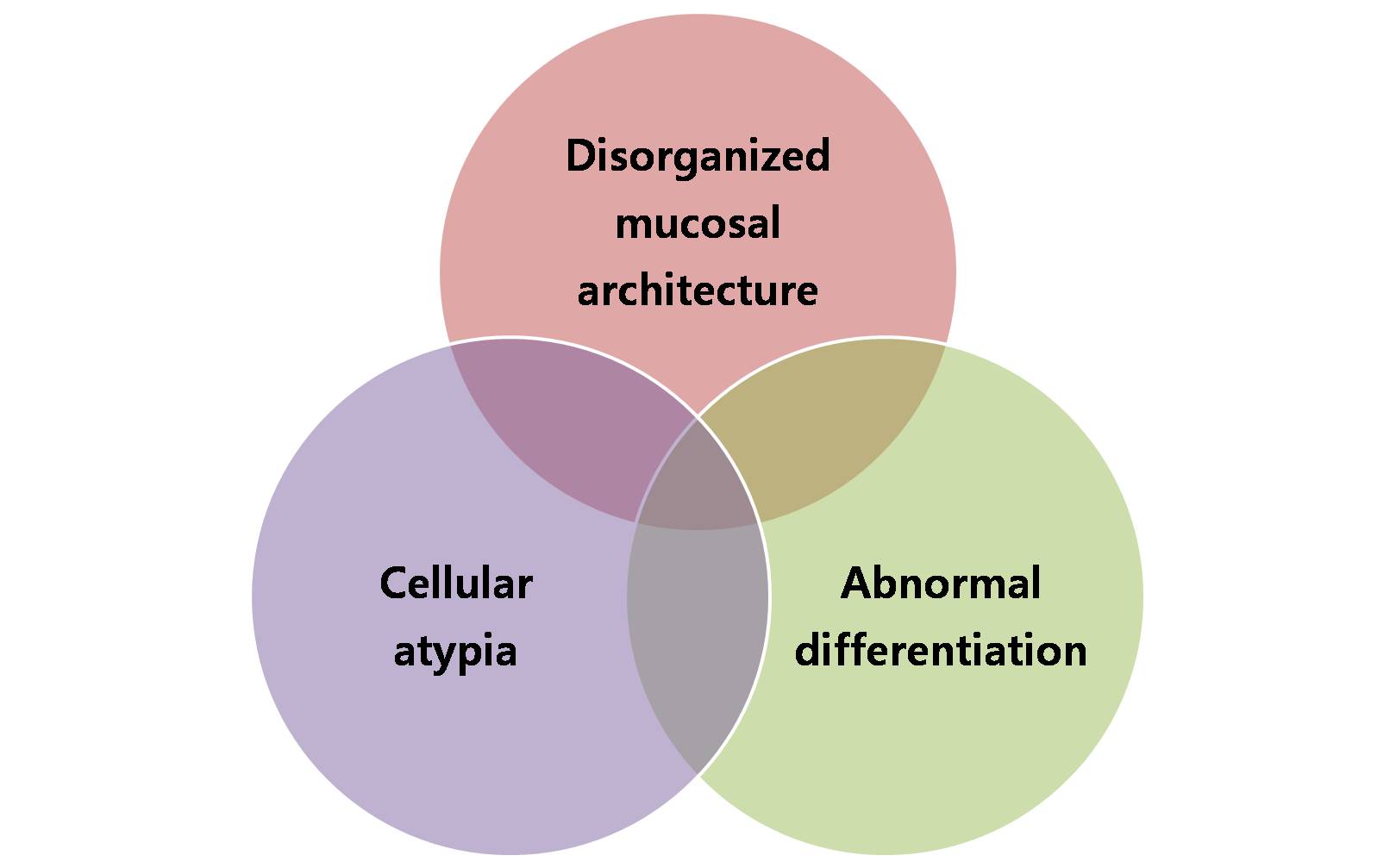
�������� ���������� Ư¡�� �Ʒ��� ����.
| Microscopic characteristics of gastric epithelial dysplasia |
| 1) Cellular atypia
- nuclear pleomorphism - hyperchromasia - nuclear stratification - increased N/P ratio - sometimes increased cytoplasmic basophilia - loss of cellular and nuclear polarity |
| 2) Abnormal differentiation
- lack or reduced numbers of goblet cells and Paneth cells in the metaplastic intestinal epithelium - reduction, alteration or disappearance of secretory products from the gastric epithelium |
| 3) Disorganized mucosal architecture
- irregularity of crypt structure - back-to-back gland formation - budding and branching of crypts - intraluminal and surface papillary growth |
������������ �������� ����� ���� regenerating atypia�ε�, �̴� ������ �ջ� ���� �������� ��������� �ϳ��� ���ֵǴ� ������ �ݵ�� ���еǾ�� �Ѵ�.
������ analogue�̴�. ��� ���� digital�� �������� �������� ������ �����ϰ� �Ѵ�. �ָ��� ���� �ָ��ϴٰ� ���ϴ� ���� ����.
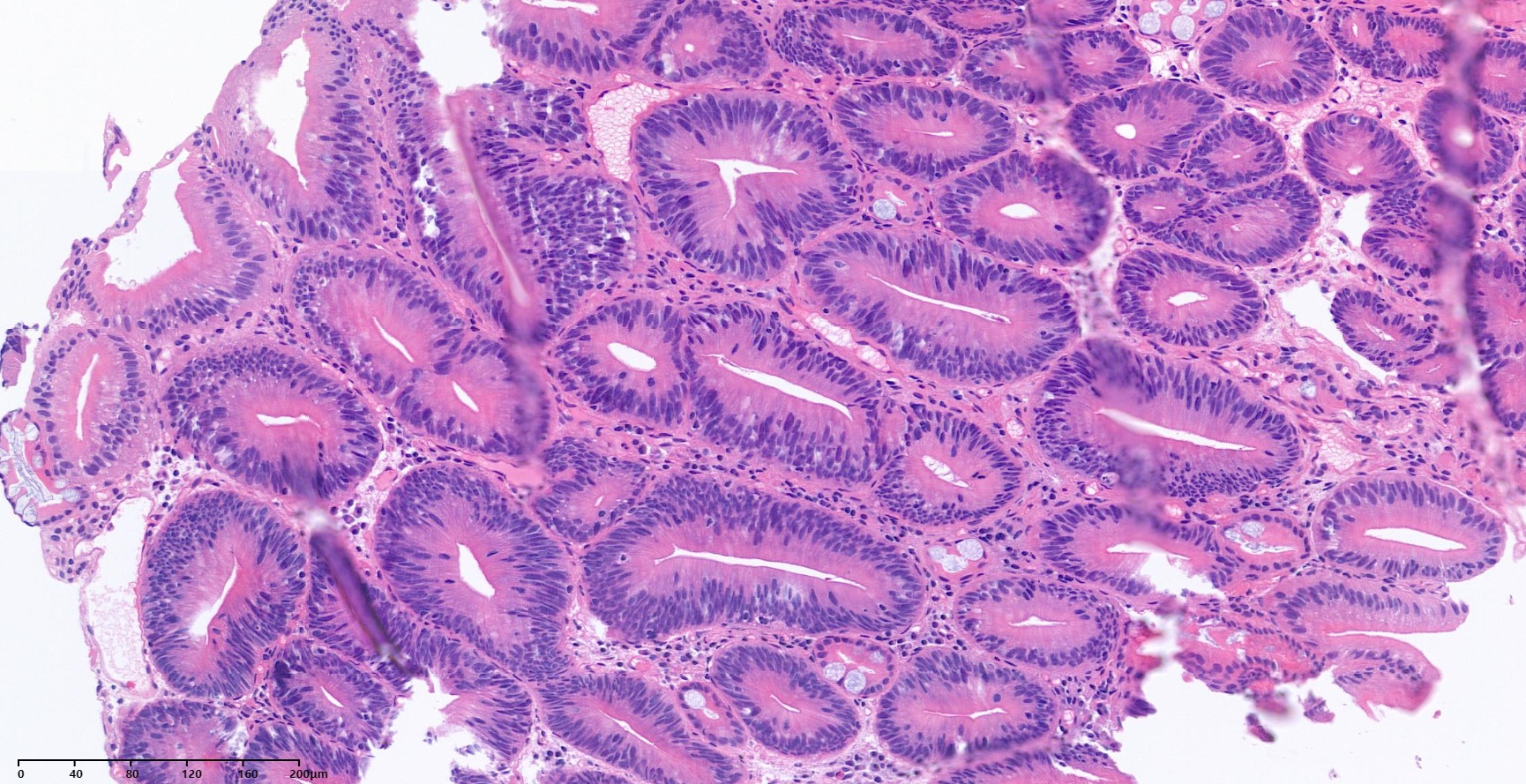
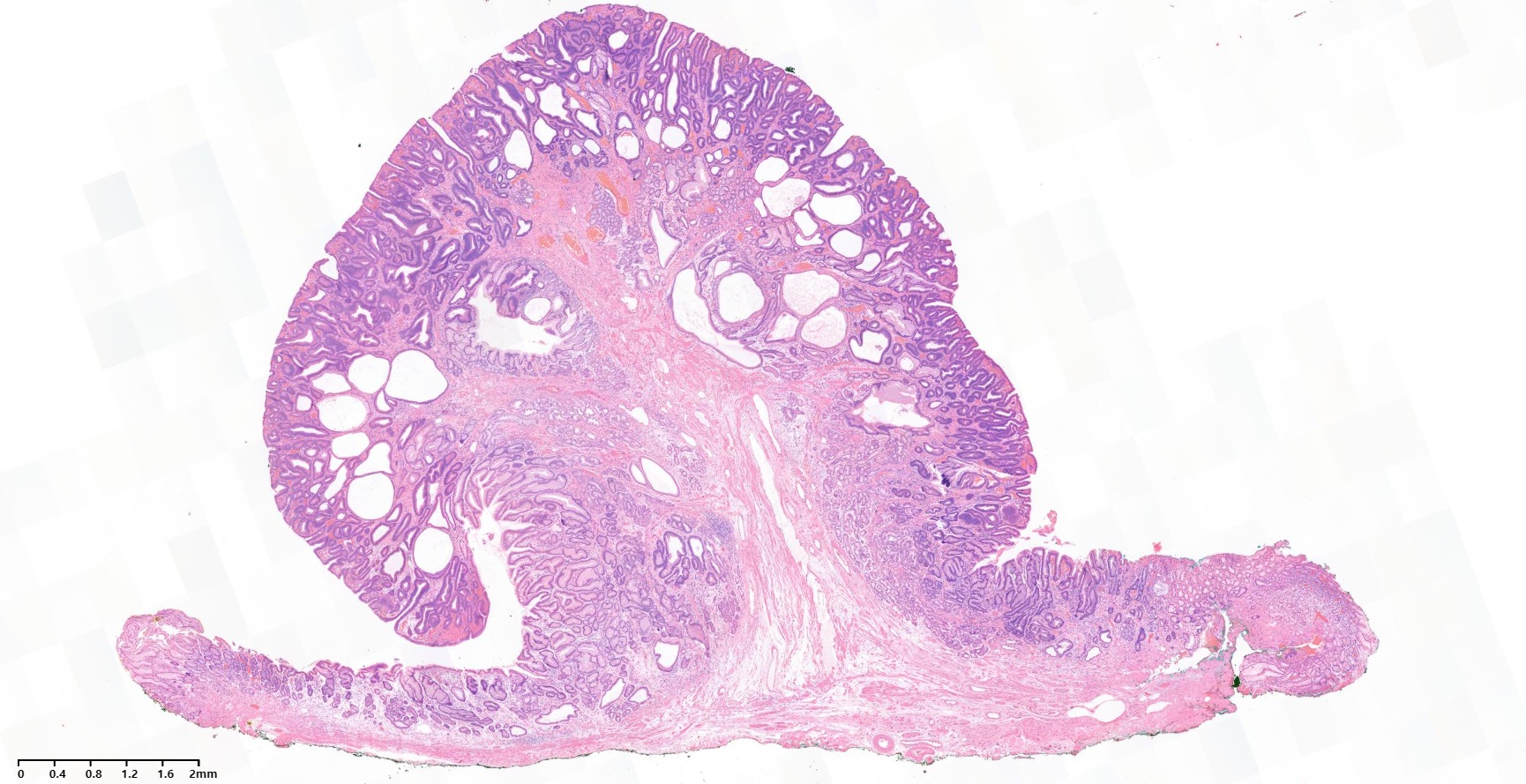
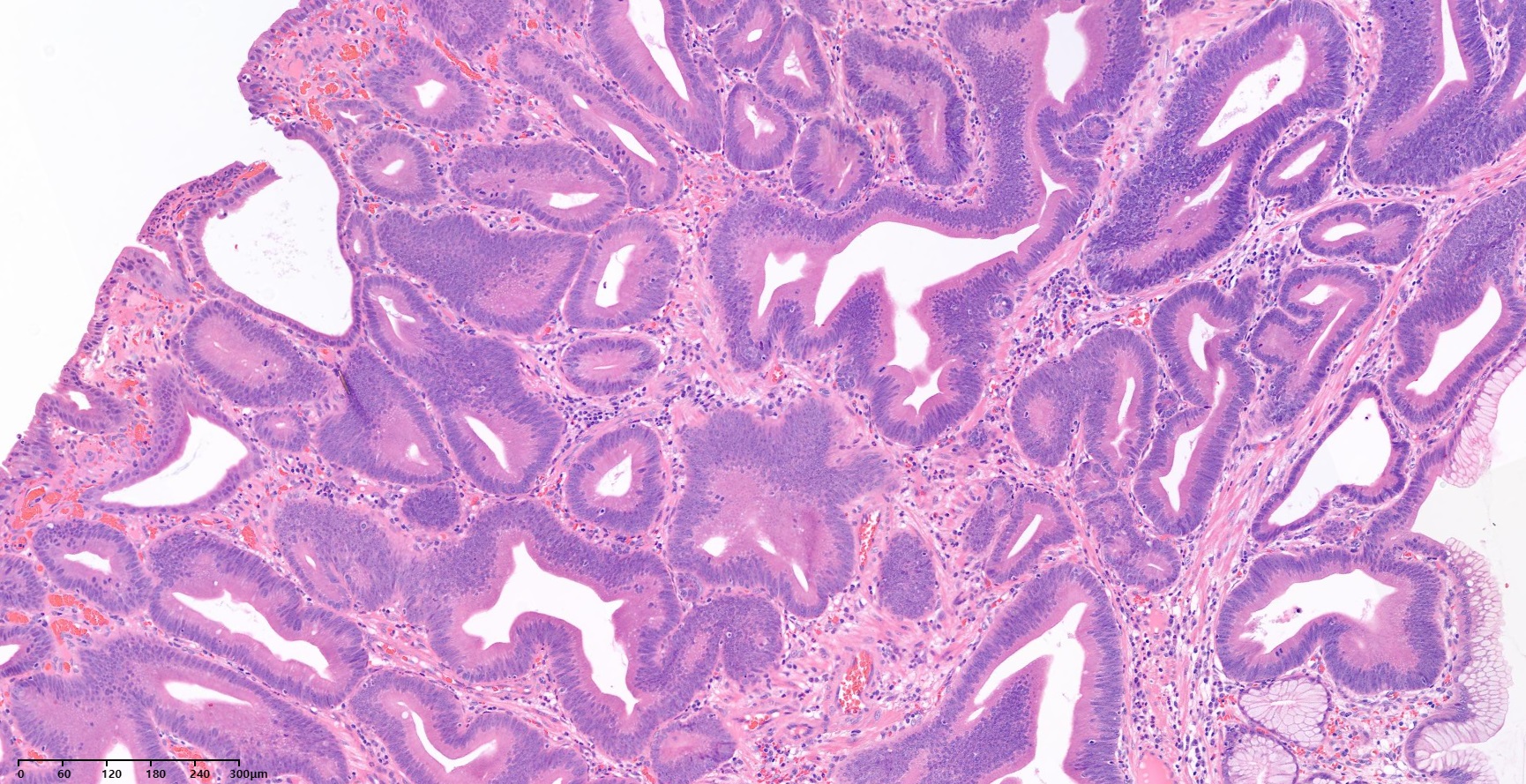
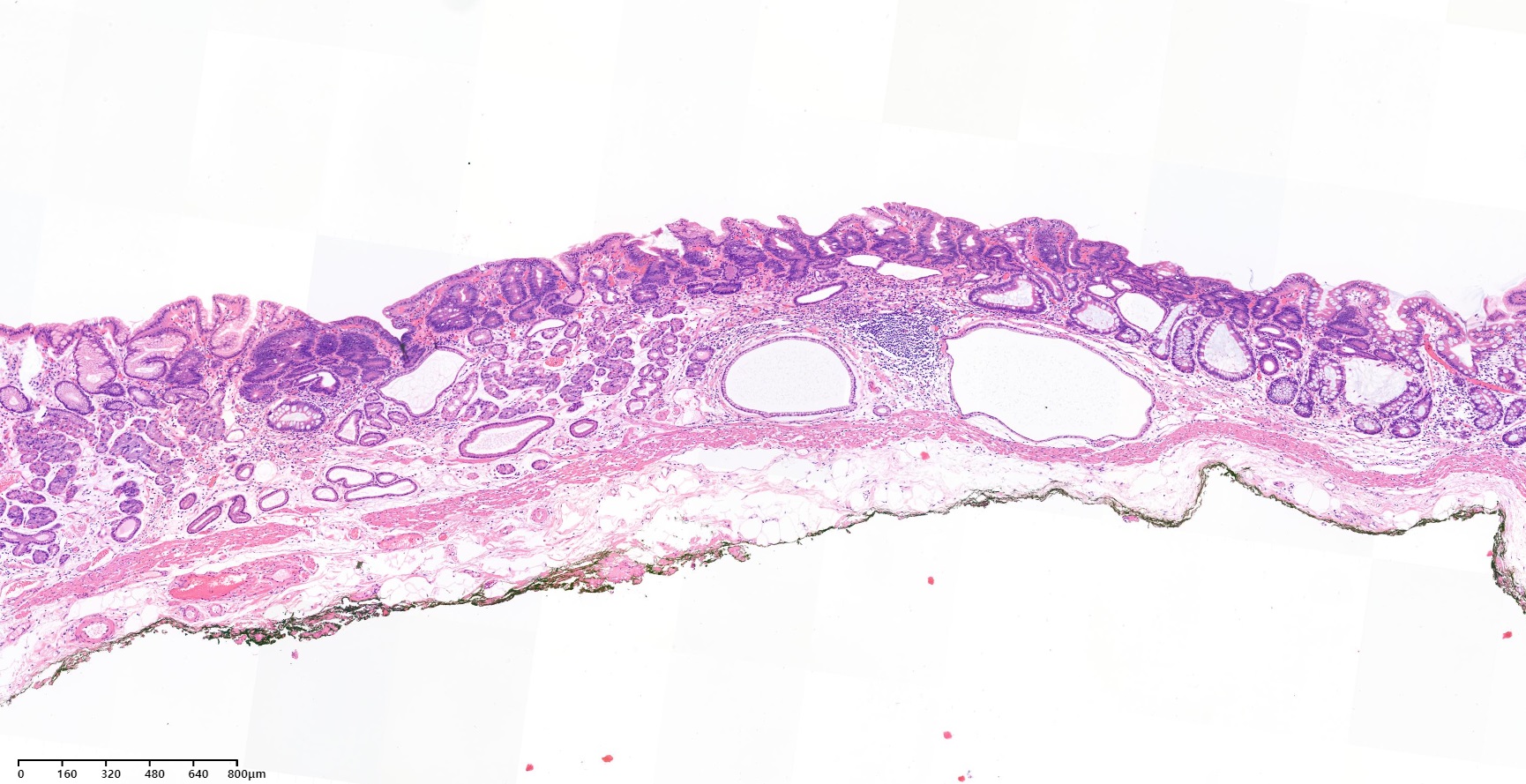
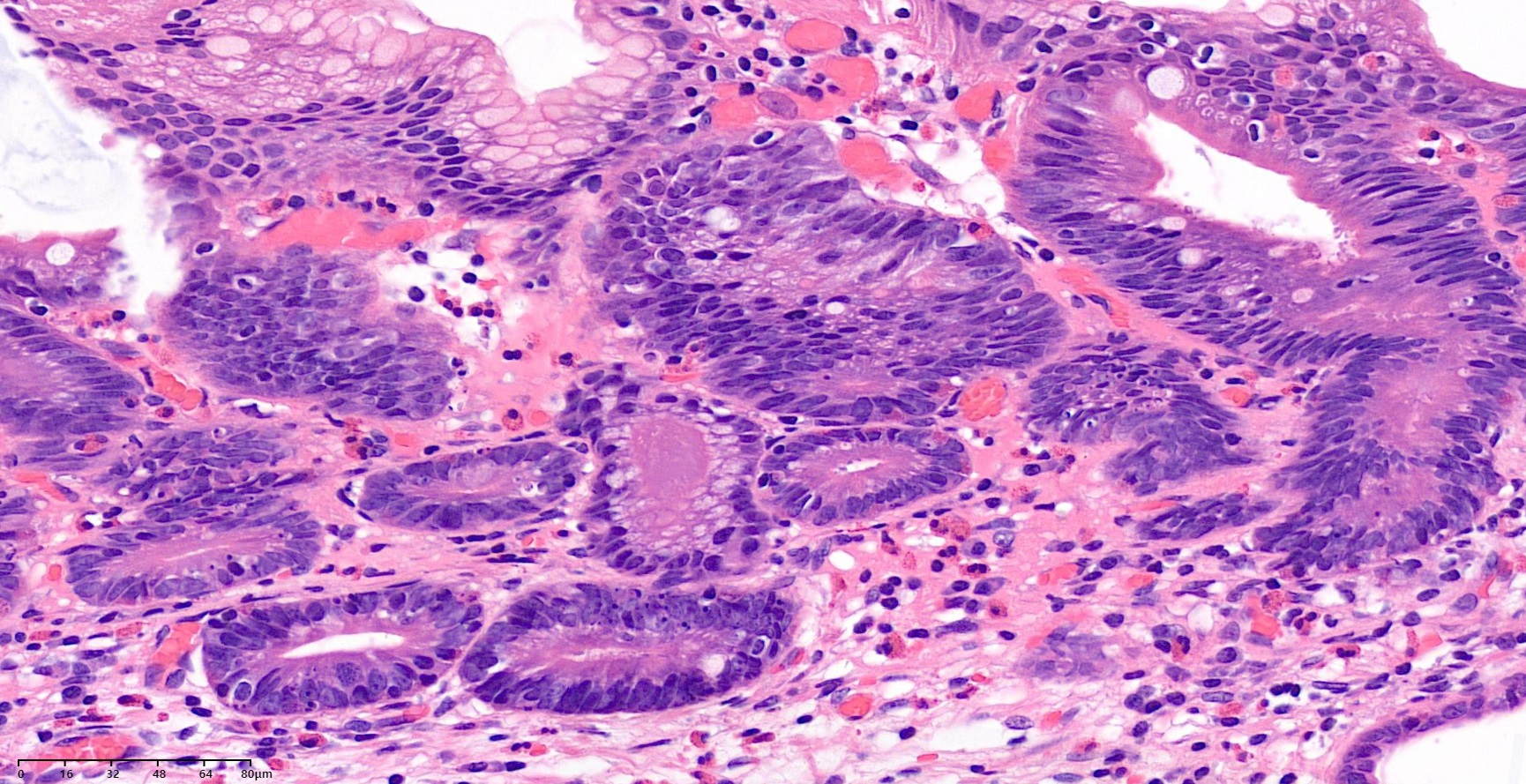
�Ʒ��� �����˻翡�� ������������ ���� ȯ���Դϴ�. ���ð����δ� ���� �������� metaplastic nodule���� ���� ������ ��ƽ��ϴ�.
![]() 3. Grading and classification. ����/���� ��� �з�
3. Grading and classification. ����/���� ��� �з�
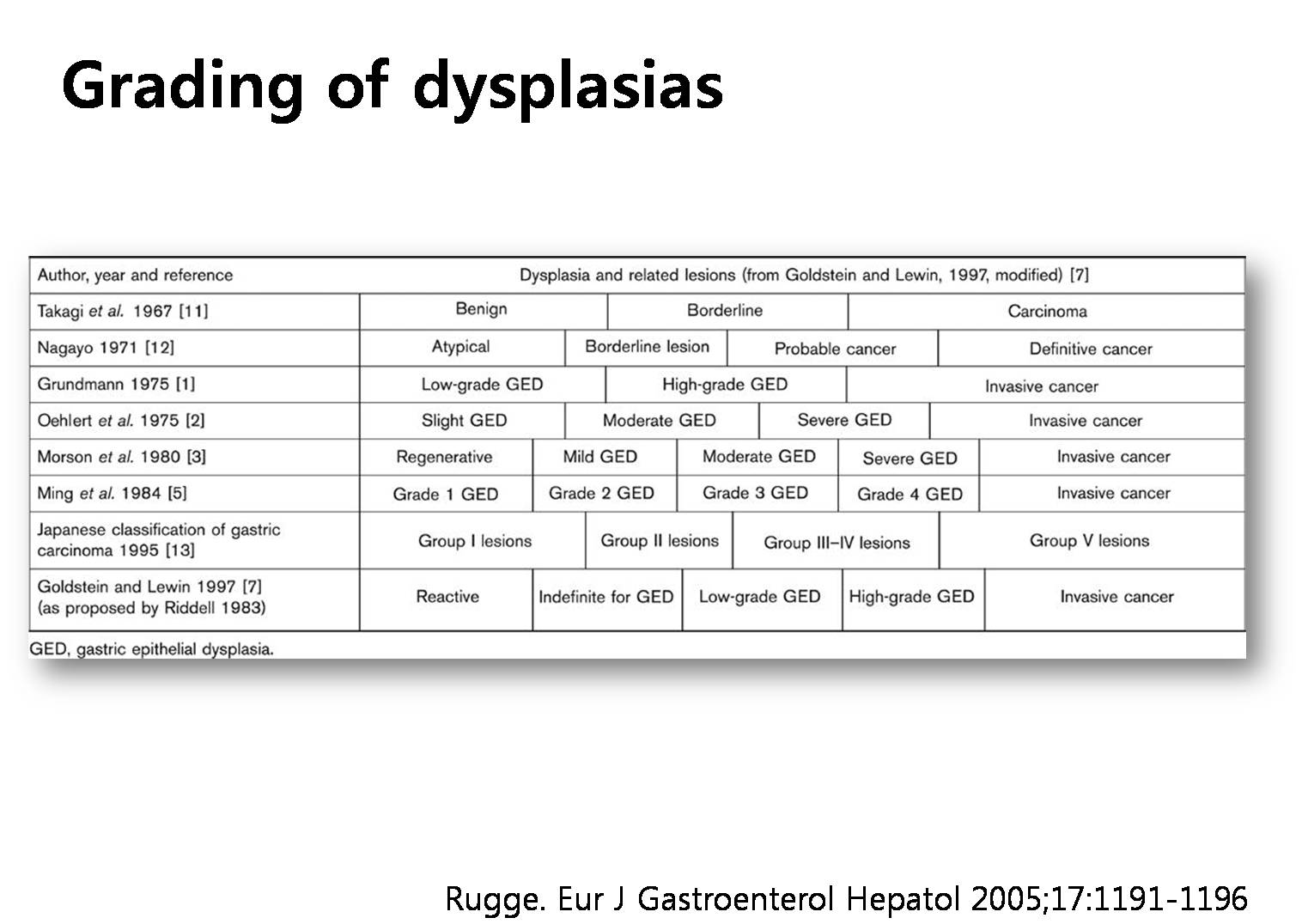
�����������δ� ������ ���� ������ ���ǰ� �ֽ��ϴ�.
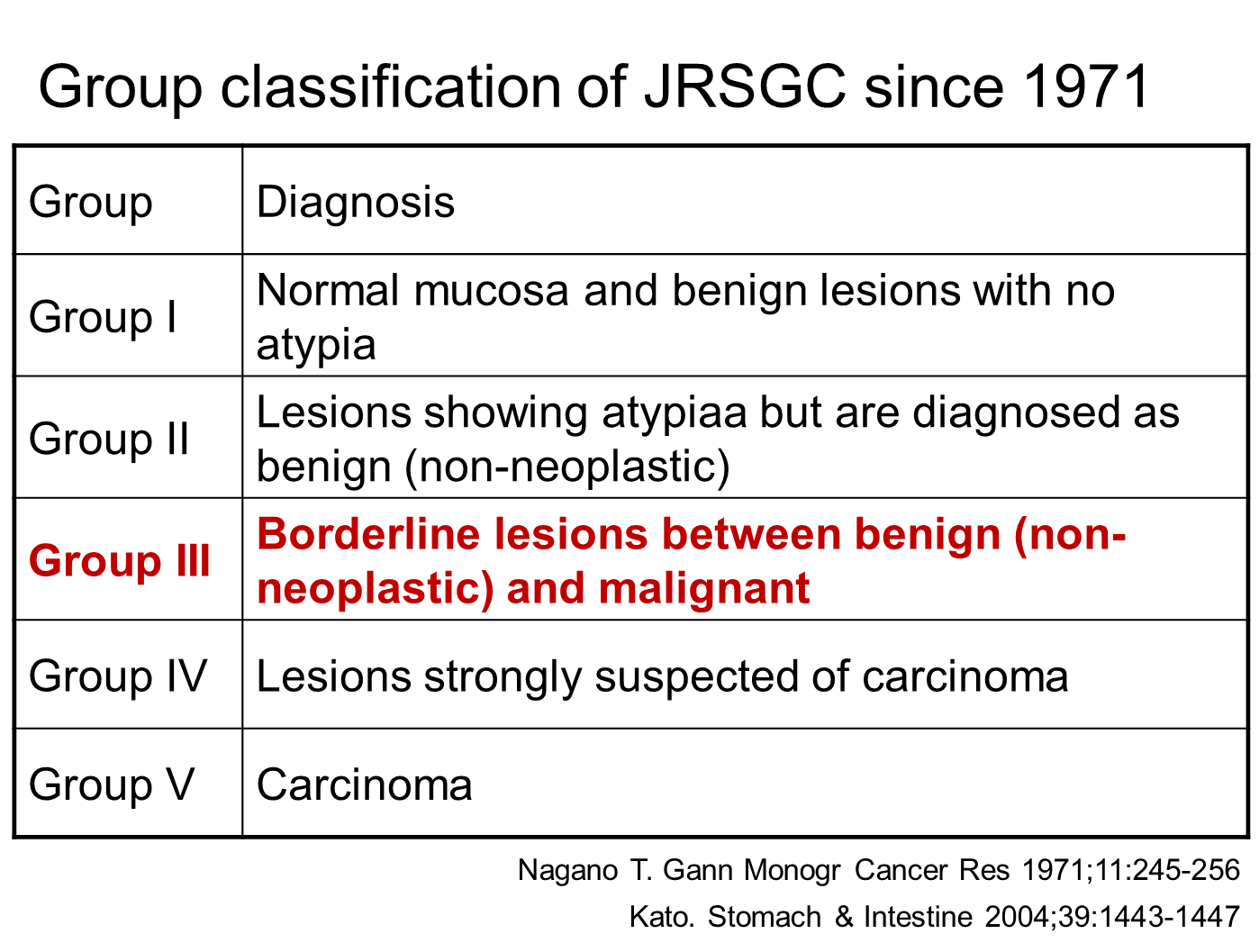
�Ϻ����� ���������� ������ ������ ���� ������ ���������� ������ 1996�� Nakamura�� ���Ͽ� ���õǾ�����, ���� 1971�� Nagayo�� ���Ͽ� 5���� ������ �з��� ����, 1985�� Japanese Research Society for Gastric Cancer (JRSGC)�� ���Ͽ� �ణ �����Ǿ� ���翡 �̸��� �ִ�.
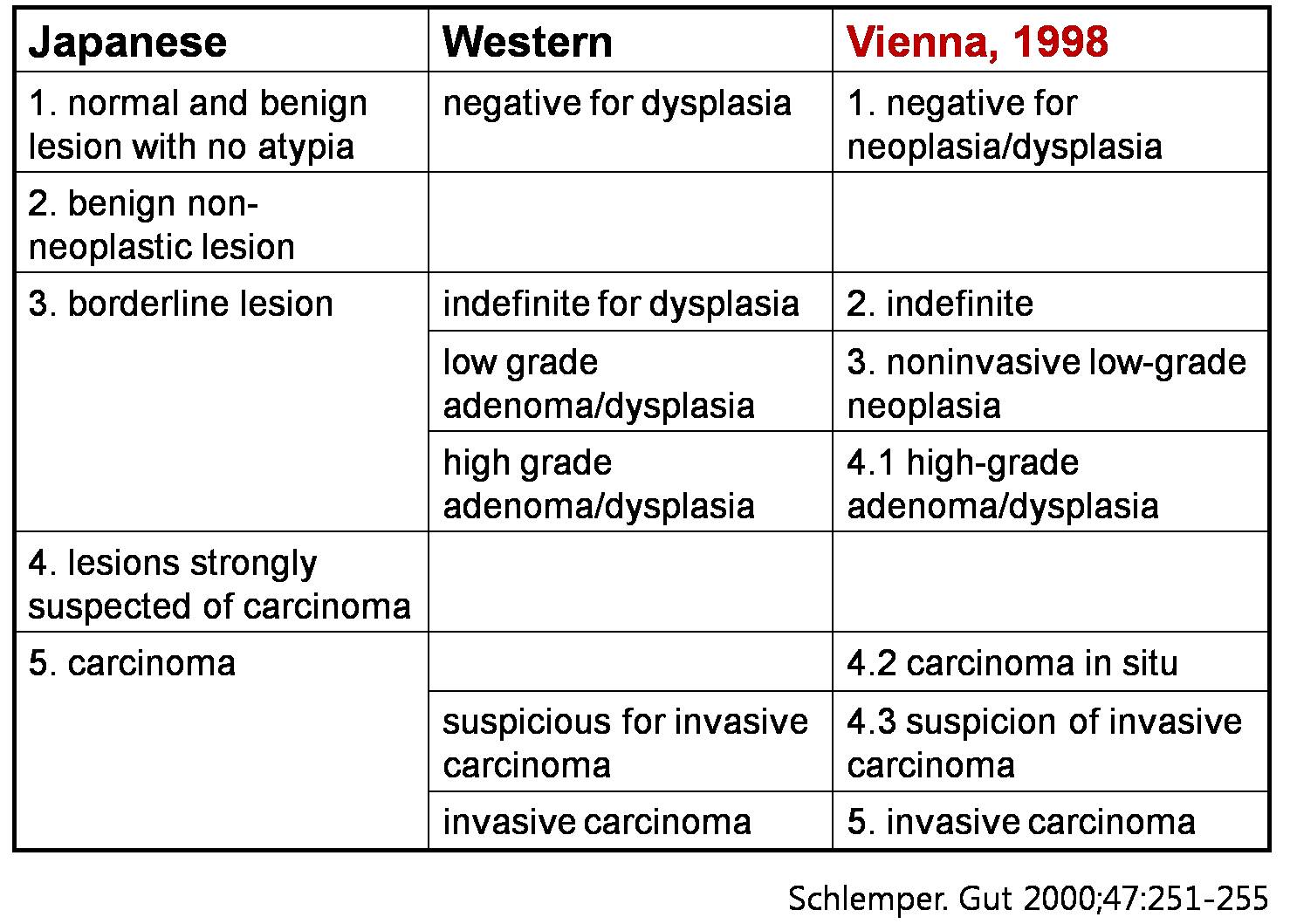
�Ϻ����� ���ǰ� �ִ� 5 �� �з��� ���� ū �������� ����輺���������� ��Ī�Ǵ� 3���� ������ �ʹ� �дٴ� ���ε�, �Ʒ����� ��Ǵ� Vienna �з��� category 2�� 3 �� 4�� ��ġ�� �������� ������ ������ 3���� ���Ե� �� �ִ�.
�̷��� �Ѱ������� �ұ��ϰ� 5 �� �з��� �����ð� �����˻��� ����� �����ϰ� ǥ���ϴ� ������� ���صǰ� �ְ�, �� �쿡 ���� ġ���ħ�� ���� ��Ȯ�ϰ� ���� �� �����Ƿ� �Ϻ������� �ſ� �������ϰ� �̿�ǰ� �ִ�. ���� ����� �Ϻ��� �������ڰ��� ���ظ� ��ġ��Ű�� ���� ����� Vienna �з��� Padova �з��� �⺻�����δ� �Ϻ��� 5 �� �з����� �����ϰ� �ֱ� ������ �� ������� �ſ� ũ�ٰ� �����ȴ�.
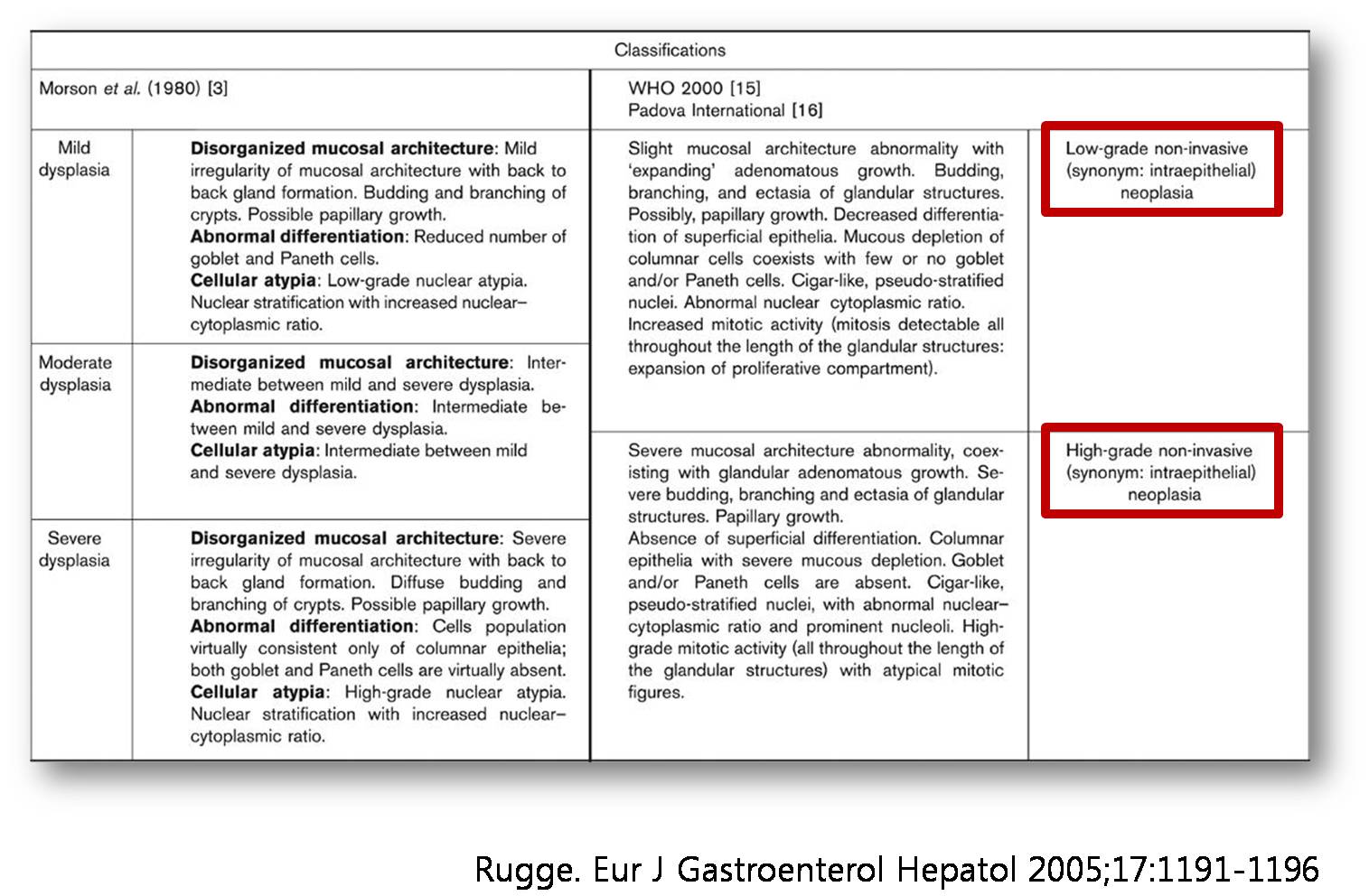
Vienna �з��� �ٸ� �з��� ��
������ ���ܿ� �־ �Ϻ��� ������ �������ڰ��� ���ش� �ſ� ���̰� ũ��. �Ϻ������� ������ ������ �������� Ư¡�� ���� ������ ���������� ���翡���� ħ���� ���Ű� ���� ������ �������� �����Ѵ�. ���� ���������� ������������ ��κа� ������������ �Ϻΰ� �Ϻ������� �������� ������ �ǰ� �ִ�. ���� �Ϻ������� ������ ���翡���� ���������� �ణ �ٸ� ���μ� ���ð� Ȥ�� ���ȼҰ߰��� �����ϸ�, ������ ���������� ������������ ����� �����̴�. ���� �Ϻ������� �Ը��� �����̶�� ������ �����ϴ�. �̿� ���Ͽ� ���翡���� �Ϲ������� �������� ���������� �����̶�� �θ��� �ִ�.
�̿� ���� �������� ���̿� ���� ��������� �ַ� Schlemper�� ���Ͽ� �̷������. Schlemper�� �ֵ��Ͽ� 1996�� ���濡�� ����ȸ�ǰ� ��������, �� ����� 1997�� ��Differences in diagnostic criteria for gastric carcinoma between Japanese and western pathologists����� �������� Lancet���� ó������ �Ǹ��鼭 �������� �ָ��� �ް� �Ǿ���.
���� 1998�� Vienna���� ���� World Congress of Gastroenterology���� consensus�� ����� ���� ȸ�ǰ� �������� �� ��� Vienna �з��� ���ȵǾ��� ������� ���� �θ� �̿�ǰ� �ִ�. 1998�� ��Ż������ Padova������ consensus�� ���� ȸ�ǰ� �������� �� ��� Padova �з��� ���ȵǾ��µ�, Vienna �з��� ���Ͽ� �̿�Ǵ� �� ���� �� �ϴ�. Padova �з������� category�� JRSGC�� ��� ���� ����� ������, Padova �з��� �Ϻ��� ������ ���翡�� ���� �������� �ʰ� �Ƶ��� ������ �����ص� ������ ������ �����ϴ�.
Vienna �з��� ���ȿ� �����Ͽ��� �Ϻ� �����ڵ��� 2000�� ȫ�ῡ�� ���� 11ȸ Asian Pacific Congress of Gastroenterology���� Vienna �з��� �ټ� ������Ų ���ο� �з����� �����Ͽ��� (��revised Vienna classification��). Vienna �з��� ��ǥ�� ���Ŀ��� ����� �Ϻ����� ���������� ���ܿ� �������� �������� ����Ǿ��µ�, �̵��� high-grade adenoma/dysplasia�� intramucosal carcinoma�� �� ������ �������μ� �������� ���̸� ���ְ��� �Ͽ���. ���� �������� ���� �ϳ��� ������ ���´ٴ� ���� ������ �������δ� �Ƶ��̱� ����� ������ revised Vienna classification�� �θ� ������ ���ϰ� �ִ� ������� �����ȴ�.
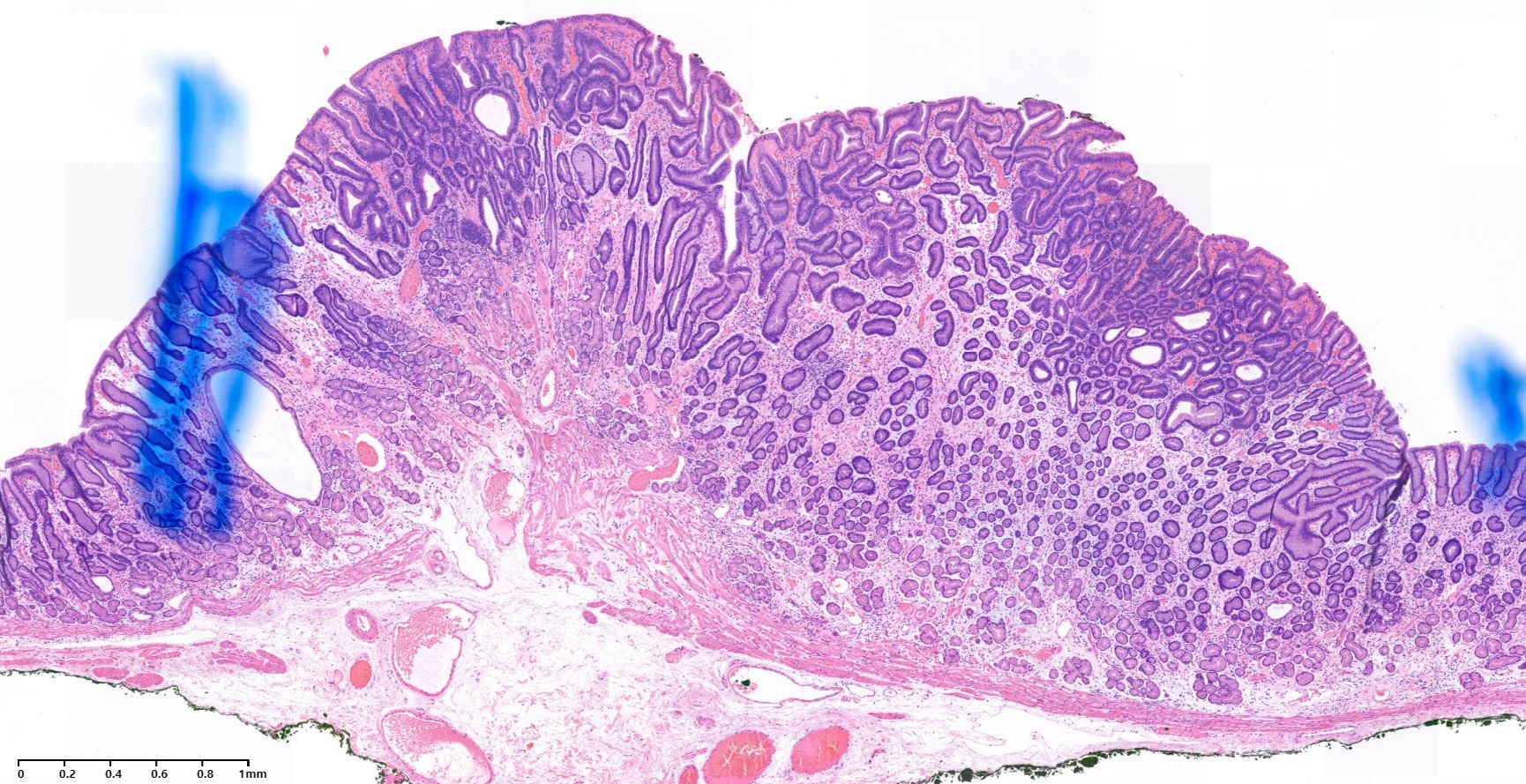
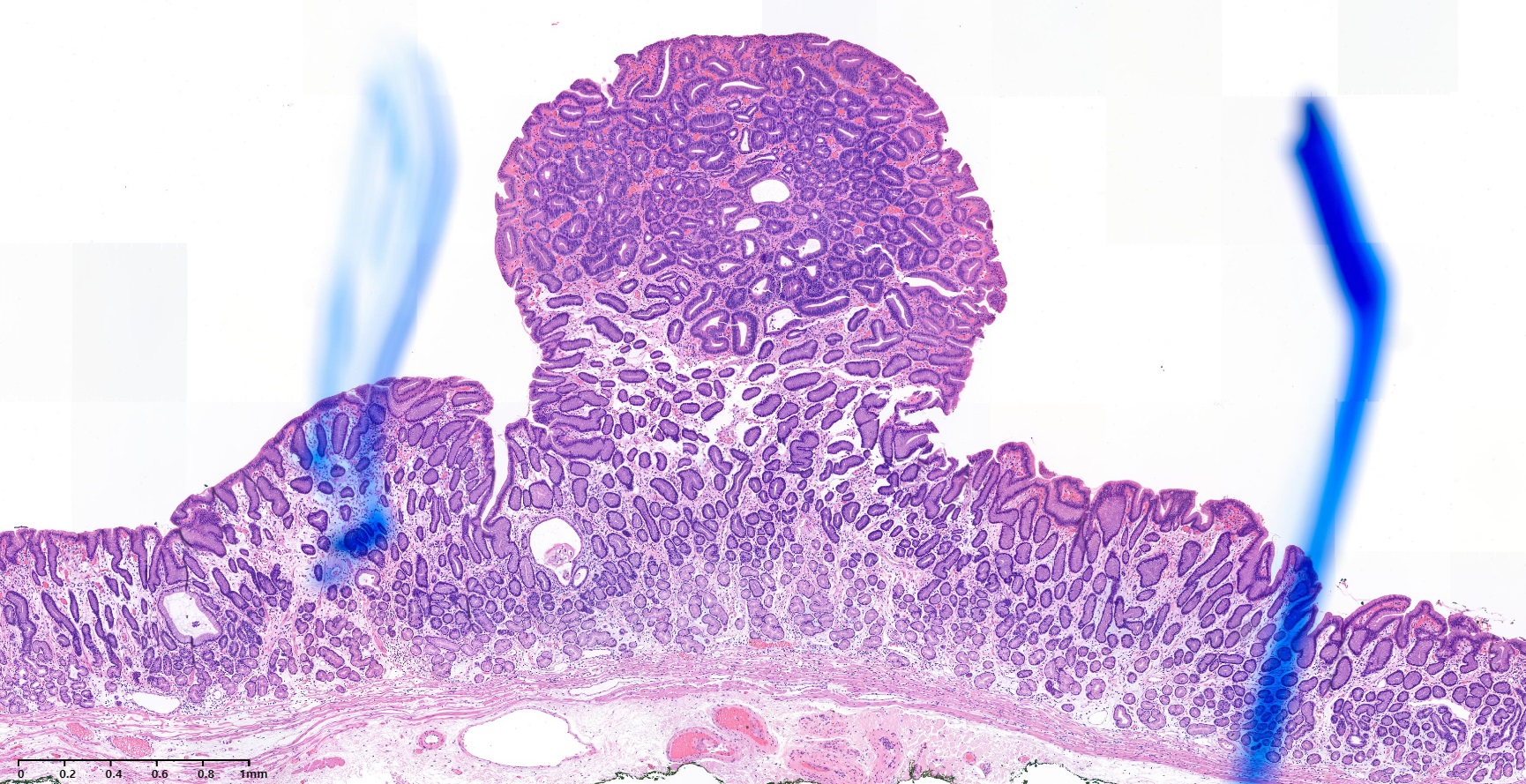
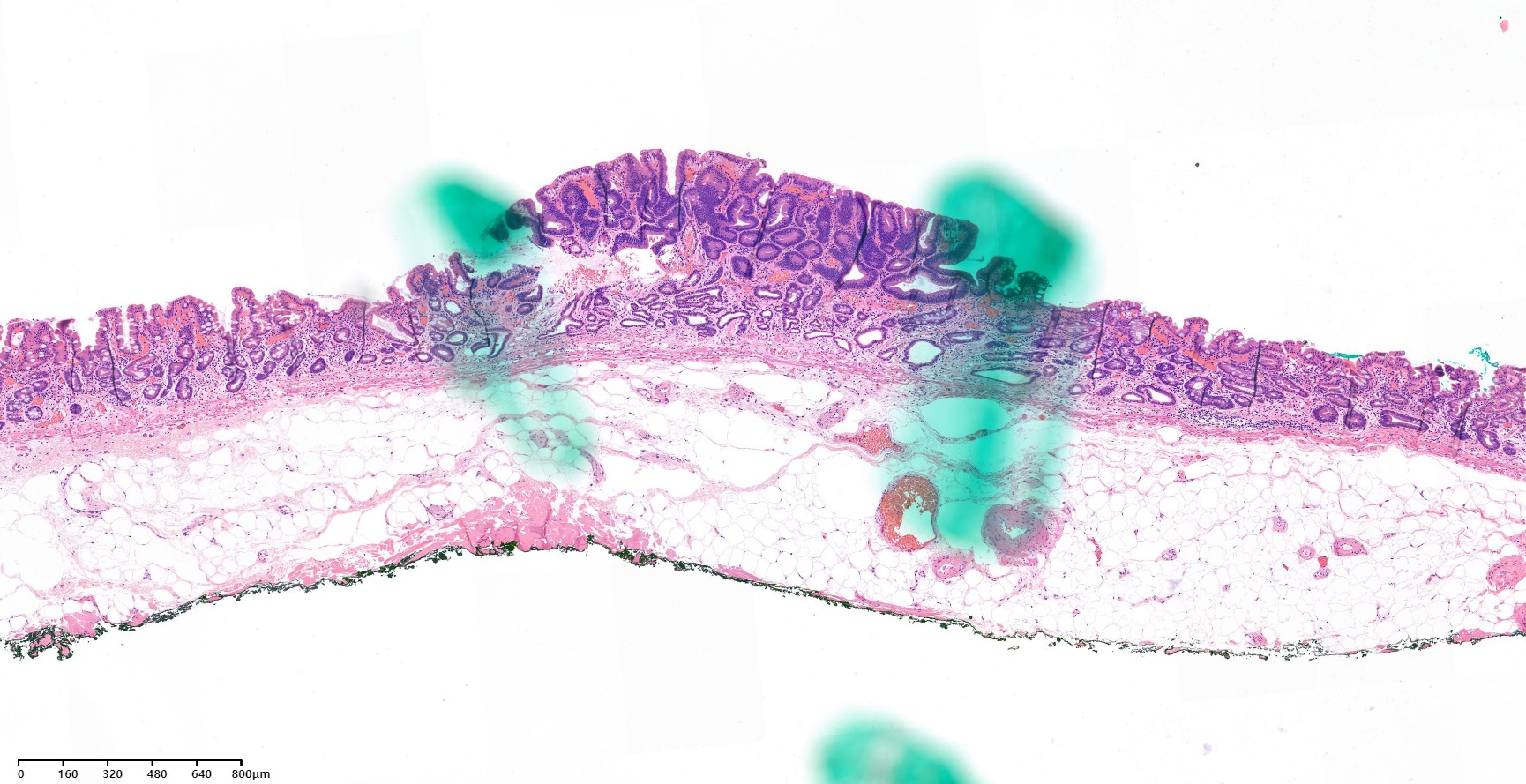
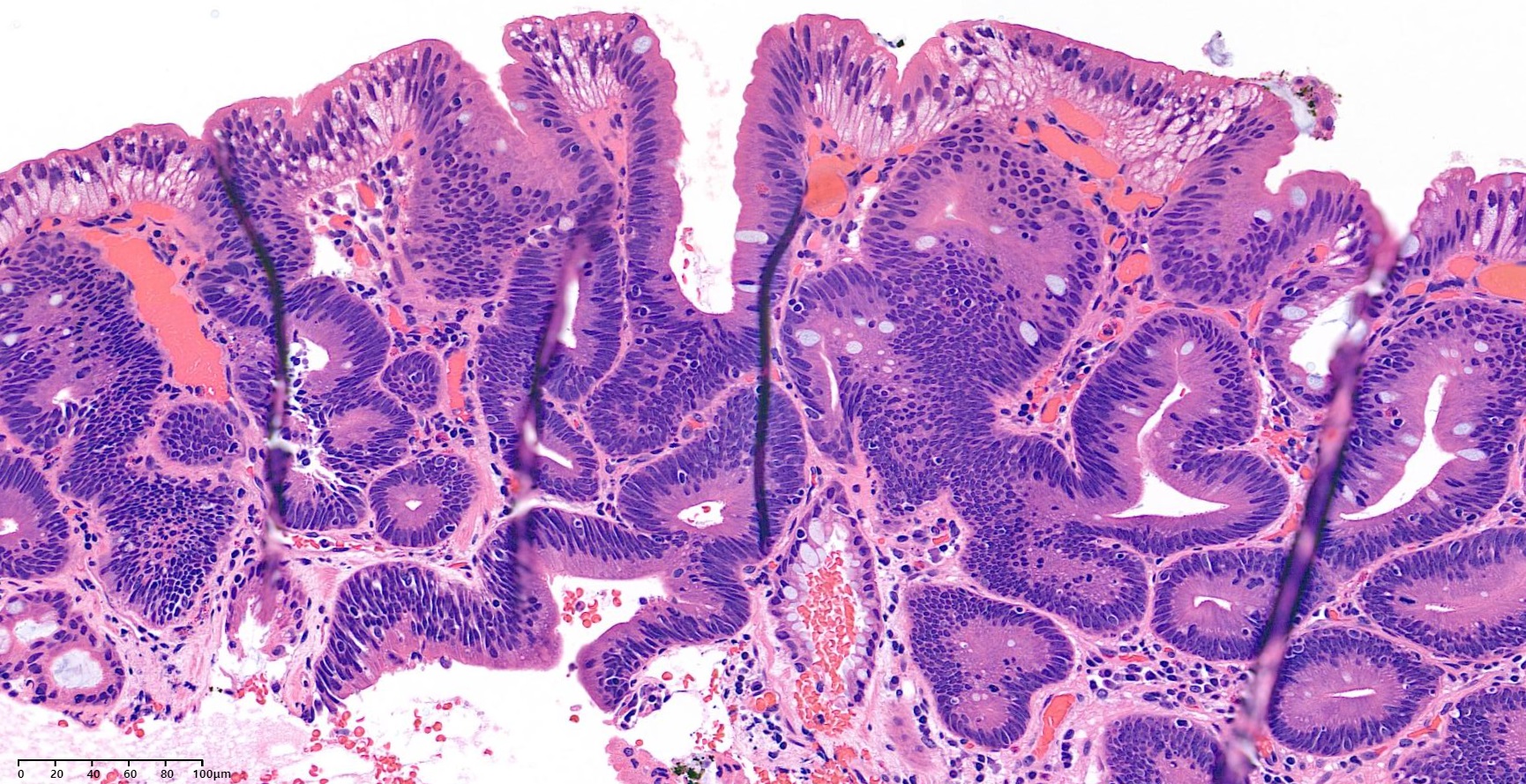
�Ʒ��� ESD �� ���� �������� �ǵ��� ���ʵ��Դϴ�.
adenoma with low grade dysplasia
adenoma with low grade dysplasia
�Ʒ��� 16mm ���������Դϴ�.
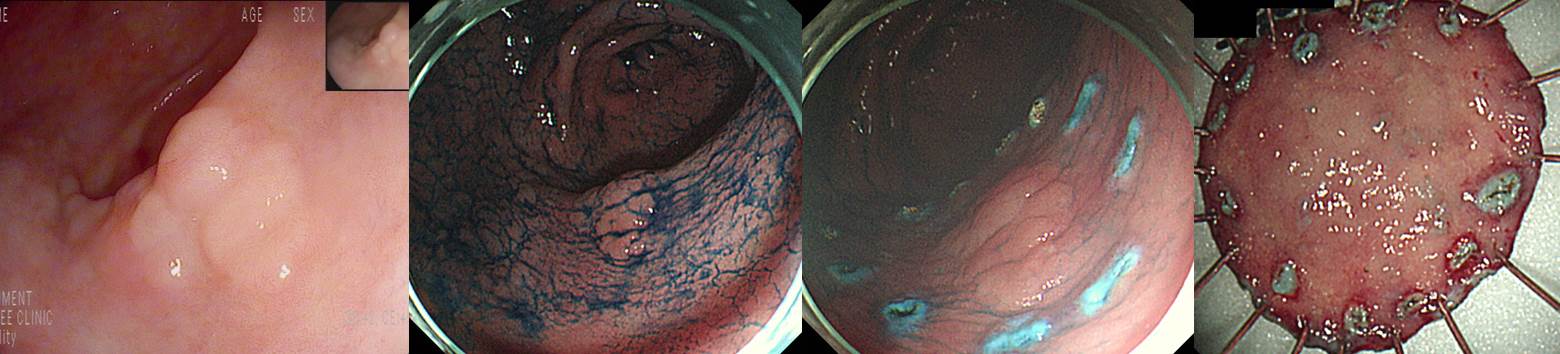
![]() 4. Endoscopic diagnosis. ����/�������� ���ð� ����
4. Endoscopic diagnosis. ����/�������� ���ð� ����
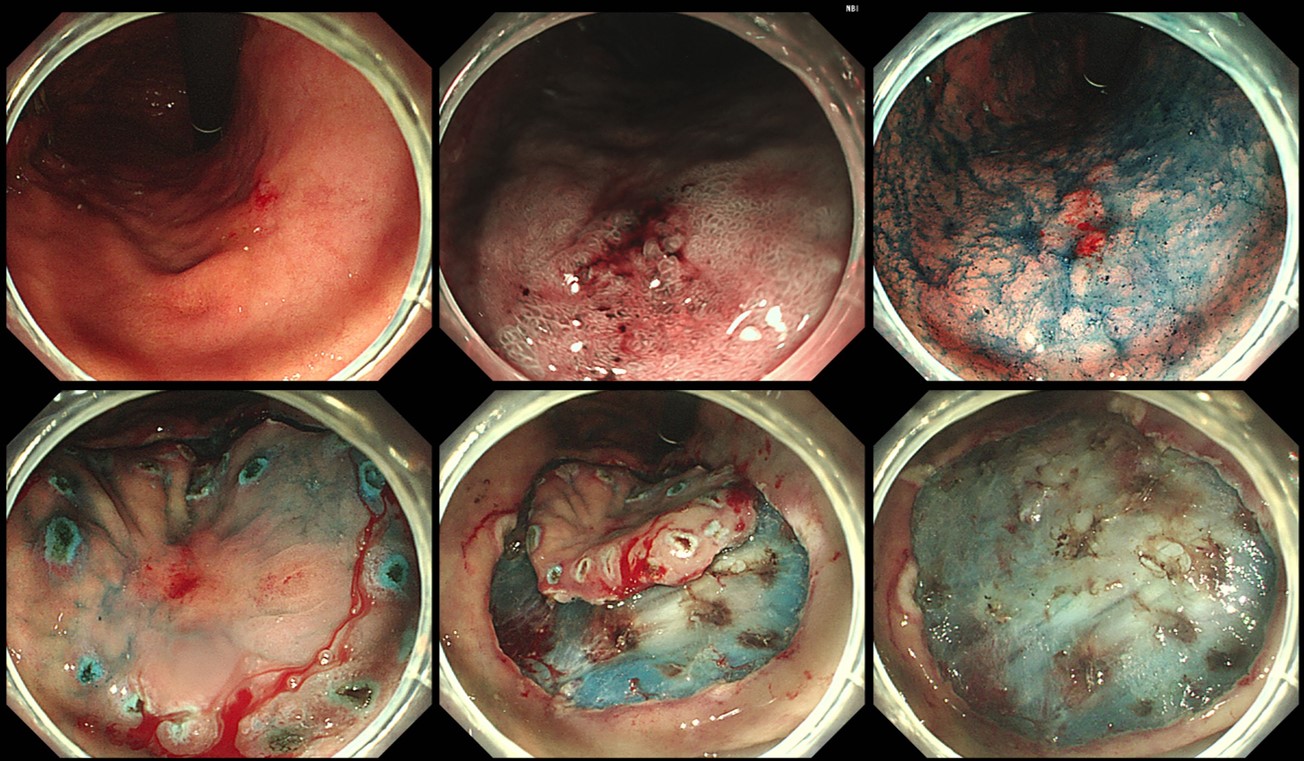
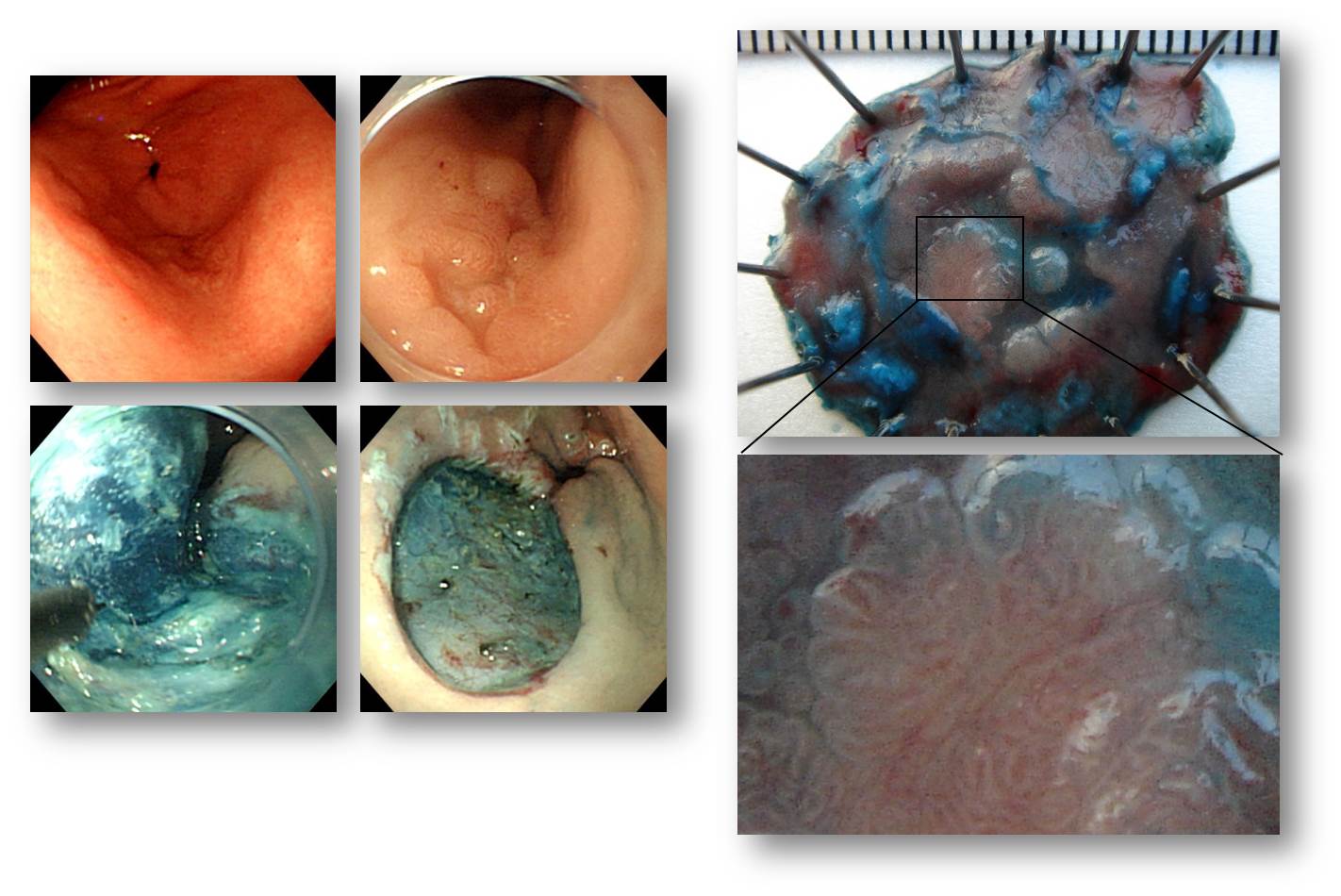
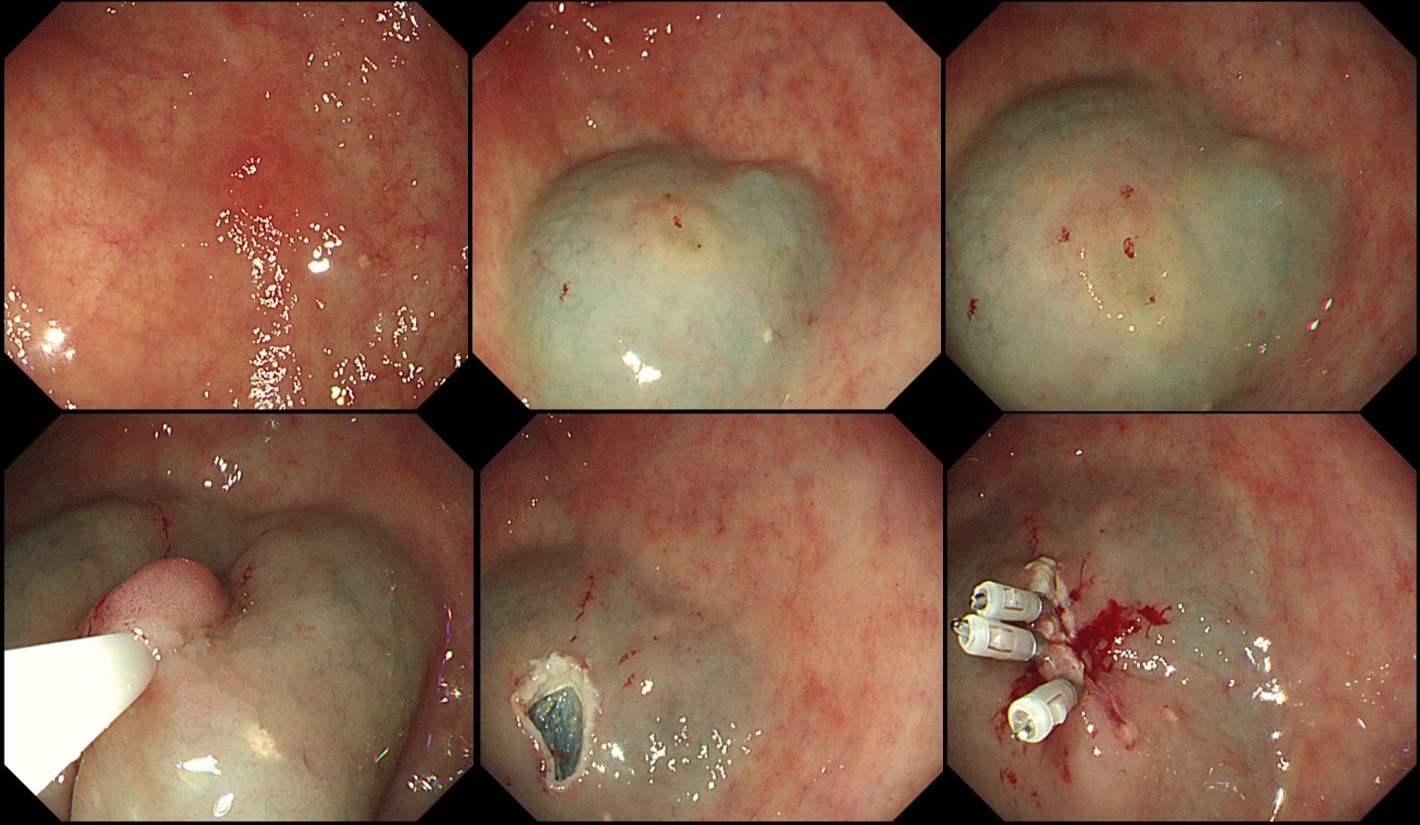
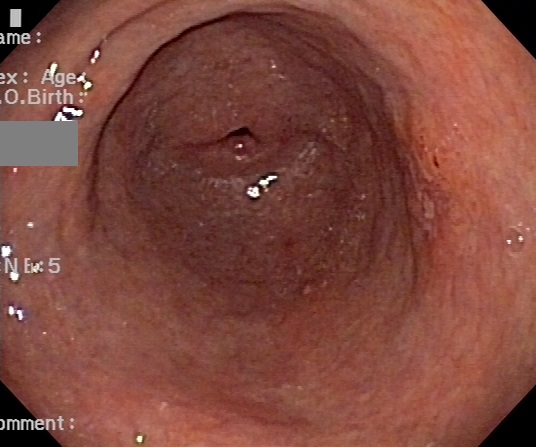
Elevated type adenoma with pseudodepression (ESD pathology: 10 mm low grade dysplasia)
Elevated type adenoma
Elevated type adenoma
80�� ����. �쿬�� �߰ߵ� ���������ε� ��� ġ�Ḧ ��õ�� ���ΰ�? �������, ���ۼ�, ������???
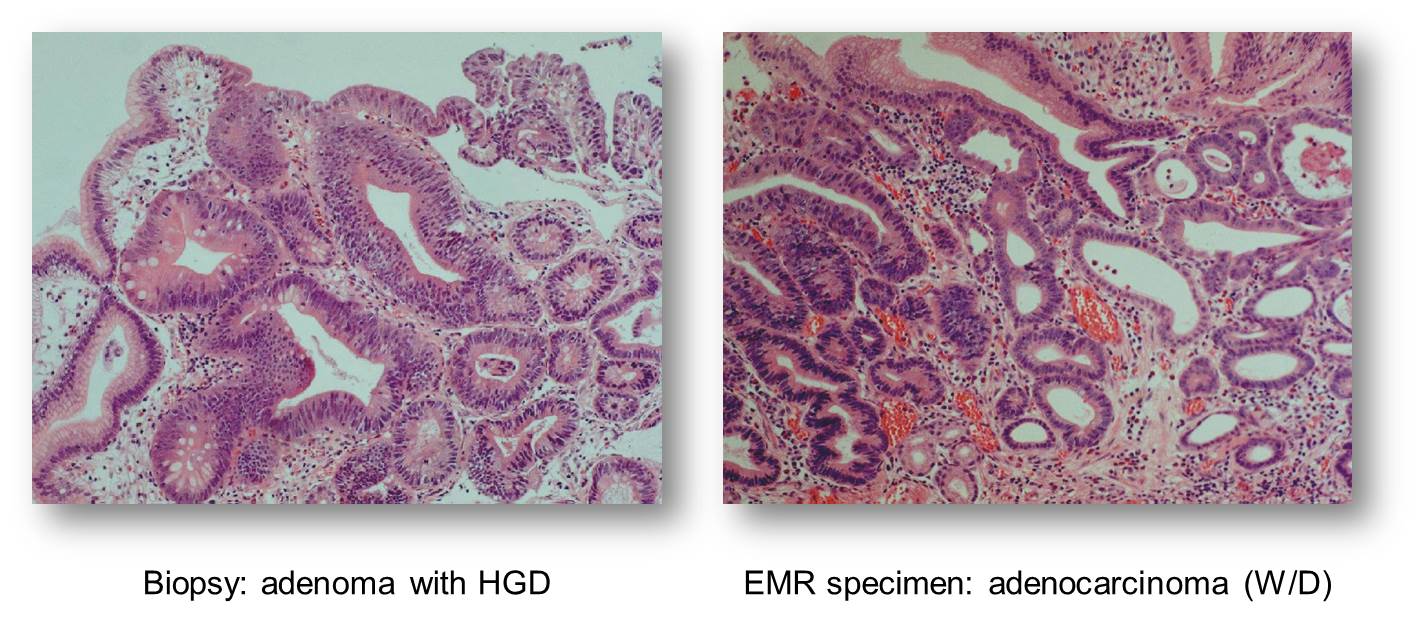
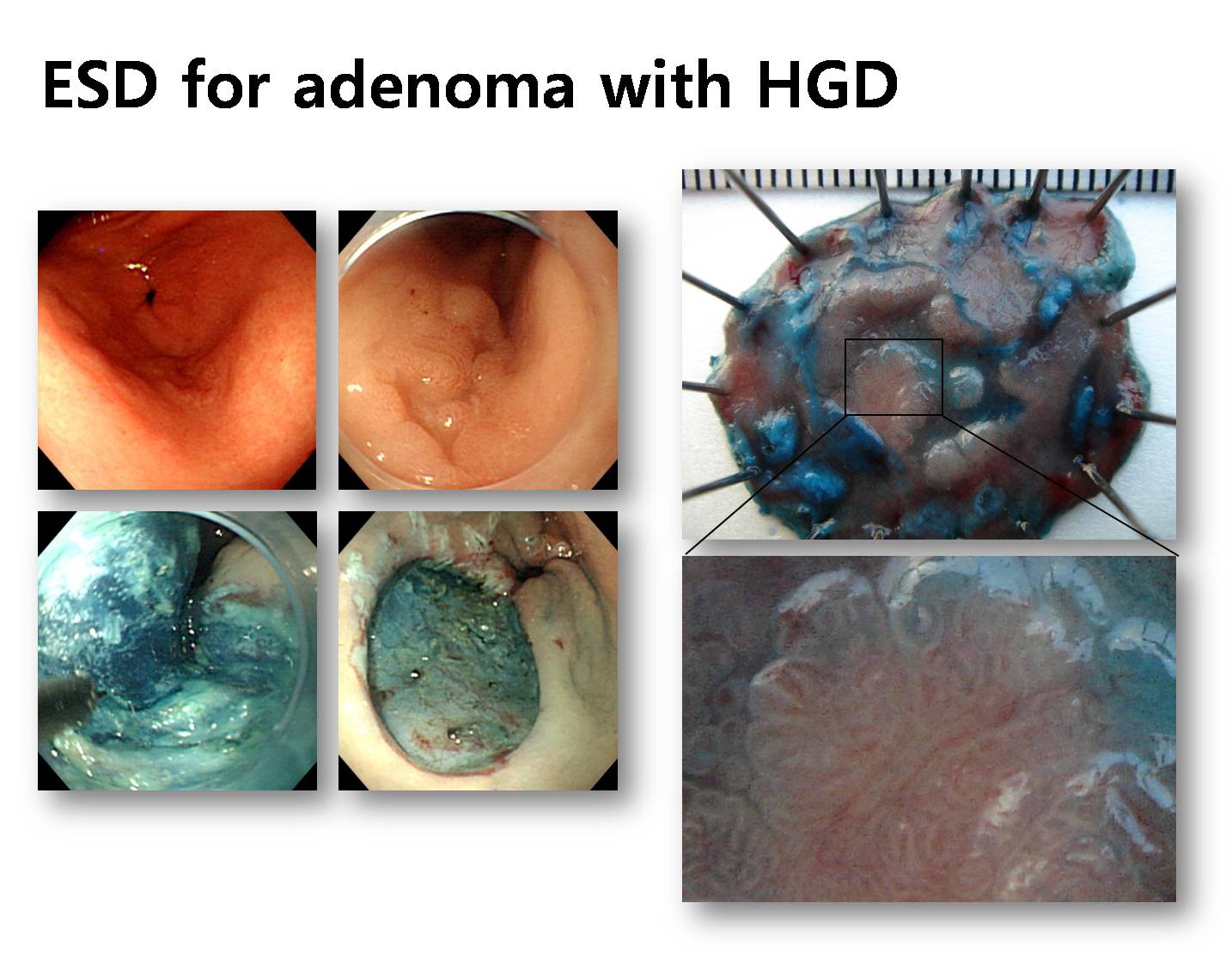
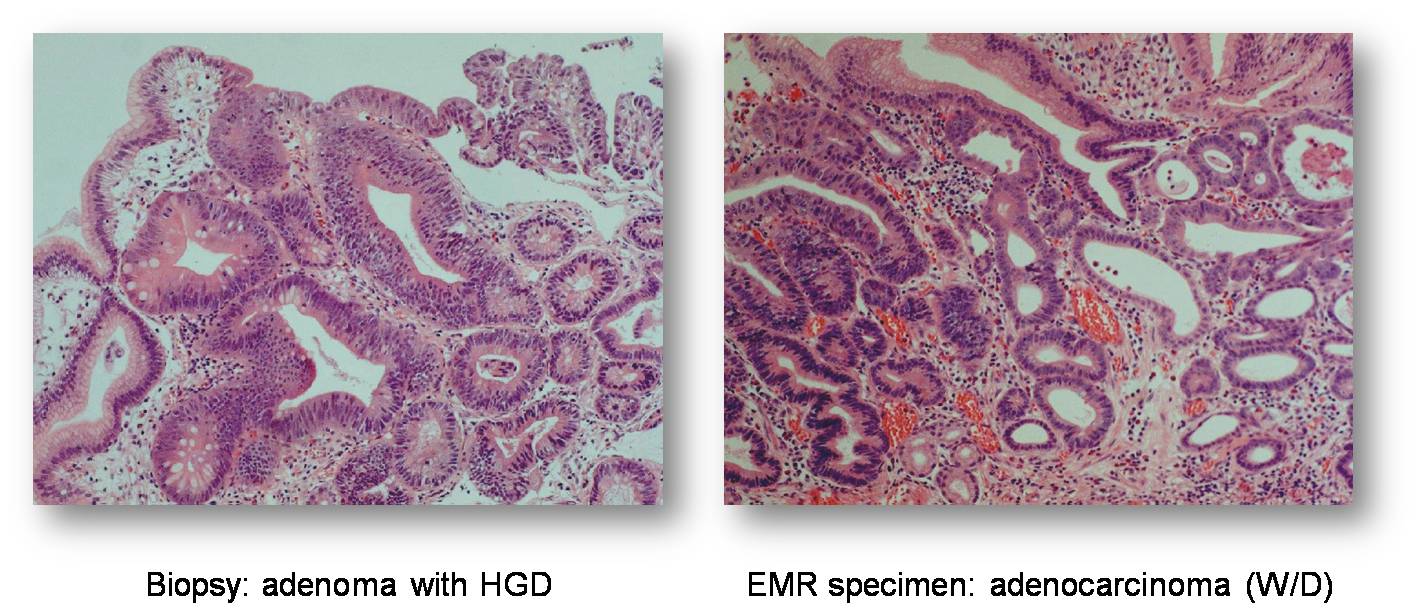
�����˻翡�� adenoma with high grade dysplasia������ EMR �� �������� ������ �ٲ� ��
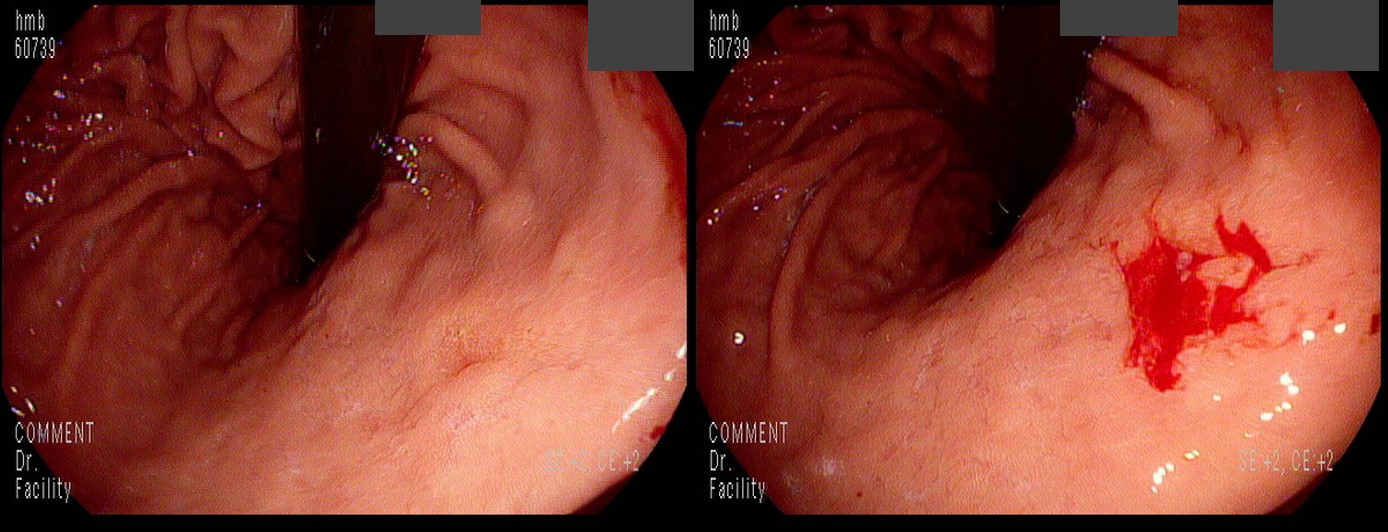
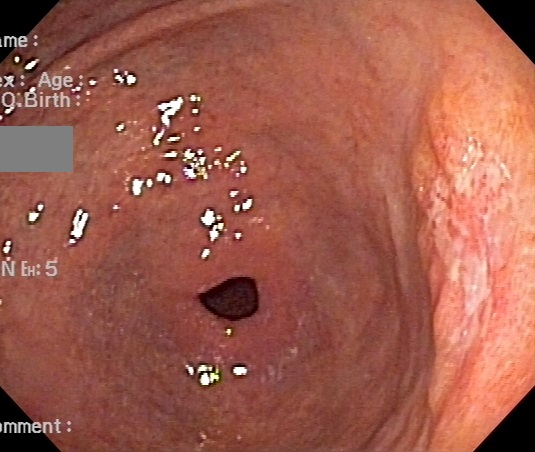
Depressed type adenoma. ���翡���� adenoma��� �θ��� �ʴ´�. flat/depressed type�� ������ ���翡���� dysplasia��� �θ���.
6mm ���� ����
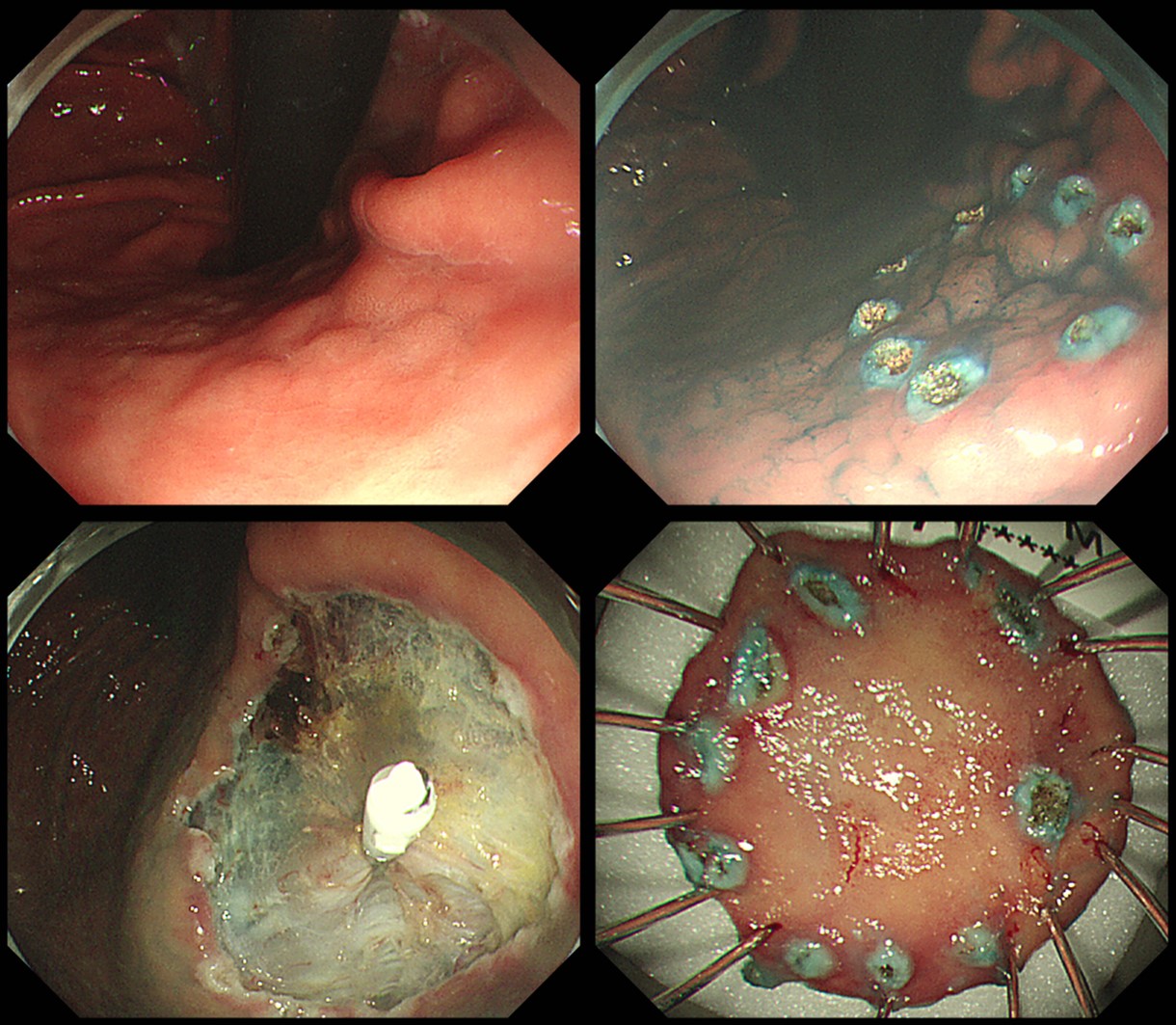
����� ���� ���� ���� �ְڴ� �����Ͽ��� ESD ����� Ȯ���Ͽ��µ� �ǿܷ� 1.4 cm ���� �������� ������.
���������� �ǰڴ� �;��µ� ������������ ���Խ��ϴ�.
Stomach, endoscopic submucosal dissection:
Tubular adenoma with low grade dysplasia
1. Location : angle, lesser curvature
2. Gross type : elevated
3. Size of adenoma : (1) longest diameter, 32 mm (2) vertical diameter, 17 mm
4. Resection margin : negative resection margins(N)
20�и� �������� (ESD was done.)
Ÿ �Ƿ������� ���ð� �� �����˻�� ���ܵ� �����̳� �������� ȯ���� ���ð� ġ�� �� ���ð� ����� �ʿ��ұ��? ù ���ð� ������ �����Ͽ� �˻簡 ������ �̷������ ���ҿ� ���� ��Ȯ�� ������ ������ ������� �ʰ� ��� �ü��� �մϴ�. �� ���� �� ���� �߰� ������ �߰ߵ˴ϴ�. ���ེ���� ù ���ҿ� �߰� ���Ұ� �ſ� ������ �Ѳ����� �����ϱ �մϴ�. ������������ �Ƿڵ� ȯ���Դϴ�. ESD�� �ϱ� ���� �߰� ���Ҹ� �߰��Ͽ��µ�, �� ������ ��ġ�� �ſ� ����� �Ѳ����� ġ���Ͽ��� ���� ��������� �� ���Խ��ϴ�. "Tubular adenoma with high grade dysplasia. (1) 14 x 13 mm, (2) 10 x 8 mm, negative resection margins." ���� ó�� ������ �ڼ��� ���캸�� �ι�° ���Ұ� ����ϰ� �������ϴ� (��� ���� ȭ��ǥ). �Ʒ� ���ʵ� ���� ������ ��쿴���ϴ�. [2017-9-10]
������ �ִ� ���� �ΰ��� �Ѳ����� ġ��
���� �ܰ踦 ���� ������ �Ǵ� �κ��� ��ü ������ �� %���� ��Ȯ���� �ʽ��ϴ�. ��ȭ�� ������ ��κ��� ���� �ܰ踦 ��ĥ ������ �����ϰ� ���� ���Դϴ�. ������ ������ �ڿ��簡 ��Ȯ���� �ʴٴ� ���Դϴ�. 11�� �� adenoma with LGD�� ���ܵǾ���, ���ð� ġ�Ḧ �������� ȯ�ڴ� ���������� ���ϼ̰�, �밭 2�� �������� �� �� �����˻翡�� ��� LGD�� ���Դٰ� 11�� ° �����˻翡�� HGD�� ���Խ��ϴ�. ESD�� �߽��ϴ�. �и� õõ�� ���ϴ� ������ �ֽ��ϴ�.
LC of mid antrum, ESD: Tubular adenoma with high grade dysplasia
1. Location : antrum, lesser curvature
2. Gross type : elevated
3. Size of adenoma : (1) longest diameter, 30 mm (2) vertical diameter, 15 mm
4. Resection margin : negative resection margins(N)
84�� ������ ���� ���ð濡�� �߰ߵ� ���Ҹ� ESD�� ġ���߽��ϴ�. 84������ ������ �ʿ������� �ǹ������� �ϴ� �߰ߵ� ���Ҵ� ġ������ ���� �� ���� ���� �����Դϴ�.
ESD: Tubular adenoma with high grade dysplasia
1. Location : mid body, lesser curvature
2. Gross type : elevated
3. Size of adenoma : (1) longest diameter, 30 mm (2) vertical diameter, 27 mm
4. Resection margin : negative resection margins(N)

ESD: Tubular adenoma with high grade dysplasia
1. Location : antrum, lesser curvature
2. Gross type : elevated
3. Size of adenoma : (1) longest diameter, 25 mm (2) vertical diameter, 24 mm
4. Resection margin : negative resection margins(N)
���� 80�� ���������Դϴ�. ��� ġ���Ͻðڽ��ϱ�? ���� ���ۼ��� ��õ�Ͽ����ϴ�.
�ܺ� �����˻翡�� '�ߵ ������'�̶� �Ƿڵ� ���Դϴ�. �ұ�Ģ�� �Ը��� �����̹Ƿ� ������ ���ɼ��� �ְڴ� �;����ϴ�. ESD�� �Ͽ��µ� �ǿܷ� ���� �������� ���Խ��ϴ�. �˴ٰ��� �� ���� �����Դϴ�. (���� ���ð� ������ contrast�� �ʹ� ���մϴ�. ���ð� �ý����� enhancement�� ����� �մϴ�. Contrast�� ���ϸ� �ϰ� �� ���̴� �� ������ subtle�� ���� ��ȭ�� �� ��ģ�ٰ� ���� �˴ϴ�. ������ ���� �ּ��Դϴ�.)
ESD: adenoma with low grade dysplasia
1. Location : antrum, greater curvature
2. Gross type : elevated
3. Size of adenoma : (1) longest diameter, 18 mm (2) vertical diameter, 13 mm
4. Resection margin : negative resection margins(N)
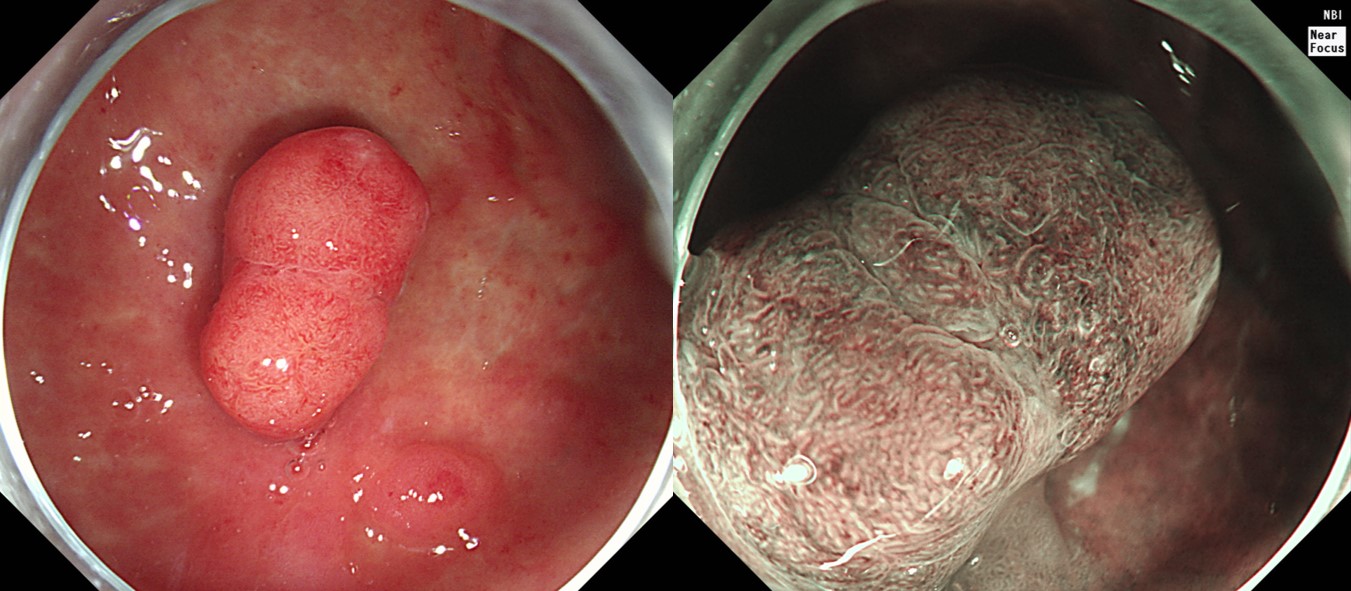
������ ����. Near Focus�� ������ �� ESD�� ���� ����. ���Ⱑ ��� ������ �ƴϾ���
![]() 5. Clinical significance. ����/�������� �ӻ��� ����
5. Clinical significance. ����/�������� �ӻ��� ����
�츮���� �� dysplasia�� �ſ� ���� ���ܵǰ� �ֽ��ϴ� (2018�� 18,717��, �����).
�������� ���� �� �ӻ��� ���ǿ� ���� ������ ���ؼ��� �������� ���������� ���ܰ� �з����� ��Ȯ�Ͽ��� �Ѵ�. ����, �ռ� ����� �ٿ� ���� �������� �������� �з�ü�谡 �ֱٱ����� ����ؼ� �����ǰ� �����Ƿ� ������ ��������� ������ ġ���ħ�� �����ϵ��� �ٽ� �ؼ��ϴ� ���� �ſ� ����� ������ �ǰ� �ִ�.
�������� ���� ���ð� ������������ ������ �� ������ ������ ���� �������� �˻����� �ü� �� �����˻� ����� ���� ���� ������ ������� ���캸�� �������� ���� ġ���Ģ�� ����µ� ������ �ȴ�.
�� ���ǿ��� ���ð� ������������ ������ ȯ���� �ü� �� �����˻� ����� �ü� �� ���������� ��������� ���� ������ ��, ������������ 1.0%���� �ü� �� �������� ������ �ٲ���� ������������ 31.8%���� �������� ������ �ٲ����. �����˻���� ���ð� �������������� �Ⱓ�� ª�� ������ ������������ �������� �����Ͽ��ٰ� �����ϱ� ���ٴ� ó������ ������ �־����� �����˻� �Ұ߸����� ������ ���ܵ��� ���Ͽ��� ������ �Ǵܵȴ�. �ֱٿ��� �������� ���� �����˻��� �ǵ� ���� �����ϸ鼭 ������������ ���ð� ���������� �� �������� ������ ����Ǵ� ��찡 �����ϰ� �ִ�.
�˾��� ������ �������� ??? --> �ᱹ ESD �� 3 cm �������� + 1 cm ������ Ȯ�εǾ����ϴ�. �����˻簡 ���������̴��� ����� �̻��ϸ� ���� �����ؾ� �մϴ�.
[2019-11] ���ð���ȸ���� ��ǥ�� ������ - Clinical outcomes of endoscopic resection for LGD and HGD on gastric pretreatment biopsy: Korea ESD Study Group
Introduction: Some cases of gastric low-grade dysplasias (LGDs) and high-grade dysplasias (HGDs) on forceps biopsy (FB) are diagnosed as gastric cancer (GC) after endoscopic resection (ER). This study aims to evaluate the clinical outcomes of ER for gastric LGD and HGD on pretreatment FB and factors predicting the pathologic upstage to GC. Patients and Methods: Patients who underwent ER for LGD and HGD on pretreatment FB from March 2005 to February 2018 in 14 hospitals in South Korea were enrolled, and medical records for the patients were reviewed retrospectively. Results: 2150 LGD and 1534 HGD diagnosed by pretreatment FB were enrolled. 589 cases of 2150 LGDs (27.4%) were diagnosed with GC after ER. Helicobacter pylori infection, smoking history, tumor location in middle third of stomach, tumor size > 10 mm, depressed lesion, and ulceration significantly predicted GC. 1129 cases of 1534 HGD (72.7%) were diagnosed with GC after ER. previous history of GC, Helicobacter pylori Infection, smoking history, tumor location in upper third of stomach, tumor size > 10 mm, depressed lesion and ulceration were significantly associated with GC. As the number of risk factors predicting GC increased in both LGD and HGD on pretreatment FB, the rate of upstage diagnosis to GC after ER increased. Conclusions; A substantial proportion of LGD and HGD on pretreatment FB were diagnosed as GC after ER. Accurate ER such as endoscopic submucosal dissection (ESD) should be recommended in cases of LGD and HGD with factors predicting pathologic upstage to GC.
[���� 505 - ���� ESD �� �������� ������ �ٲ� ����]
�쿬�� ������ ���� ���ð濡�� ������ �븸�� ������ �߰ߵǾ����ϴ�. �Ƿ� �� �����˻� �ǵ��� "atypical gland proliferation , favoring adenoma, low grade dysplasia"������ �Ƿ� �� �ܺν����̵� ���ǵ� ����� "adenoma, focal high grade dysplasia"�����ϴ�. ǥ���� �ణ �ٸ����� ������ ���� ����ϴٰ� �� �� �ֽ��ϴ�. �ܺ� ���� �������� �ǵ��� �ǿ��ϸ� '���� �����ε� gland�� �ణ atypical�ϴ� (= ���� ���� ġ���� �ణ ���ϴ�)' ������ �� ���̰�, �� ���� ���� �������� �ǵ��� '���� �����ε� focal�ϴ� (= ���� ���� ġ���� �ణ �����ϴ�)' �����Դϴ�. �� �� ��� ���� ������ ���� ������ �߰� �ƴѰ� ������ �ǵ��� �ֽ� ���Դϴ�.
���� ���� ESD �� �������� ������ �ٲ�� ���� 5-10%�Դϴ�. ���� ���� ESD �� �������� ������ �ٲ�� ���� 33%-50%�Դϴ� (EndoTODAY Diagnostic group classification). ���� ������ ���������� �߰� ������� ESD �� ������ ������ �ٲ� ���ɼ��� �� �߰� ������� ���Դϴ�. �뷫 20% ����?
��ü������ 6.9% (141/2,041)�� down-grade �ǰ� 15.9% (324/2,041)�� up-grade �Ǿ����ϴ�. Diagnostic group classification�� ���� �ٲ���ٴ� �ǹ��Դϴ�. (Lee JH. Surg Endosc 2016)
ESD�� �����Ͽ��� ����� �Ʒ��� ���ҽ��ϴ�.
Stomach, endoscopic submucosal dissection:
. Early gastric carcinoma
1. Location : antrum, greater curvature
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 11 mm (2) vertical diameter, 10 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 10 mm, proximal 10 mm, anterior 8 mm, posterior 16 mm
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent���� 4�� 5�� CP(clinical pathway)�� �ü��� ������ ��� �� ��������� ���Խ��ϴ�. ������ �Կ���� ���� �з����� ���Ͽ� CP�� 3�� 4�Ϸ� �ٲ� �ķδ� ��� �� ��������� ������ �ʱ� ������ �ܷ����� ������ �ϰ� �ֽ��ϴ�. ���� �Ʒ��� ���� �����Ͽ����ϴ�. ������ �� ���ɼ��� ����� �˷���ȱ� ������ ȯ�ڰ� ũ�� ���� ���� ���� �����ϴ�.
![]() 6. Treatment. ����/�������� ġ��
6. Treatment. ����/�������� ġ��
�� ����/������(adenoma/dysplasi)�� ���� ġ���� �� ���� �������� ����� �������������� �ֱٿ��� ���� ���Ǵ� ���� ������, ��κ� ���ð��� �̿��� ġ�ᰡ �̿�ǰ� �ֽ��ϴ�. ������ ��쿡 ���ð������������� ��� ��Ⱓ�� �������� ������ �����ϰ� �ü��ڸ��� ���� �ٸ� ġ������ ���ǰ� �ִٴ� �Ѱ�� ������, �������� �����ϴ� �Ϻ� ���������� ��ġ�� ġ����� �ϳ��� �����ǰ� �ֽ��ϴ�.
Ư�� ���ð�������������(ESD: endoscopic submucosal dissection) ����� ���ԵǸ鼭, ���ź��ٴ� �ξ� ū ������ ���� �ϰ������� ���������鼭 ���ð�ġ���� �������� �������� ���Դϴ�. �������� ��쿡�� ��� ���ð� ġ����� �ּ��� ��������� ���� ���ϵ� �ǰ��� ������, ���ð� ġ���� �������� �Ǵ� ���ϰ� ������������ ���������� Ư���� ũ�� �ٸ��� �ʴٴ� �������� ������ ġ����� �����ϴ� ���� �Ϲ����Դϴ�. ����, �������� ���� ���ð�ġ�ῡ �־ �������� �ذ�Ǿ�� �� ���� ������ �����ֽ��ϴ�.
(1) ������������ ���ؼ� ���ð�ġ�Ḧ �õ��ϴ� ���� �Ϲ������� �����ǰ� ������, ������������ ���������� ġ�Ḧ �� ������ Ȥ�� �������ڸ� ������ �������������� ���������� ġ���� �������� ���� ���ǰ� ���ӵǰ� �ֽ��ϴ�. 2014�� ����(�DZ��� �̼���)���� ��� �� �ֵ��� �츮����� �Ϻ��� �������� ���ܱ��� ���̿� ���� ȥ���� ����մϴ�. �� �̽��� ����� ���� 20���� �Ѿ����� ������ ���� �������� ���� �� �����ϴ�. �츮������ �츮���� �����ǻ��� ���ؿ� ���� ġ����� ������ �� �ۿ� ���ٰ� �����մϴ�.
���� ȯ�ڿ��� ���� �����̰� ���ð� �Ұ��� �������̰� pale�� ���� ���ɽ����� ��������� �� �� �ִٰ� �����մϴ�. ���� ���ۼ��� ������ ġ���� �� �ֱ ������...
15�� �̻� ������� ���� ���� ����. ����� ���� �ٲ� ���� ���� �����˻� ������ �ƴѰ� �����Ǿ����ϴ�.
(2) ���ۼ�: ������ ���� ǥ������ ġ����� ���ð� ������������ ��Ȥ ���ð� ���ۼ��� ���ǰ� �ֽ��ϴ� (���ۼ� ). ���� ġ��� ������ ������ ������ �Ҹ�Ȯ�մϴ�. ���ۼ��� �������� ���Ͽ� ���� �����ϸ�, �Կ��� ���� �ʰ� �ܷ����� �����ϱ �ϸ�, �Ƹ��� �ö�� �������ۼ��̶�� ������� ���̵��� ���� ���� ����̹Ƿ� �ֱ� �� �̿� �� �����ϰ� �ֽ��ϴ�. ���� ���ۼ��� ġ���� ������ ���� ������ ���������� ���䰡 �Ұ����ϸ�, Ư�� �Ƹ��� ���� ���ۼ��� ��� ������ �����������ۼ��̳� ���������ۼ��� ���Ͽ� ������ �ı��Ǵ� ���̰� ��ٴ� ������ �����Ƿ�, �������ڰ� ���� ���������� �̿��� ������������ ���� ���ۼ��� �ټ� �����ϴٰ� �����մϴ�.
���� ������ ������ �� ������������ �ٲ�� ���� �ֽ��ϴ�. ���� �۰� �Ͼ�� �����ϰ� �˾��� ���� ���������� �ü� �� ������������ �ٲ�� ���� ���� �����ϴ�. �۰� �Ͼ�� �����ϰ� �˾��� ���� ���������� ���Ͽ� APC ablation�� �� �� �ִٰ� �����մϴ�.
�� ���� ���� �����̸� ���ۼ��� ġ���ϰ� �ֽ��ϴ�.
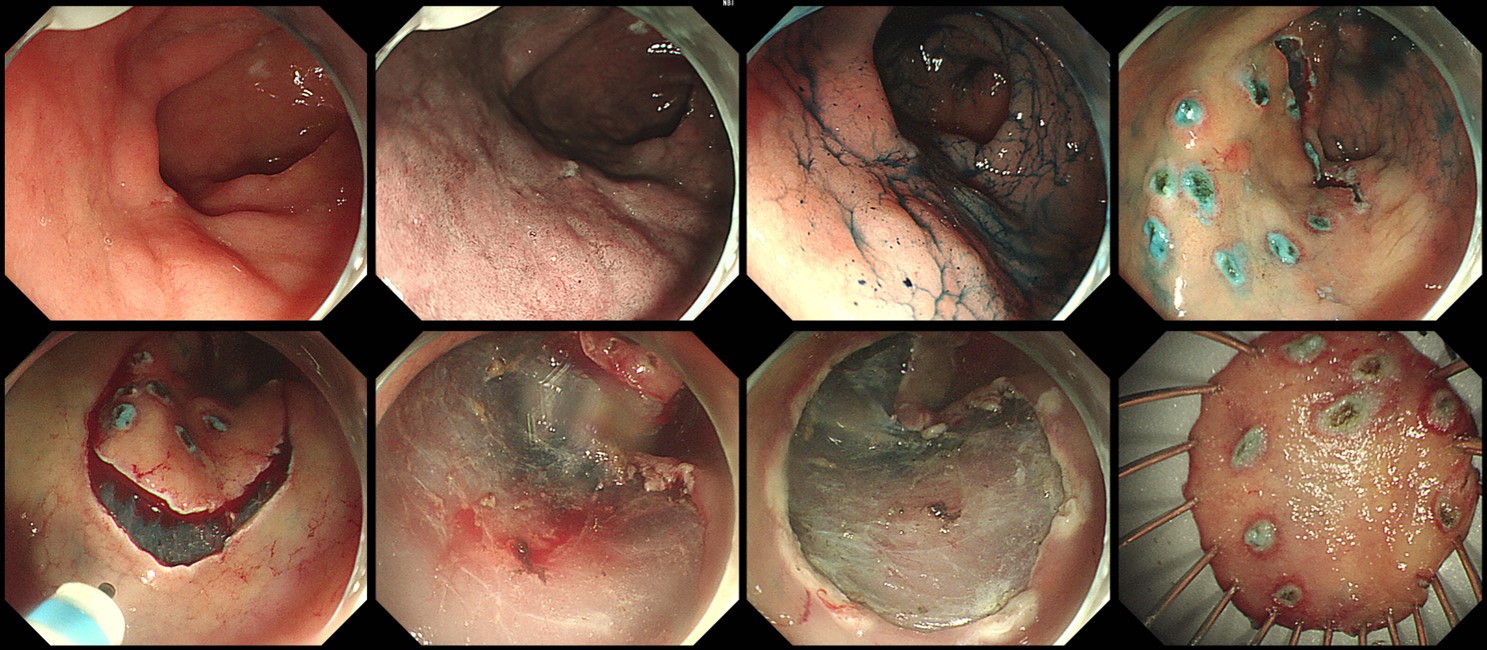
APC ablation for gastric low grade adenoma (�ü� ����� serial�� ���÷��� ���� Ŭ���ϼ���.)
Flat�ϰ� pale�� ������ APC�� ġ�� �� ��� ���� ������� �ϰ� �ֽ��ϴ�. Fujifilm���� ���ܵǾ� �ǷڵǾ��� Olympus�� ġ���Ͽ��� Pentax�� �������� �Ͽ����ϴ�.
���ۼ�(APC ablation)�� ���� ������ ġ��� ���ֵǴ� ������ �ֽ��ϴ�. ��κ� �ܷ� ������� ġ�ᰡ �˴ϴ�. ���� �幰�� ������ �ϴ� ��찡 �ֽ��ϴ�. �������� mucosal destruction�� ũ�� ���� �����Դϴ�. Local control�� �� �ȴٴ� �ǹ��̱ �մϴٸ�... ���� �ü��� �ϱ� ������ �� ���� ������ �����ؾ� �մϴ�.
APC �� delayed bleeding�� ���� ����
2022�� Gut and Liver ���� �ƻ꺴������ APC �� ������ ������ �м��� ������ �־����ϴ� (Gut Liver 2022). �������� 2.4%�����ϴ�. �������� ���� ������ ������ ���̿��� ������ ������谡 �������ϴ�. ������ ������ �������� �����˴ϴ�.
APC �� ���� ���� (Gut Liver 2022)
���� ��κ� �ܷ� ������� ���ۼ��� �����ϰ� �ֽ��ϴ�. ȯ�ڿ����� �Ʒ��� ���� ������ �ϰ� �ִµ� 2%�� �������� �ȳ��ϰ� �ֽ��ϴ�. �Կ�ġ�Ḧ ���ϴ� ������ �ֽ��ϴ�.
[������ ȯ�� ������ 2017�� ���� ���ۼ� �κ�]
"ȭ�������� - ��������(����) - �������� - �������� - ���༺����"�� �ܰ迡�� ������������ ���Խ��ϴ�. ������ �ٹ��ϴ� ������ �־ �������� ���ÿ� �߰ߵǰų�, ó������ �ϳ����µ� ���߿� �� ���� �����̳� ���������� �߰ߵǴ� ���� �����ϴ�. ���� �̹��� �� ġ���ϴ� �͵� �߿�������, ������̰� �������� �˻簡 �� �ʿ��մϴ�. ���� 1� �ѹ� ���ð� �˻縦 ��õ�մϴ�.
������ ���� ġ����� ��������� �ϴٰ� ���� �Ǵ� �и� ���������� �Ͽ����ϴ�. �ֱٿ��� �̸� ���ð�ġ�Ḧ �մϴ�. �� ���� ġ����� �ֽ��ϴ�. �������� ���� ġ���� �� �ְ� ���������� ��Ȯ���� �� �ִٴ� ������ �ֽ��ϴ�. ������ �Կ��� �ʿ��ϰ�, �պ��� ���赵 �����ϴ�. ���ۼ��� ���� �Կ��� �ʿ����� �ʰ� ���� �����ϰ� ���� ������ ġ���� �� �ֽ��ϴ�. �۰� ������ ���������� �ַ� ���ۼ��� ġ���ϰ� �ֽ��ϴ�.
���ð� �ü� �� 1�ð� ���� ȸ���ǿ��� ������ ���� �� ����ϰ� �˴ϴ�. �ü� 2�ð� �� (= ��� 1�ð� ��) ���̳� �����(����, ������ ����)�� ���ð�, �ü� 3�ð� �� (= ��� 2�ð� ��) �ε巯�� ���� ��ʽÿ�. ���� �� ��ħ�� ���� ��ŵ� �����ϴٸ� �ܴ��� ������ ���Ͻʽÿ�. ���� 2�ְ� �Ϸ� �� �� ��ħ ������ �����Ͻʽÿ�. �Ͱ� �� ���������� �ֽ��ϴٸ�, �� �� 2% �����Դϴ�. �� ��� ������ �ֽðų� ������ ã���ֽʽÿ�. ��ĥ�� �ణ ���� �� �ֽ��ϴ�. ����(����)���ð� �� ������ ���� �������� ���ð�, ��ȣ�ڿ� �Բ� �Ͱ��Ͻñ� �ٶ��ϴ�.
�����̳� �������� �ִ� �п��� ������̳� ���� ������ �� ����ٰ� �մϴ�. ���� ���� �˻縦 ���� �����̴ٸ� ���峻�ð� �˻縦 �� �ƺ��ʽÿ�.
���ۼ��� ��κ� ���� ������ ���������� ��ġ�� ȯ���� ������ȯ ���� �����Ͽ� ���� ������ ���ۼ��� ġ���ϴ� ��찡 �ֽ��ϴ�. ���� �ʽ��ϴ�.
2024�� 6�� �ƻ꺴�� ������ ���ð� ���ۼ��� ���� ��簡 �־����ϴ�.
![]() [2025-7-21] �︮�ڹ�����ȸ���� ���� ���� ġ�� ��Ȳ�� �����Ͽ� ��ǥ�Ͽ����ϴ�. (https://doi.org/10.7704/kjhugr.2025.0021) �� �������� �츮���� �ǻ���� aggressive�� ġ�Ḧ �ϰ� ��ô� ����Դϴ�. ġ���� ��� �ǿ� ���� ����� ������ �ʿ��ϴٰ� �����մϴ�.
[2025-7-21] �︮�ڹ�����ȸ���� ���� ���� ġ�� ��Ȳ�� �����Ͽ� ��ǥ�Ͽ����ϴ�. (https://doi.org/10.7704/kjhugr.2025.0021) �� �������� �츮���� �ǻ���� aggressive�� ġ�Ḧ �ϰ� ��ô� ����Դϴ�. ġ���� ��� �ǿ� ���� ����� ������ �ʿ��ϴٰ� �����մϴ�.
(3) ������: ������ �� �������� ���� �����̰��� ���� �����̶� ũ�Ⱑ ū ���, �Ը��ΰ� �ִ� ��� ����� �������� ����ǰ� �ֽ��ϴ�. ESD�� ���� ���� ��������� �������� ������ EMR�� ����DZ �մϴ�. ���� ���� ESD�� ��ȣ�ϰ� �ֽ��ϴ�.
Stomach: Posterior wall of low body, ESD: Tubular adenoma with low grade dysplasia
1. Location : low body, posterior wall
2. Gross type : elevated
3. Size of adenoma : (1) longest diameter, 9 mm (2) vertical diameter, 8 mm
4. Resection margin : negative resection margins(N)
���������̶� ũ�� �������� ġ���ؾ� �մϴ�.
���������� ũ��� �����ϰ� �켱������ �������� �����ϴ� ���� �����մϴ�.
�������� ���ð�ġ�Ḧ �����ϴ� ȯ�ڿ� ���� � �������� ������ (2018). ������ ������ upgrade �� Ȯ��, ������ �ʿ��ϴٴ� ����� ���� Ȯ��, �̼Ҽ� ������ ���迡 ���� ������ �� �Ǿ� �ֽ��ϴ�.
�����ź������� ���� ���� ȯ���� KT workup ���� �߰ߵ� ���������� ���� ESD.
Stomach, endoscopic submucosal dissection:
Tubular adenoma with high grade dysplasia
1. Location : prepyloric antrum, posterior wall
2. Gross type : depressed
3. Size of adenoma : (1) longest diameter, 12 mm (2) vertical diameter, 5 mm
4. Resection margin : negative resection margins(N)
���� �ǽ����� �����˻縦 �Ͽ� ���������� ������. EUS���� SM invasion �ǽɵȴٰ� �Ͽ� �� 4���� �����˻縦 �Ͽ��µ� ������ ������ �ʾ� ���ܸ����� ESD�� �����Ǿ� �Ƿڵ�. �Ʒ� ������ ���� �ü��Ͽ���. (2018��, ���� 60��)
ESD: Tubular adenoma with high grade dysplasia
1. Location : body, anterior wall-lesser curvature
2. Gross type : flat
3. Size of adenoma : (1) longest diameter, 16 mm (2) vertical diameter, 14 mm
4. Resection margin : negative resection margins(N)
���� ������ �����ε� �����˻翡�� high grade dysplasia�� ���� ESD�� �Ͽ��� 6mm HGD�� ���� ��� (�Ʒ� ���� ���� ����)
(4) �� ġ���� �Ϲ����� ��Ģ�� ���� ���������� ��쿡�� �ټҰ��� ���輺�� �ִٰ� �ϴ��� �ϰ������� ���Ͽ� ����ϴ� ���� ����ȭ�� �� �ֽ��ϴ�. ���� �������� ȯ�ڿ����� ���ð�������������(ESD)�� ���� �������� ġ�Ḧ ���Ͽ� ����� �������� Ȯ���ϸ鼭 �ϰ������� �� �� �ִ� �ü����� �θ� �̿�ǰ� �ֽ��ϴ�. ���� ������������ ������ Ȯ�ε��� ���� ������ ������ ���ؼ��� ���������� ġ�ῡ ���Ǵ� ��� ����� �����ϰ� ����Ǿ�� �ϴ����� ��Ȯ���� �ʽ��ϴ�. ESD ������ ���� �ü��ڴ� ���� ���� ������ ESD�� ġ���ϴ� �����̰�, ESD �ʽ��ڴ� ���� ū ���ҵ� EMR�� ġ���ϴ� �� �ü����� ���迡 ���� ġ���� ���ÿ� ���̰� �ֽ��ϴ�. ���� �ǻ���� �ڽ��� ����� �İ��� �������� �ּ��� ġ����� �����ϵ��� ���뼺�� �����ϴ� ���� ���� ������ �����մϴ�. 2018�� �� ������ ESD ���ؿ����� 1.5cm ������ ������ ���� ESD�� �������� �ʰ� �ֽ��ϴ�. �ǻ��� ġ��� ���� ������ ũ�� �����Ű�� �ִ� ���� ���� �����̹Ƿ� ���� ����Ǿ�� �մϴ�. 1.5cm ������ ���� ESD �� ������������ ���� ���� ���� ������, �� �� �Ϻδ� ù �����˻翡�� ���� �����̾����ϴ� (�Ʒ� ���� ����). 2018�� �� ������ ���ؿ� ���� EMR�� ġ���Ͽ������ �ټ� ġ�ᰡ ������Ͽ��� ���ɼ��� �ֽ��ϴ�.
���� ���� ESD �� �������� ���������� ����.
Stomach, endoscopic submucosal dissection:
Early gastric carcinoma
1. Location : proximal antrum, postero-greater curvature
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 10 mm (2) vertical diameter, 8 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N) - safety margin : distal 6 mm, proximal 5 mm, anterior 8 mm, posterior 8 mm
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
(5) ���������� ���ð�˻簡 �����ϰ� �ǰ������� �� �а� ����ǰ� �ֱ� ������ �������� �� �����Ƿ������� ���ð�˻縦 ���Ͽ� �������� ���ܵǴ� ��찡 �ð� �ֽ��ϴ�. ���� ��κ��� �������� ���� ���⼺ Ȥ�� �Ը��� �����̹Ƿ�, ù �˻���� �ڼ��� ������ ������ ������ �ٽ� ������ ���ð� �˻翡�� ��Ȯ�� ������ ��ġ�� ã�� ���ϴ� ��찡 ���� �� �ֽ��ϴ�. �������� ġ�Ḧ ���Ͽ� �ǷڵǾ����� ���Ҹ� ã�� ���� ��쿡 indigocarmine�� ���� ���Ҹ� �����ϸ� ������ �ȴٴ� ���嵵 ������, �������༺ ������ ���Ͽ� ǥ���� ��ź���� ���� ������ ���������� �ڼ��� �����Ͽ� �߰ߵ��� �ʾҴ� ������ ������ ������ ������ �Ƽ� �߰��ϴ� ���� �ſ� ����� ���Դϴ�. ���� �������� ȿ������ ���ð�ġ�Ḧ ���ؼ��� ù ���ð� �˻翡�� �߰ߵ� ������ ��ġ, ũ��, ����� ��Ȯ�� ����ϴ� ������ �ʿ��ϸ�, ȯ�ڸ� �Ƿ��� ������ ������ ���������� �Բ� �ڼ��� �ڷḦ �Բ� ������ ���� ����� �ʿ��մϴ�.
(6) ���ð� �ü��ǿ� �����ǻ���� Ȱ���� �ǰ߱�ȯ�� �߿��� ������ �ϳ��Դϴ�. ������ �����̸� ���߷��� �پ��� �õ����� �ұ��ϰ� ������ ������ �Ϻ��� �������ڵ��� ������ �������� ���ϰ� �������� ������ ������ ���� ���ϴٴ� �� �Ϲ����Դϴ�. ���������� �̿� ����� �� �̷�����ٸ� ȯ���� ���ܰ� ġ�ῡ ũ�� ������ �� ������ �����ȴ�. ���ð� �ǻ�� ���� �Ұ߿� ���Ͽ� ��� ������ ���ذ� �־�� �մϴ� (EndoTODAY ����� ����).
![]() 7. Cancer after ESD for adenoma with high grade dysplasia
7. Cancer after ESD for adenoma with high grade dysplasia
�ü� �� �����˻�: ��������
Stomach, ESD :
Early gastric carcinoma
1. Location : proximal antrum, lesser curvature
2. Gross type : EGC type IIa+IIc
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 52 mm (2) vertical diameter, 19 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N); safety margin : distal 9 mm, proximal 9 mm, anterior 8 mm, posterior 10 mm, deep 1800 ��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
���� 643
Cardia, ESD: Early gastric carcinoma
1. Location : cardia, lesser curvature
2. Gross type : EGC type IIb
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 20 mm (2) vertical diameter, 13 mm
6. Depth of invasion : invades mucosa (muscularis mucosa) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 6 mm, proximal 2 mm, anterior 10 mm, posterior 12 mm, deep 900 ��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
���� �������� ESD �� �������� ���������� ����.
- Histologic type : tubular adenocarcinoma, moderately differentiated
- Size : 1.6x0.7x0.05 cm
- Depth of invasion : invades mucosa (muscularis mucosa) (pT1a)
- Resection margin: free from carcinoma (safety margin: distal 1.2 cm, proximal 1 cm, anterior 1.4 cm, posterior 1.4 cm)
- Lymphatic invasion : not identified
- Venous invasion : not identified
High grade dysplasia��� �����˻� ����� �Ƿڵ� ȯ���Դϴ�. Olympus ���ð��̾����ϴ�. ���� �Ը��� ������ ũ��� ��踦 ���캸���� �� ������ ���ɼ��� ���ٰ� �ǴܵǾ����ϴ�.
ESD�� �����Ͽ����ϴ�. Pentax ���ð��̾����ϴ�.
ESD: Early gastric carcinoma
1. Location : antrum, lesser curvature-posterior wall
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 20 mm (2) vertical diameter, 15 mm
6. Depth of invasion : invades mucosa (muscularis mucosa) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 7 mm, proximal 9 mm, anterior 8 mm, posterior 24 mm, deep 800 ��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
13. Associated finding: Gastritis cystica
������������ �ǷڵǾ� ESD �Ͽ��� 4mm LP ������ ����
�� ȯ���� ����
�� ȯ���� ����
![]() 8. Cancer after ESD for adenoma with low grade dysplasia
8. Cancer after ESD for adenoma with low grade dysplasia
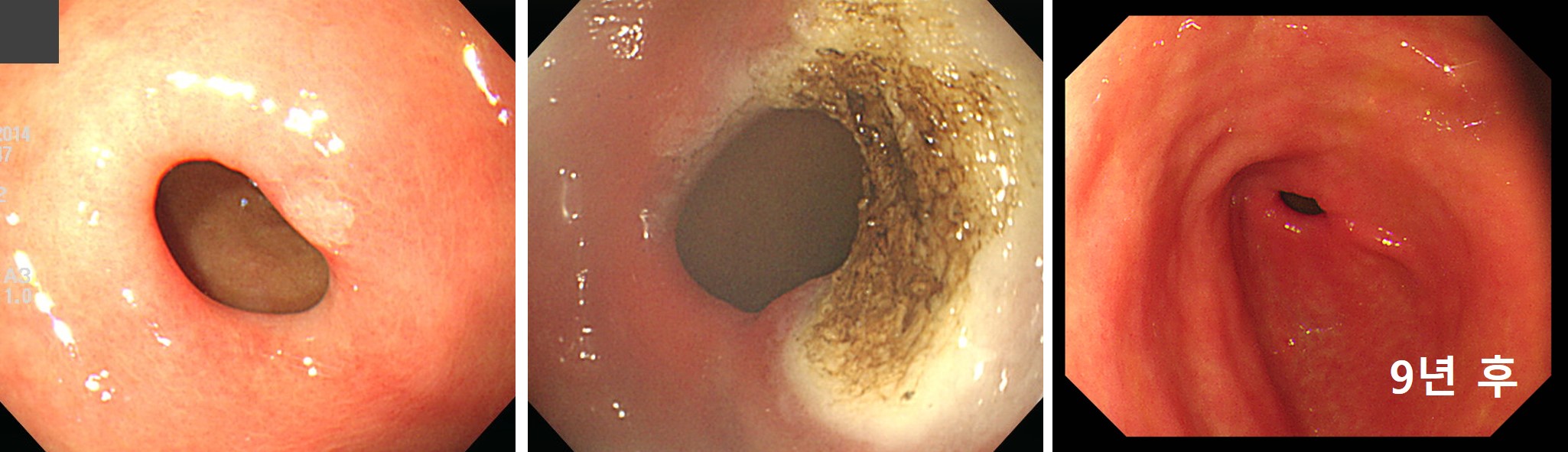
�ǰ��������� �쿬�� �߰ߵ� r/o EGC�� ���Ͽ� �����˻縦 �����Ͽ� adenoma with low grade dysplasia�� ���� 1�� �� �������ð� �����˻翡�� �������� ���� �Ƿڵ� ȯ���Դϴ�. ���Ҵ� ������ �Ҹ��� angle ���Ϻο� ��ġ�ϰ� �־��� ESD�� �����Ͽ� complete resection�̶�� ���� ����� ������ϴ�.
���ȼҰ߿��� ������ �ǽɵǾ��� �����˻翡�� adenoma�� ���� ��쿡�� (1) short-term follow up�� �ϰų� (2) ���ð��� �������� ������ �� �ֽ��ϴ�. Short-term follow up���� ���� ������ ������ ��������, ���� ������ �ʴ� ���� ġ���ħ ������ ��ȣ���� �� �ֽ��ϴ�. ���� ���� �ָ��� ����� ���� �� �ִ� short-term follow-up���ٴ� ���� Ȯ���ϰ� ���������� �� �� �ִ� ���ð��������� ��ȣ�ϴ� ���Դϴ�. ��� ������ ESD�� �ʿ�� ������ ���ȼҰ� ���������� �ǽɵǴ� ��쿡�� ESD�� ������ �� �ִٰ� �������ϴ�.
���� ���� ESD �� ������ ������ ���� ���� ���Ƽ� (33-50%), ���� ���� ESD �� ������ ���� ��츦 �߽����� �� ���ʸ� �Ұ��մϴ�.
���� ���� ESD �� �������� ���������� ����.
ESD: Early gastric carcinoma
1. Location : antrum, greater curvature
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 10 mm (2) vertical diameter, 6 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 12 mm, proximal 12 mm, anterior 14 mm, posterior 12 mm, deep 500 ��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
���� �������� �Ƿڵ� ���Դϴ�. ��� �ܺ� ������ �ſ� ���������, ���ȼҰ��� ���� + �Ը������� �ɻ�ġ �ʴٰ� �ǴܵǾ����ϴ�. ESD �Ͽ��� ���� ������ ���Խ��ϴ�.
ESD: Early gastric carcinoma
1. Location : angle
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 18 mm (2) vertical diameter, 7 mm
6. Depth of invasion : invades mucosa (muscularis mucosa) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 17 mm, proximal 7 mm, anterior 10 mm, posterior 12 mm, deep 1500 ��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
���� ���� ESD �� ������ �ʿ��� �������� ������.
Stomach, endoscopic submucosal dissection:
Early gastric carcinoma
1. Location : low body, posterior wall
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 36 mm (2) vertical diameter, 22 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion :800 ��) (pT1b)
7. Resection margin : safety margin : distal 2 mm, proximal 5 mm, anterior 2 mm, posterior 2 mm, deep < 50 ��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
���� ���� ESD �� ������ �ʿ��� �������� ������ (2016)
Stomach, ESD: Early gastric carcinoma
1. Location : low body, lesser curvature
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 24 mm (2) vertical diameter, 14 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion : 750 ��) (pT1b)
7. Resection margin : free from carcinoma(N); safety margin : distal 7 mm, proximal 5 mm, anterior 12 mm, posterior 4 mm, deep 150 ��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
������ ���� conventional endoscopic resection �� ���� ������ ��찡 ���� �����ϴ�. ���� ���� ��쿡 resection margin�� ������� ���Ͽ� 'ó������ ESD�� �ߴ���� �� �������ٵ�'��� ��ȸ�ϰ� �˴ϴ�. 2020�� ���� 1.5cm�� �� �Ǵ� ���������� ESD�� �� �� ���� ������ conventional EMR�� ����Ǵ� ��찡 �����ϴ�. ������� ����� ������ ��쵵 ���� ������... ȯ�ڸ� ���� �ּ��� ���Ḧ �� �� �ִ� ȯ���� ����� �ͽ��ϴ�.
������ ���� inject and cut ����� EMR �� SM invasion�� �ִ� cancer�̰� resection margin�� ������� �ʴٰ� �Ƿڵ� ȯ���Դϴ�.
Outside slide reading: EMR; ADENOCARCINOMA, MODERATELY DIFFERENTIATED, arising from tubular adenoma
1. Location : body (according to outside report)
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 8 mm (2) vertical diameter, 6 mm (according to outside report)
6. Depth of invasion : invades submucosa, (depth of sm invasion : 300 ��) (pT1b)
7. Resection margin : free from carcinoma(N) safety margin : closest lateral, 0.2 mm (in given specimen), deep, 80-90��
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
���ð� �����˻縦 �Ͽ��� suspected high grade dysplasia�� ���� ESD�� �� �� �ۿ� �������ϴ�. Fibrotic scar ������ �̷� ����� ESD�� ����ġ �ʽ��ϴ�.
�����˻� �����̶� �����̶� �ǽɽ������ ũ��� �����ϰ� ESD�� �� �� �ְ� �Ǿ����� ���ڽ��ϴ� (2020-2-11. ������)
[���� �������� �ǷڵǾ����� �ܺ� �����̵� ���ǵ����� ���������̰� ���ǽɵȴٰ� ���� ESD�� �Ͽ��� ���������� ���� Ȯ�ε� ����]
�ܺ� �����̵� ���ǵ�: Atypical glands, high grade dysplasia versus tubular adenocarcinoma, well differentiated. ESD is recommended.
![]() 9. 2014 Konkuk symposium lecture on adenoma (LJH)
9. 2014 Konkuk symposium lecture on adenoma (LJH)
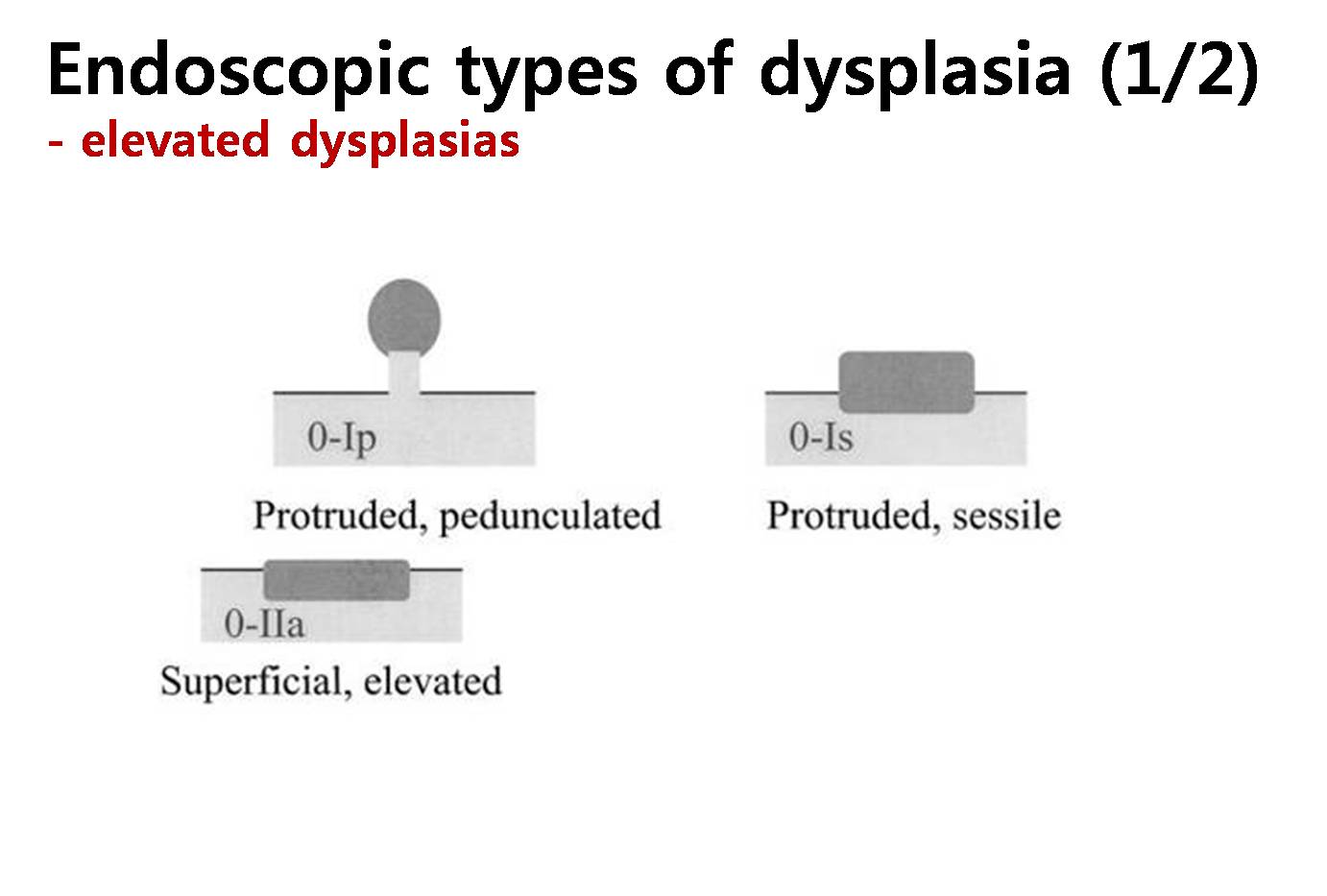
There are no generally accepted definitions of dysplasia and adenoma of the stomach. Dysplasia is best defined as an unequivocal neoplastic epithelial alteration. Detailed histological findings of gastric dysplasias have been described in many literatures. However, endoscopic or gross findings of gastric dysplasia need to be studied in more detail. Macroscopically, two types of dysplasias are recognized: elevated dysplasia and flat/depressed dysplasia.
Definition for adenoma is somewhat confusing. In the western countries, adenomas mean elevated or nodular lesions with dysplasia in histology, so only elevated type of dysplasias are considered as adenomas. In the eastern countries, however, both elevated and flat/depressed types of dysplasia are considered as adenomas. Actually, the terms dysplasia and adenoma are thought to be the same thing in the clinical practice. The difference is who prefers what. Usually, pathologists prefer dysplasia, and endoscopists prefer adenoma.
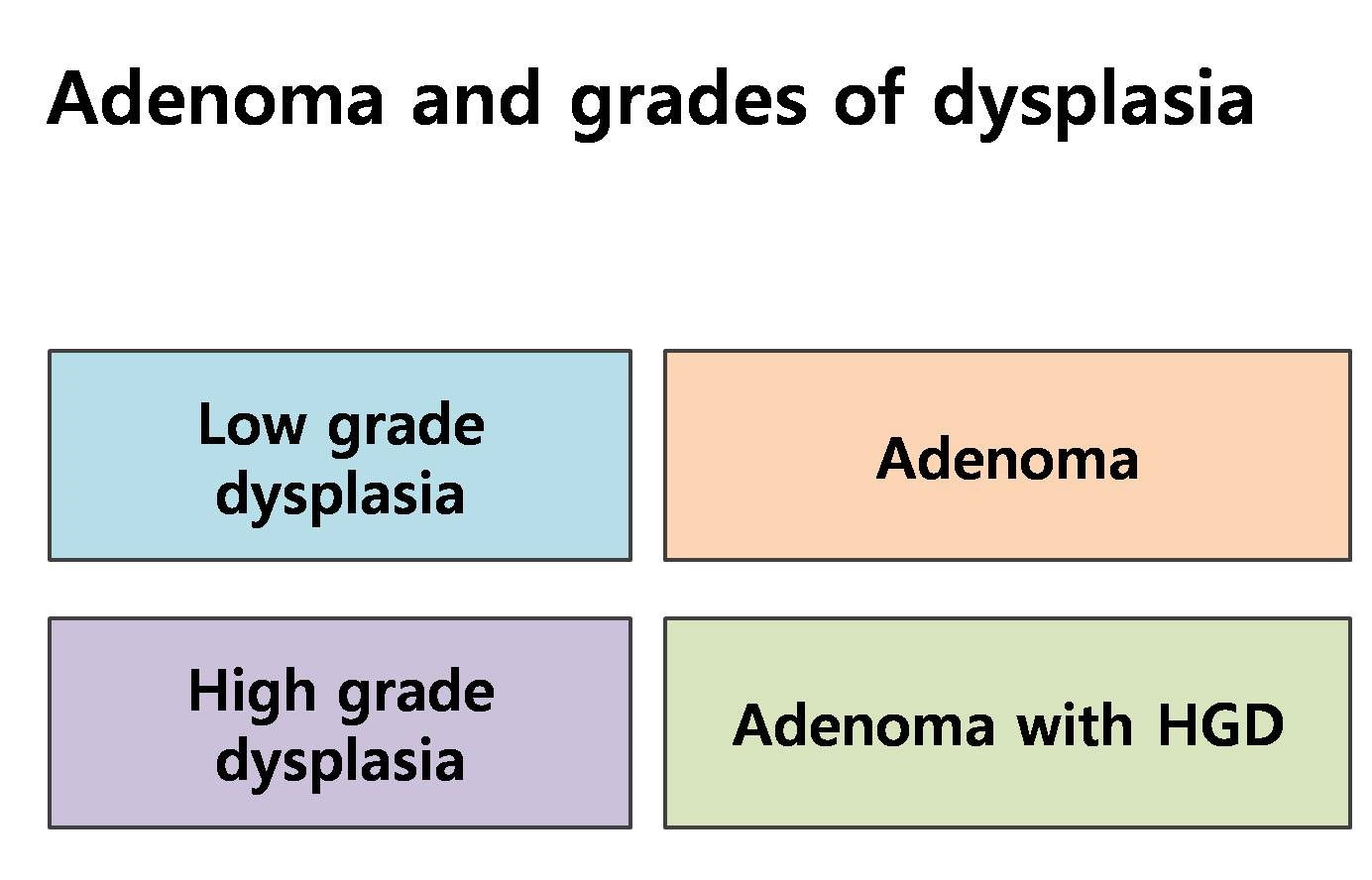
Dysplasias are graded as either high grade or low grade. So, adenomas (= dysplasias) can be divided as adenoma with low grade dysplasia (LGD) and adenoma with high grade dysplasia (HGD). In Korean pathologists' tradition, adenoma usually means adenoma with LGD.
In Korea, gastric adenomas with HGD are usually treated by endoscopic resection. In the final pathology for the resected specimen, 1/3 to 1/2 of adenomas with HGD are upgraded as cancer. Therapeutic approach for adenomas with HGD should be the same for early gastric cancers within absolute indications for endoscopic submucosal dissection (ESD).
Situations for gastric adenomas with LGD are quite different. After endoscopic resection of adenoma with LGD, the risk of histological upgrading is relatively small. About 10-20% of adenomas with LGD are upgraded to adenoma with HGD and 5-10% are upgraded to early gastric cancers. So, the clinical options for adenomas with LGD can be resection (EMR or ESD), ablation, and observation. In the lecture, some data regarding the advantages and disadvantages of each treatment options will be discussed.
We need to start from the definition of dysplasia. What is dysplasia? Most simply, it is an unequivocal neoplastic transformation.
There are three important histological characteristics for gastric dysplasia. They are disorganized mucosal architecture, abnormal differentiation, and cellular atypia.
Based on those three characteristics, a lot of grading schemes have been proposed. Isn��t it confusing?
Recently, dysplasias are histologically divided into two groups, low grade dysplasia and high grade dysplasia.
Endoscopically, dysplasias can be divided into elevated dysplasias and flat/depressed dysplasias.
What is the relationship between dysplasia and adenoma? Definition of adenoma is somewhat confusing. In the western countries, adenomas mean elevated or nodular lesions with dysplasia in histology, so only elevated type dysplasias are considered as adenomas. In the eastern countries, however, both elevated and flat/depressed dysplasias are considered as adenomas. Actually, the two terms dysplasia and adenoma are thought to be the same thing in the clinical practice. The difference is who prefers what. Usually, pathologists prefer dysplasia, and endoscopists prefer adenoma.
Dysplasias are graded as either high grade or low grade. So, adenomas (= dysplasias) can be divided as adenoma with low grade dysplasia (LGD) and adenoma with high grade dysplasia (HGD). In Korean pathologists' tradition, adenoma usually means adenoma with LGD.
Ideally, there should be no difference in the histological diagnosis of adenoma and cancer, because everybody is using the Vienna classification. However, it��s not so simple.
The concept of cancer may be different between countries. In Japan, structural and cytological features are important. In the western countries and in Korea, evidence of invasion is much more important. Actually, we think that most cases of HGD in the western system and Korea, as well as some LGD, become carcinoma in the Japanese system.
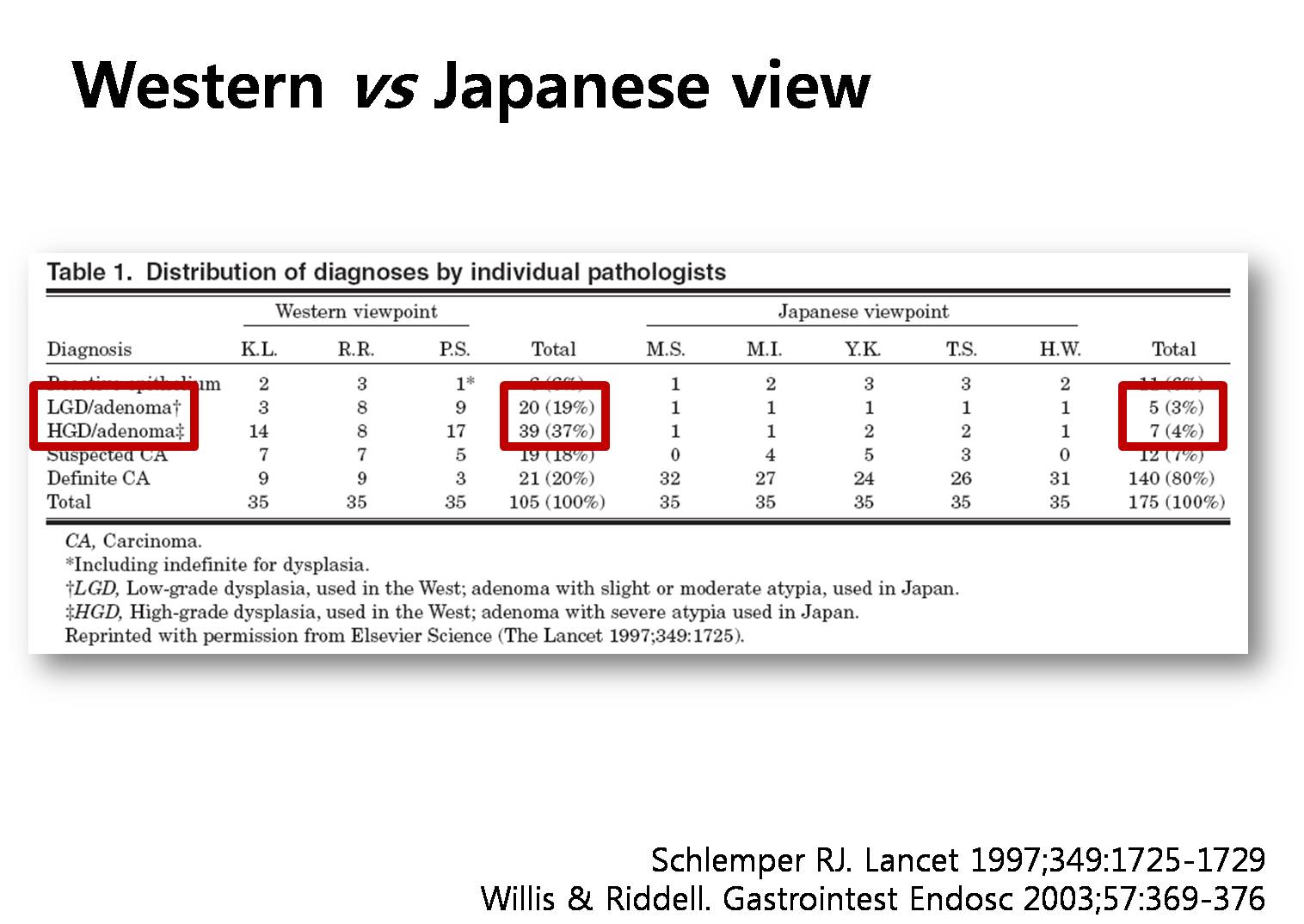
This is a famous study comparing the pathological diagnosis of gastric neoplasm between western countries and Japan. About half of the cases were adenomas by the western point of view. However, only 7 percent were adenomas by Japanese doctors. There is a huge difference. Korean pathologists seem to be close to western doctors in the diagnosis of gastric adenomas.
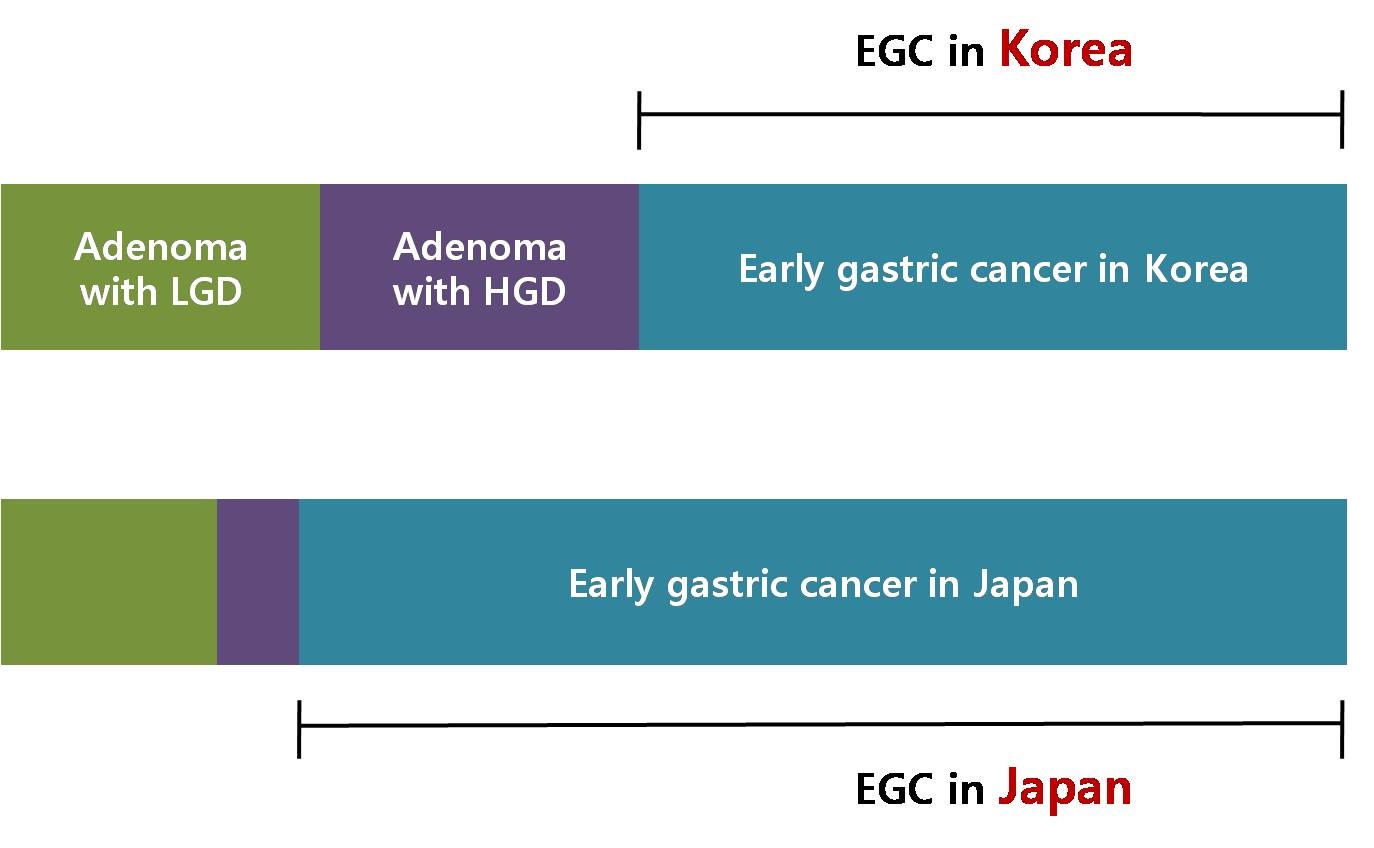
This is my understanding of this confusing situation. Three blocks are adenoma with LGD, adenoma with HGD and EGC in Korea. The next three blocks are diagnoses in Japan. So, most cases of adenoma with HGD in Korea may be EGCs in Japan.
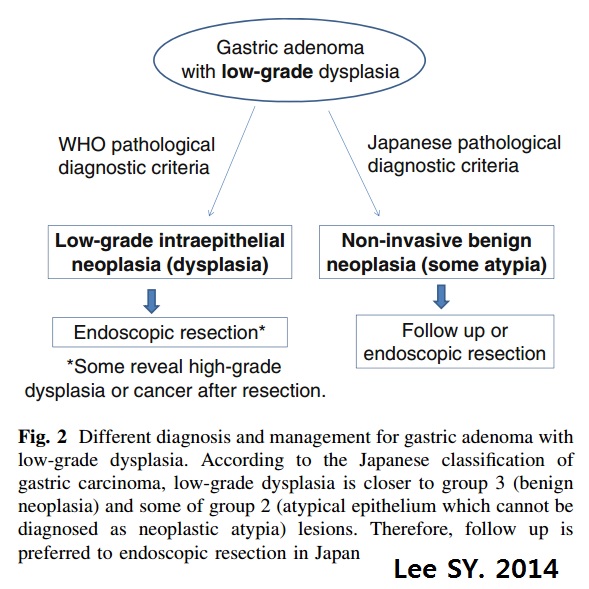
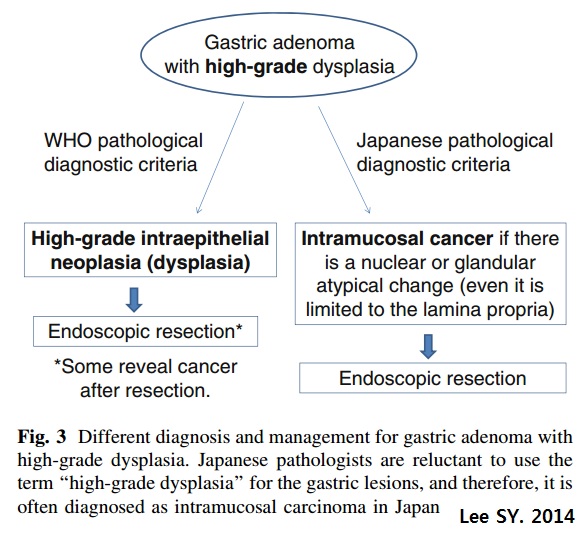
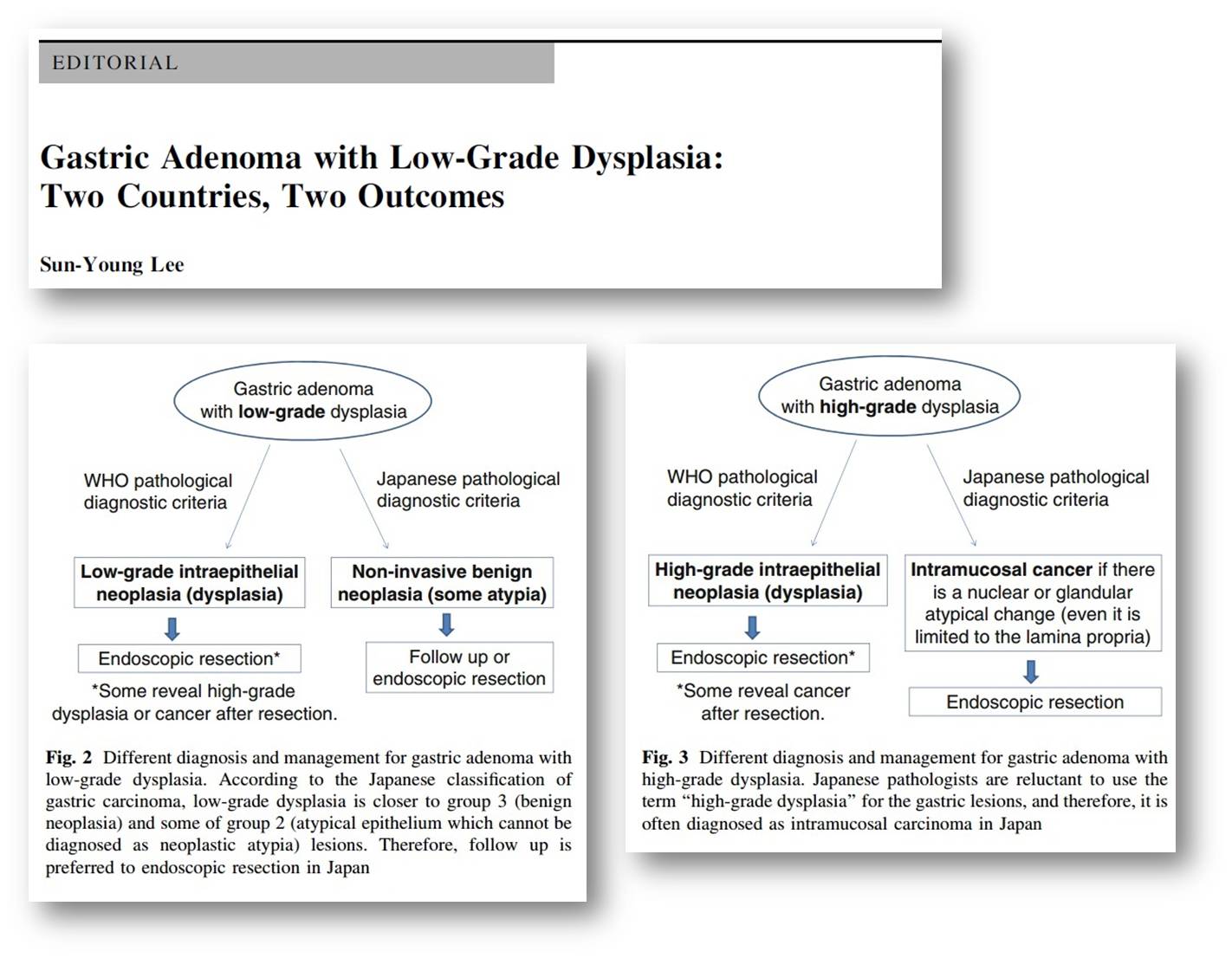
Professor Sun Young Lee at Konkuk University discussed this dilemma in the recent editorial. Most cases of low grade dysplasias are endoscopically resected in Korea, but observation is frequently chosen in Japan. High grade dysplasias are endoscopically resected not only in Korea but also in Japan. But the diagnosis is different.
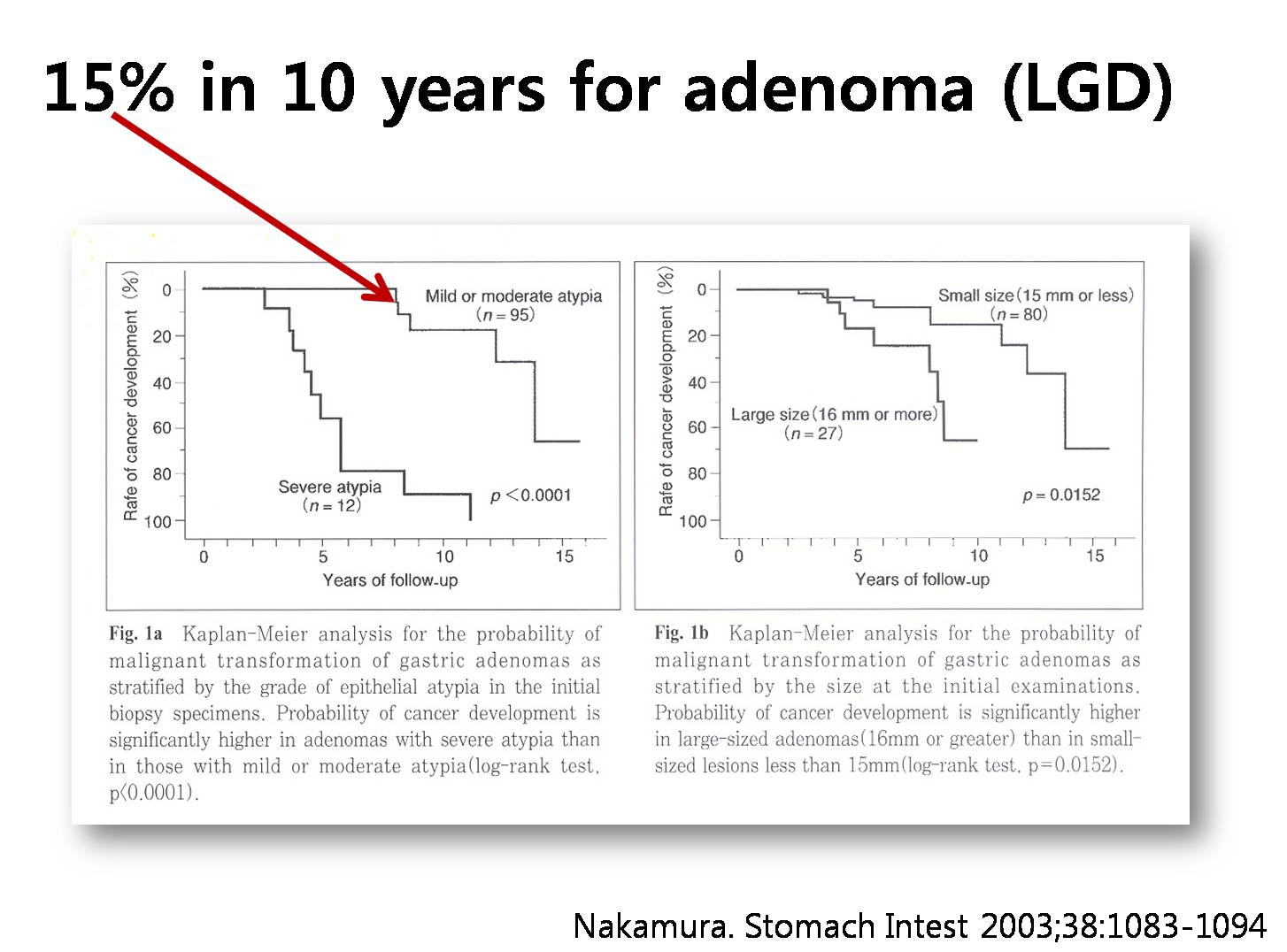
The natural history of adenoma is not clear yet. In this old study, the low grade adenomas progressed to cancer in 15% in 10 years.
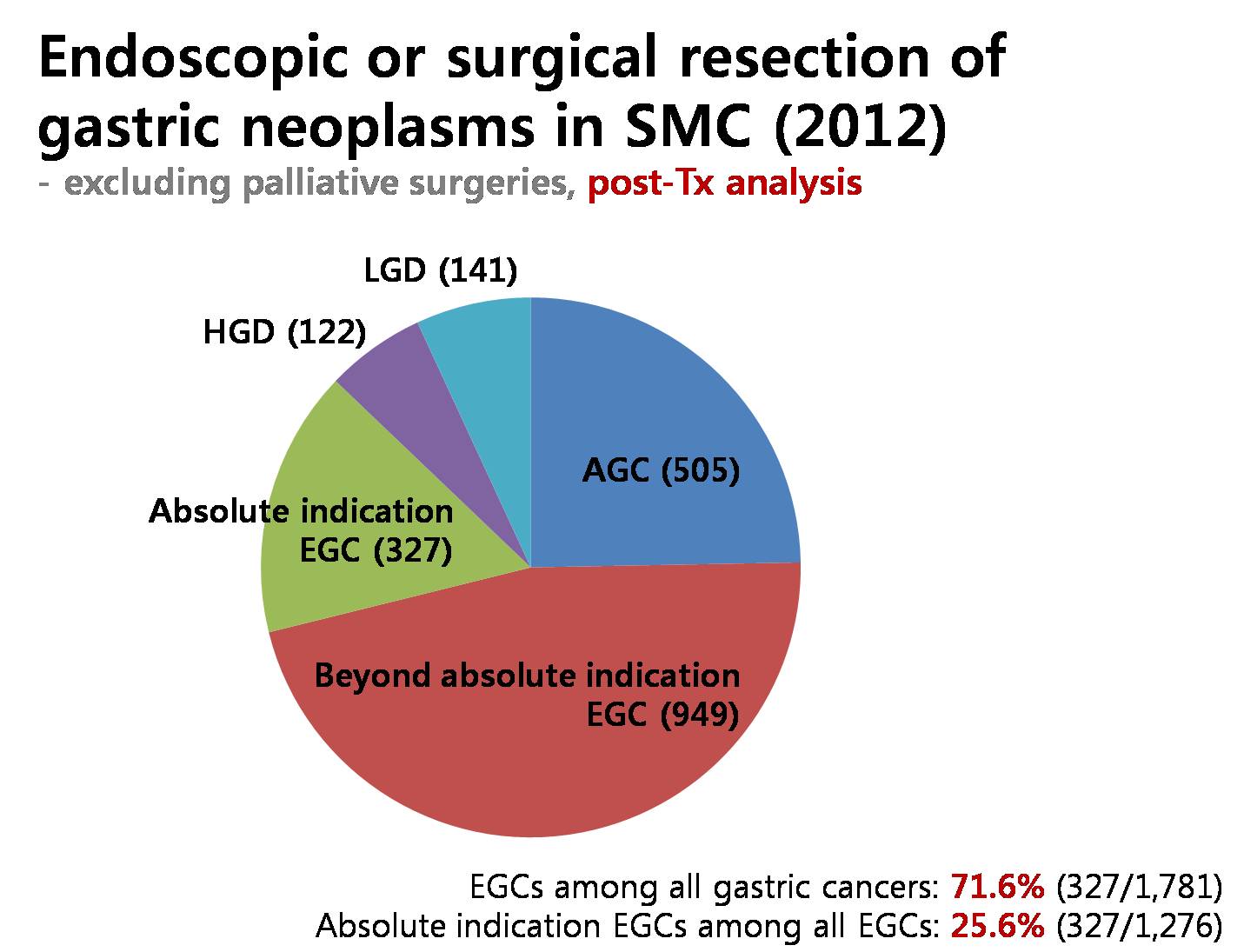
Excluding palliative surgeries, we have endoscopically or surgically treated more than seventeen hundred gastric cancers in 2012 at Samsung Medical Center. Among them, 72% were early gastric cancers. In early gastric cancers, cases within absolute indications were 25%. There were 263 cases of gastric adenomas in a single year.
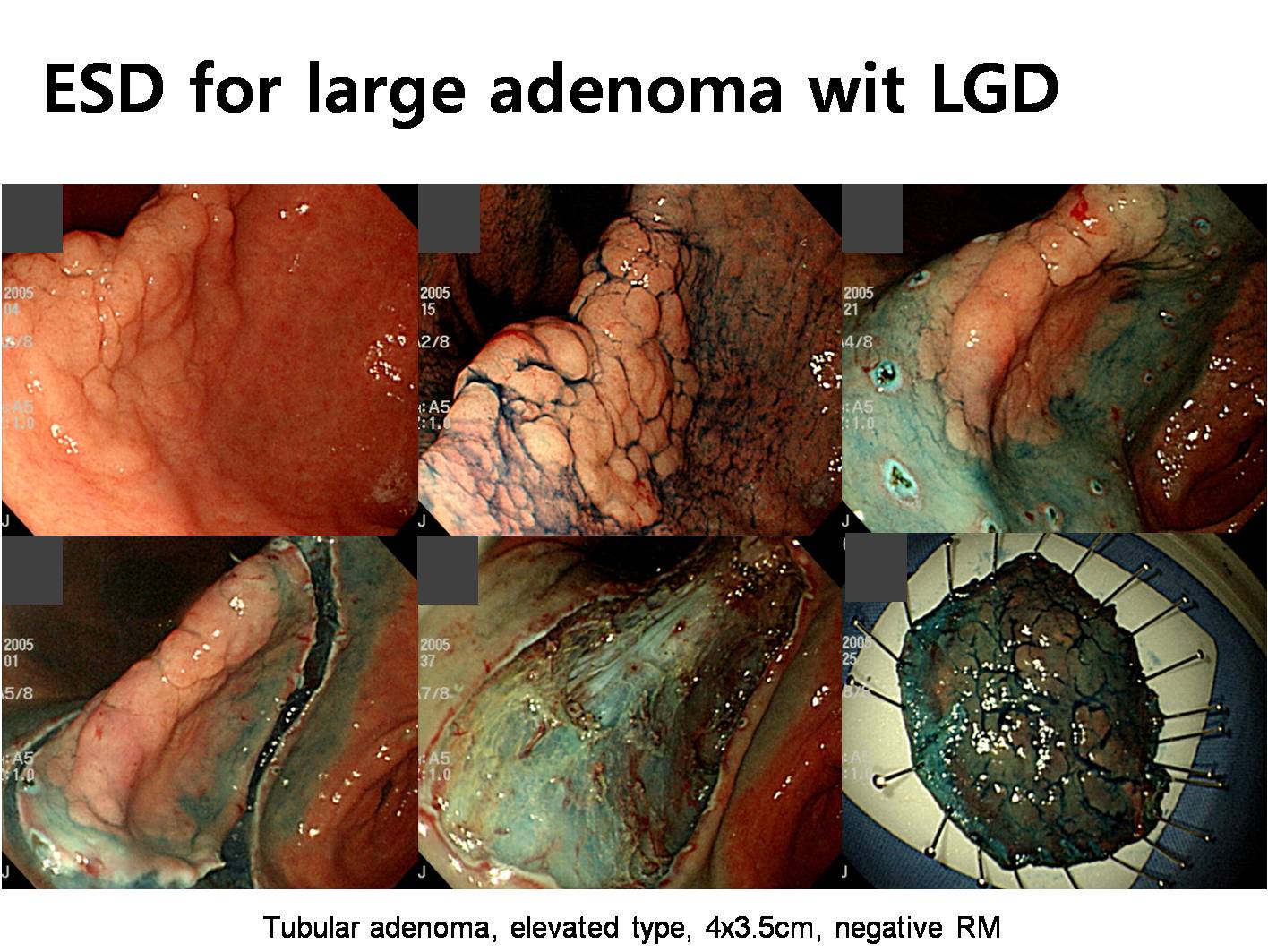
This is an example of endoscopically treated adenoma with low grade dysplasia.
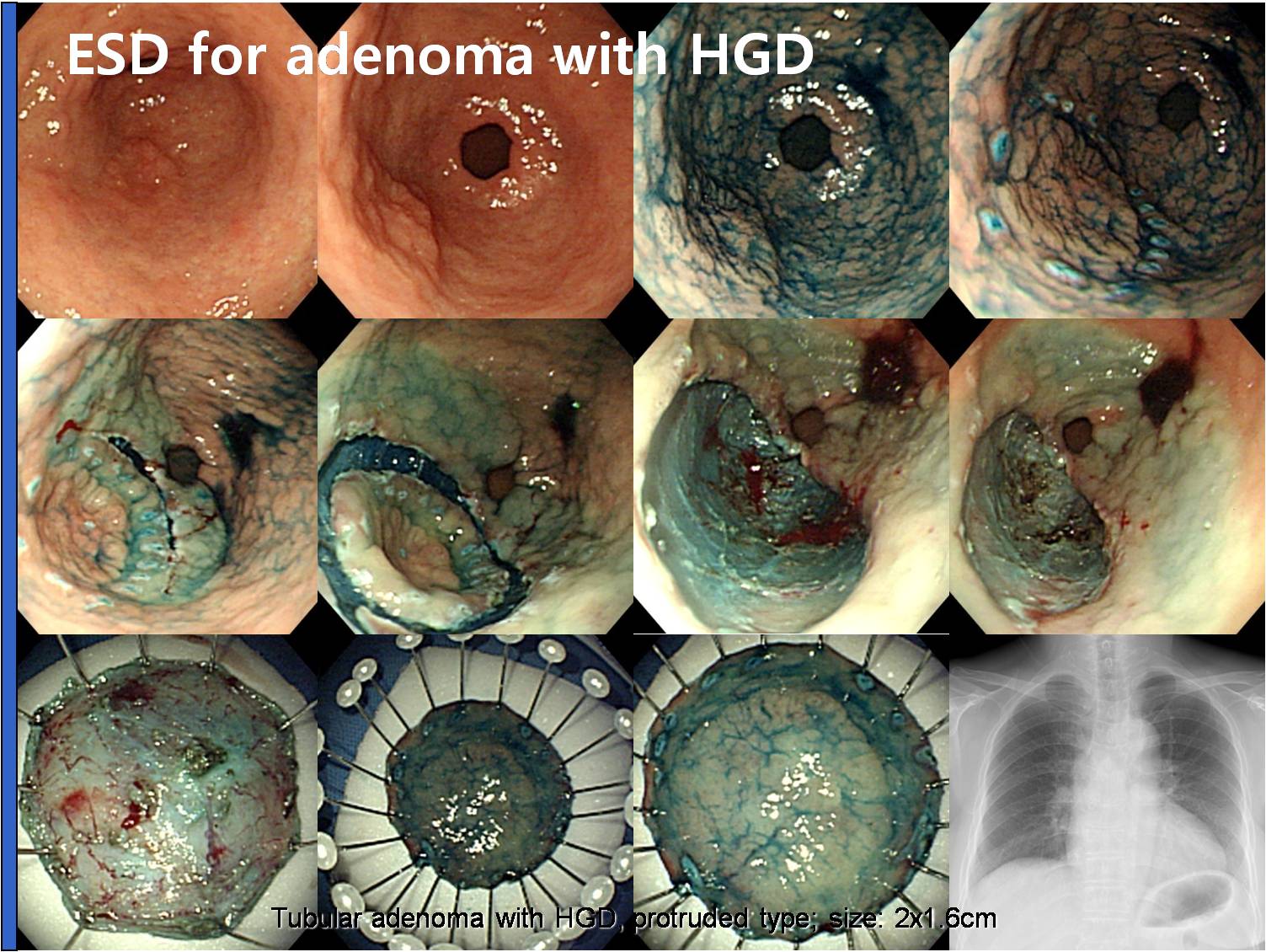
Almost the same thing except that it was an adenoma with high grade dysplasia.
I performed ESD for a small depressed adenoma with LGD.
However, the final ESD pathology was adenocarcinoma.
It��s another example of gastric cancer with initial biopsy of adenoma. In this case, the initial biopsy was adenoma with low grade dysplasia.
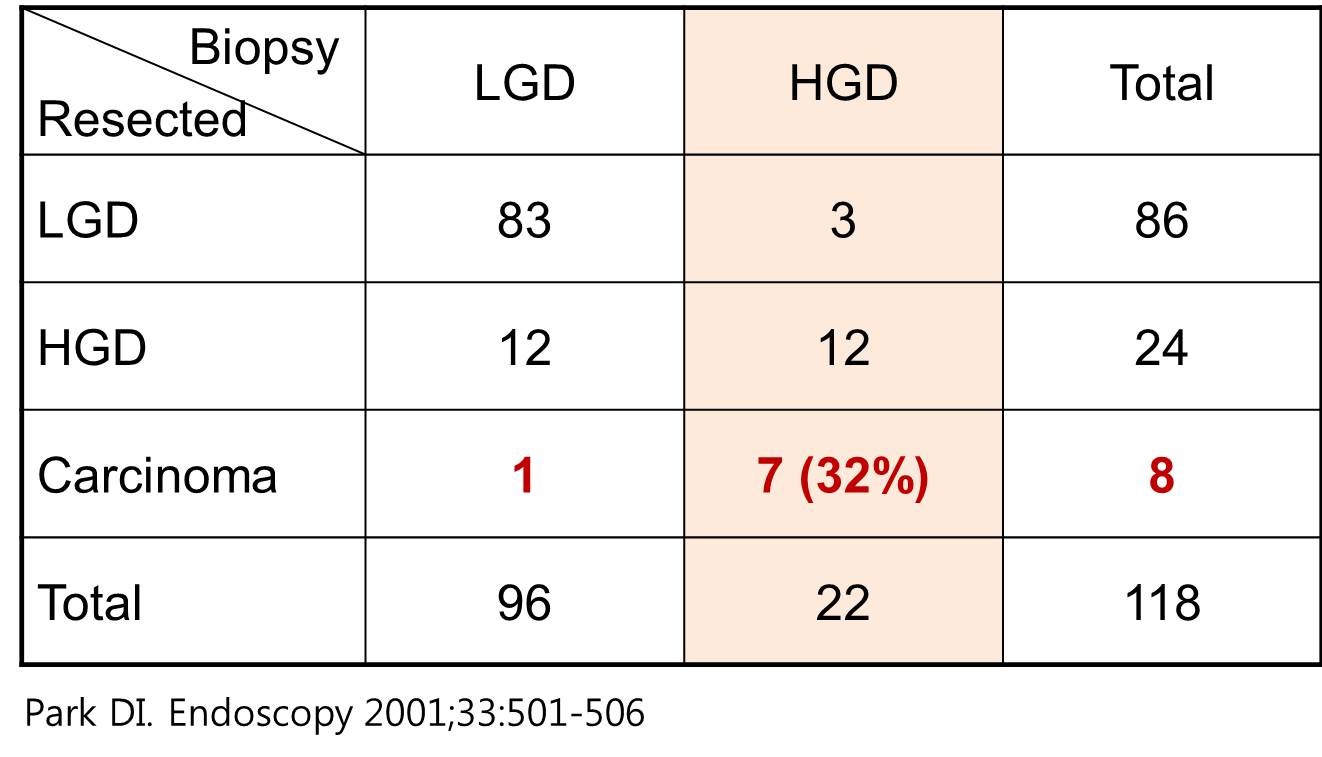
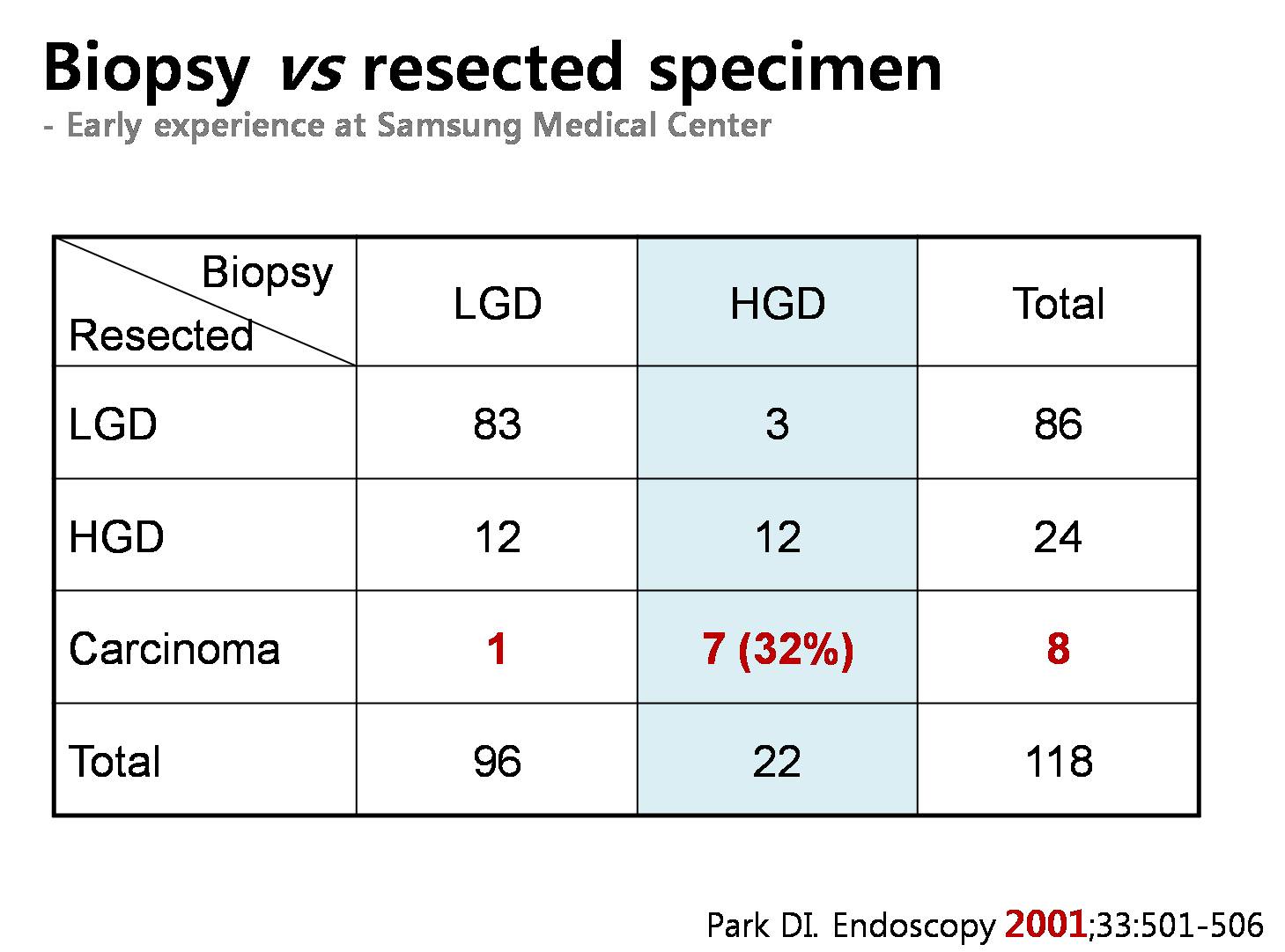
In this old report from my institution, 7 out of 22 adenomas with HGD were actually carcinomas in the endoscopically resected specimen.
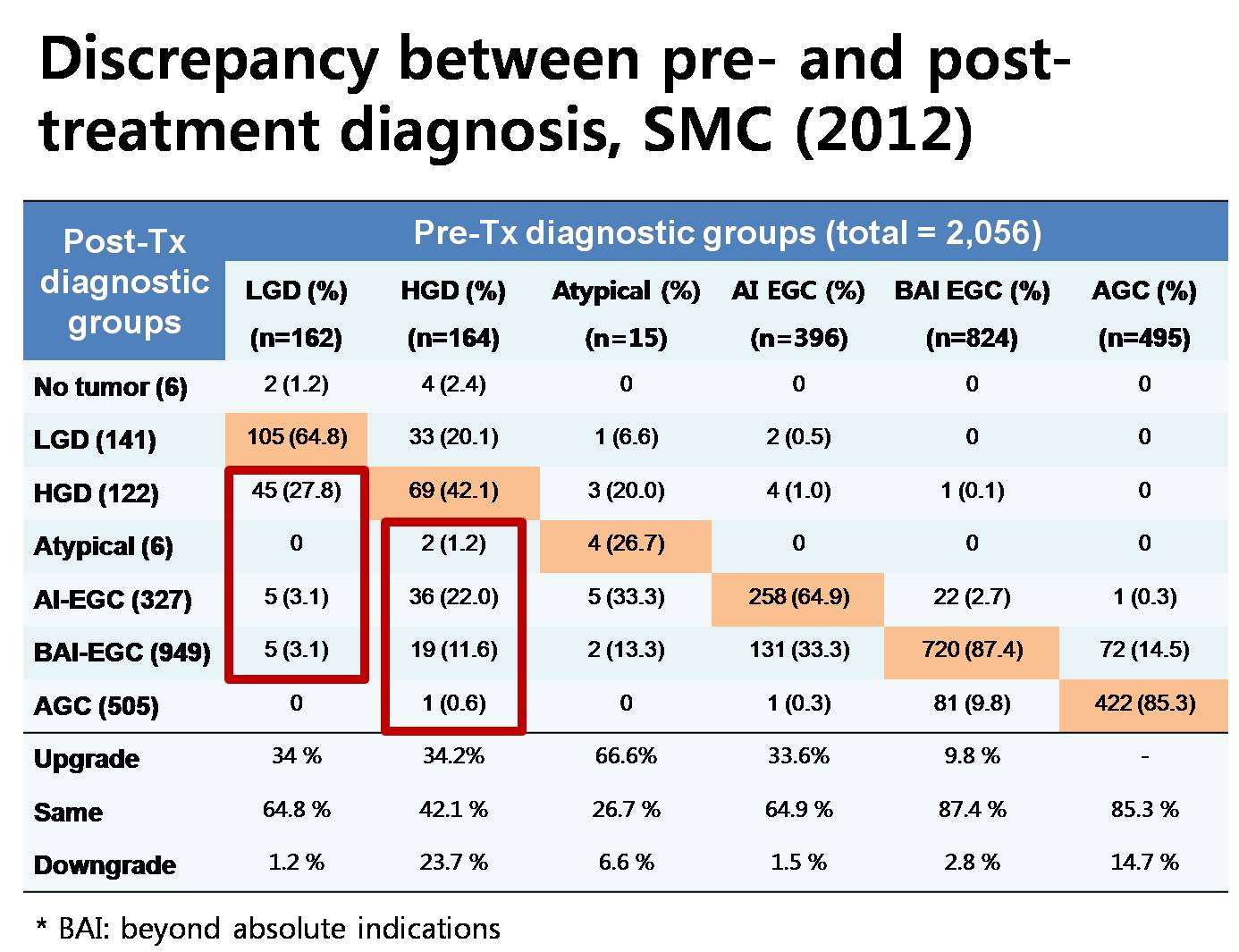
We reviewed the discrepancy between pre-treatment diagnostic groups and post-treatment diagnostic groups. As you can see in this complicated slide, the rate of discrepancy is more than expected. For adenoma with LGD, about 34 percents were upgraded as high grade dysplasias or cancers. For adenomas with HGD, 34 percents were upgraded as cancers.
This is a personal communication. About 1/3 to half of cases with high grade dysplasia are upgraded into cancers at Samsung Medical Center, Gangnam Severance Hospital, and Asan Medical Center.
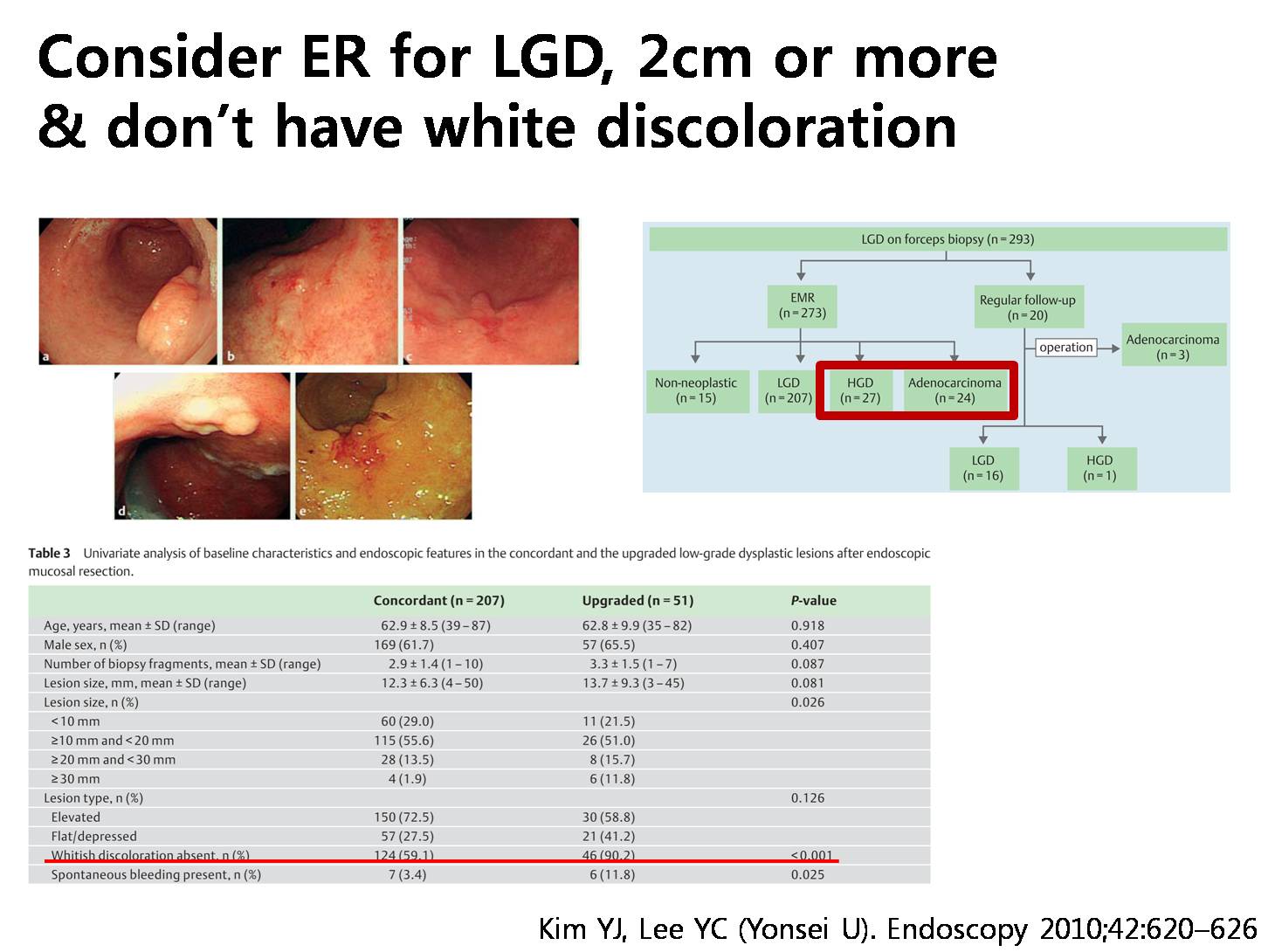
In this report from Yonsei University, 51 out of 273 endoscopically resected low grade adenomas were upgraded into either HGD or adenocarcinoma. They evaluated the risk factors for upgrading, and recommended endoscopic resection for larger lesions and lesions without white discoloration
So, small pale flat elevated low graded adenomas can be easily treated by ablation therapy using argon plasma coagulation.
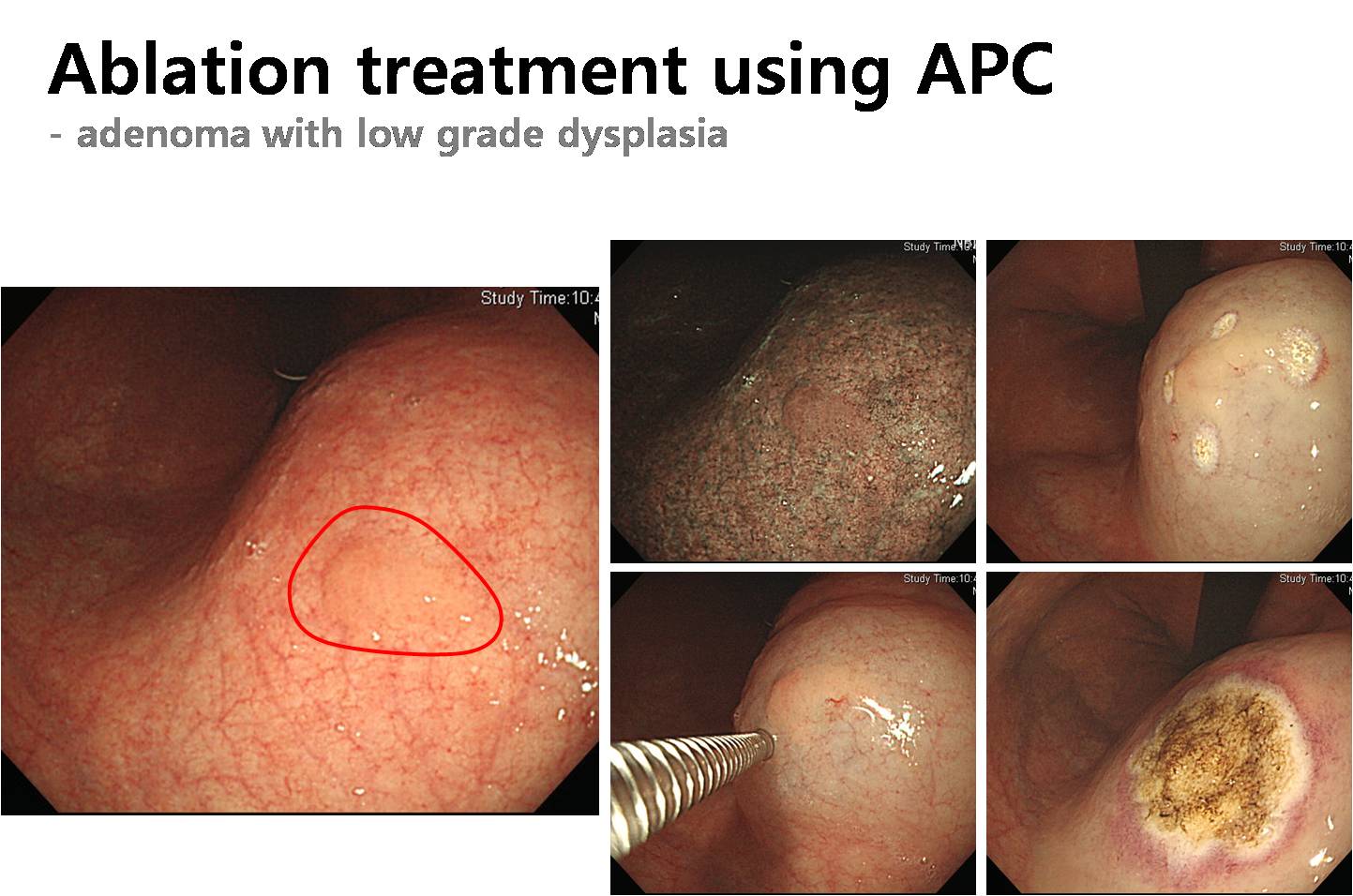
Ladies and gentlemen. I��d like to conclude my short presentation. For adenomas with HGD, endoscopic resection, preferably ESD, is recommended. For adenomas with LGD, endoscopic resection is preferred for larger lesions or lesions with central depression. Ablation is an easy and effective treatment for small pale flat/elevated adenomas with LGD.
![]() 10. ���� ESD �� CT���� �߰ߵ� �����
10. ���� ESD �� CT���� �߰ߵ� �����
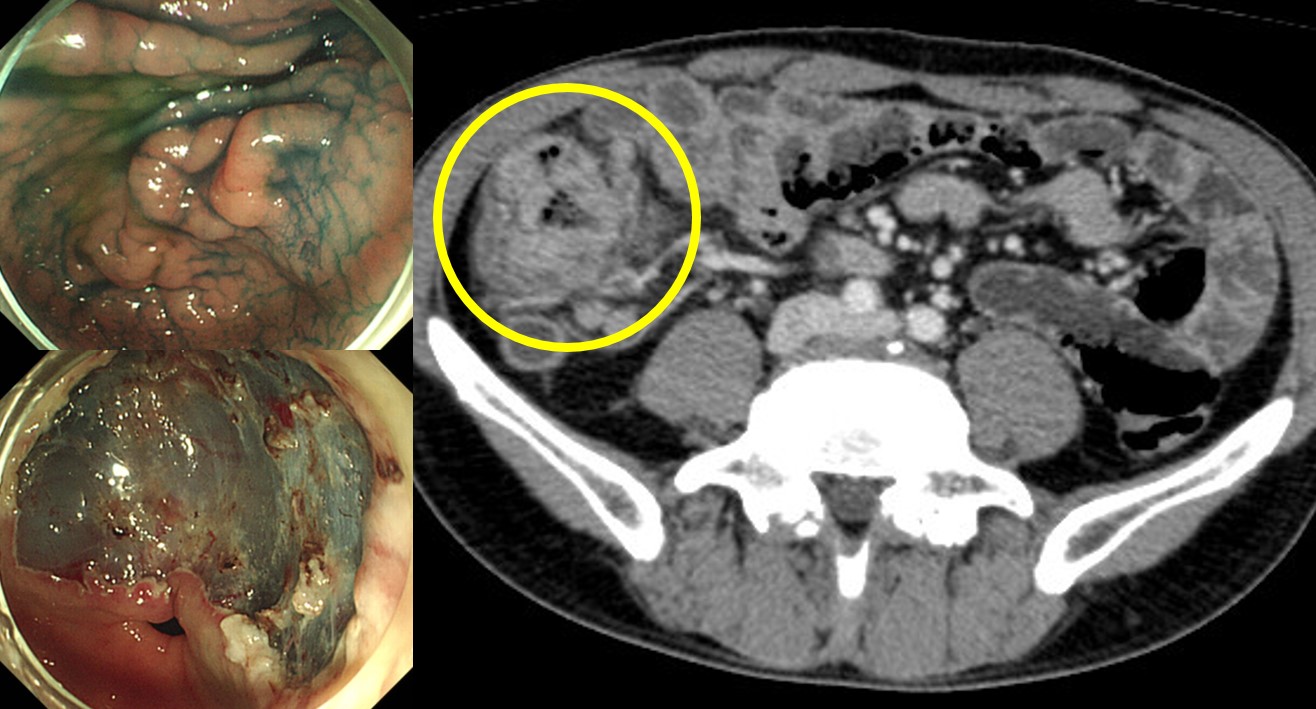
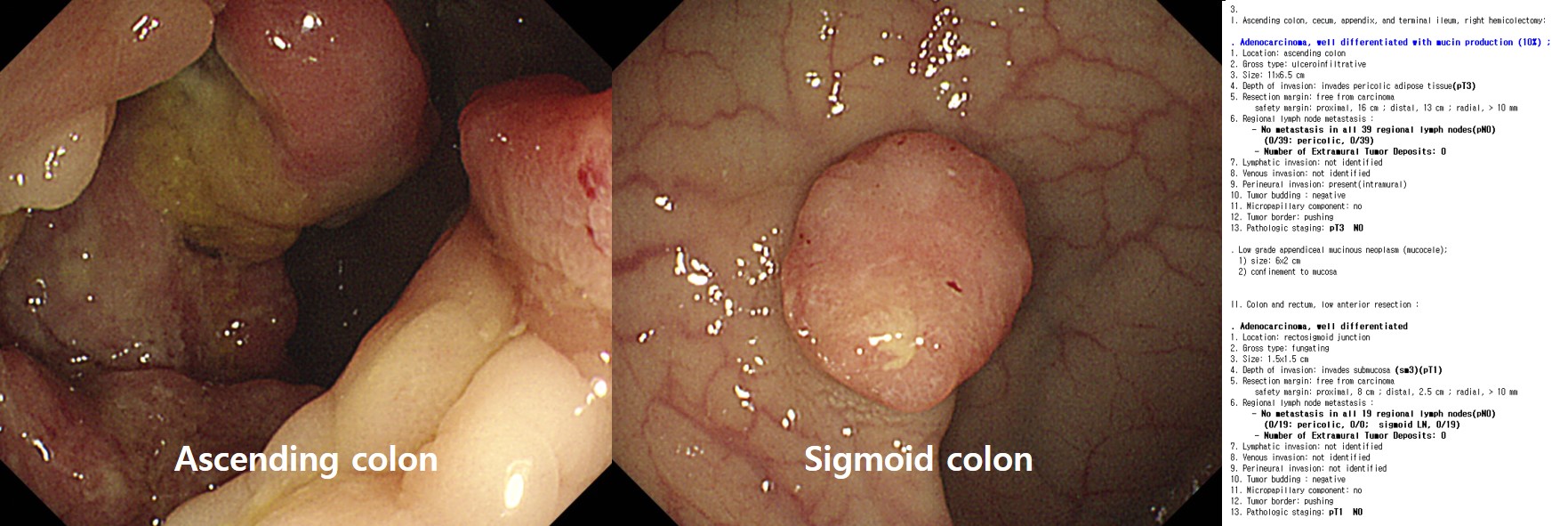
�츮���� �����ð��� �ʹ� ���� ����˴ϴ�. ���� ���� �������� ������ ���ο��� ����Ǵ� ���� �����̰�, ��Ư���� ���� ������ ���� ȯ�ڿ��� ���� �����̳� ���װ˻纸�� ���� �����ð��� ����DZ �մϴ�. �� ��� ���� ���� �� ������� ���� ���¿��� �����̳� ���������� ��������� �ǷڵǴ� ��찡 �ֽ��ϴ�. ���� ������ ESD �� CT�� �����ϴ� ��찡 �����ϴ�. �ֵ� ������ ESD �� �������� ������ �ٲ�� ���� ���� �����Դϴٸ�, ���� ���� �� �����Ͽ��� ���ɼ��� �����ϴ� �͵� �� �ٸ� �����Դϴ�. �� �������� �ſ� ���� incidental finding�� �߰ߵ˴ϴ�.
�Ʒ� ȯ�ڴ� ������ ESD�� ���Ͽ� �ǷڵǾ��� �ü� �� ������������ Ȯ�εǾ����ϴ�. ���� �� ESD �� CT���� ������� �ǽɵǾ���, ���峻�ð濡�� �� ���� ������� �߰ߵǾ� ���嵵 ������ �Ͽ����ϴ�.
![]() [FAQ]
[FAQ]
[2015-5-5. �ֵ��� ����]
[2015-5-5. ������ �亯]
�� ���� ���� ġ��� ���ÿ��� ���� ���� �����ؾ� �մϴ�. ���� �������� ESD����, �߰� ������ ablation, �ټ� �������� careful observation, ���� �������� ���� �� ���� ������ �����մϴ�. 70���̰�, ���� ���� ���� ������ ���̰�, �����ϰ� ����� ���������̹Ƿ� ��� �����Բ��� 1�� �� �������ð��� ���Ͻ� ���� acceptable �� �������� �����մϴ�. ���� �� ȯ�ڶ�� ablation Ȥ�� resection�� ���Ͽ��� �� ����� �մϴ�. ���� ǥ������ ġ����� �������� ���� ������ ��ȯ�̹Ƿ� �ǻ� ������ ġ��� ���ÿ� ���̰� ���� �� �ִٰ� ���� ���� ���ڽ��ϴ�. 70�� ���Ĺ� ȯ���� ������������ 1�� �� �������ð��� �� �߸��� �����̶�� ���ϱ�� ��ƴٰ� �����մϴ�.
[2015-5-5. ȯ�� ��ȣ�� ����]
ū ������������ �Ƿڵ� ȯ���� ��ȣ�ڰ� ����(80�� �߹�)�ε� ���ð� ġ�ᰡ �ʿ��Ѱ� �����Ͽ��� �Ʒ��� ���� ���� ��Ƚ��ϴ�.
[2016-5-31. �ֵ��� ����]
������ �����ֽô� ���������� �����մϴ�. PW/antrum �����̸� EGC�� ���� ������ �����ߴµ� �����˻�� tubular adenoma �����ϴ�.
* Stomach, antrum, posterior wall, endoscopic biopsy ; Suggestive of tubular adenoma, focal high grade dysplasia, (see note) with
1. Erosion.
2. Focally back to back or fused pattern.
3. Combined regenerated atypia.* Microscopic findings by Sydney system ;
1. Neutrophils : absent
2. Mononuclear cells : moderate
3. Atrophy : absent
4. Intestinal metaplasia : mild
5. H.pylori : absent in Giemsa stain* Note : Endoscopic mucosal resection is recommended for excluding higher grade lesion.
�����˻翡�� focal high grade dysplasia�� �־��� �� ���� ���ð� �Ұ��� EGC���� ������ �α� ���к������� �Ƿ��߽��ϴ�. ���ʿ��� ���� ���������̵� review�� �ֽ� ����� ���ð� �����˻� ��� ����� ������ ���ҽ��ϴ�.
���� �����̵� ���ǵ�: Stomach, antrum, posterior wall, endoscopic biopsy: Tubular adenoma with low grade dysplasia.
�α� ���к��� �����˻� ���: Stomach, posterior wall of antrum, endoscopic biopsy: Tubular adenoma with low grade dysplasia (Immunoexpression of tumor: MUC5AC: weakly positive)
�������� �����˻� ����� ���ϰ� ���ͼ� ���� ���� �־��ٰ� �ұ�� ��¦ �Ű��� ���Դϴ�. ���� ���ɼ��� �ּ� 50%��� �߰ŵ��...
��� local���� special stain���� �˻��� �ϵ� �����ϴ�. ���⼭�� H&E stain, Giemsa stain ������ ���ϴ�. �����˻� special stain�� � ���� � ��쿡 �ϴ���, �װ� ��� ������ �Ǵ���, �� �ǹ̰� � ������ �ñ��� ���� �ֽ��ϴ�. Special stain�� ���ؼ� ���ð� ��ȸ�� �������� ���������� ���� �ٷ��� ���� ������ �� �����ϴ�. ���� ������ stain���� ������ �� �ǹ̸� �ٺ��� ����� ���� �ֽ��ϴ�.
[2016-6-6. ������ �亯]
�ϰ� �������� ������ �������� ���� ����Դϴ�. ���� ���Դϴ�. �� �ݴ뵵 �����ϴ�.
���� ���� ������ 5%, ���� ������ 33%�� ���ð� ������ �� ���� ������ ������ �ٲ�ٰ� �����ϰ� �ֽ��ϴ�. ���� �ٰŴ� �Ҽ� ������ �ڷ��Դϴ�. 10�� �̻� ������ �ΰ� ���� ���Ҵµ� ����� ����߽��ϴ�. ���ð� �� ���� �˻��� ����� �������̶�� ���Դϴ�.
ġ�� ���� �������� discrepancy�� �ִ� ��� ȯ�ڿ��� ��� �����ؾ� �ұ��? �� ������ �ֽ��ϴ�. ù��° ����� �ְ����� �Ǵ��̳� ������ ���Ͽ� ����Ÿ�� �ٰ��Ͽ� �����ϴ� ���Դϴ�. �� "����� ���� Ȯ���� ���Դ� 5% ���Դ� 33%�Դϴ�"�� ���� �����ϴ� ��������. �ι�° ����� �ְ����� �Ǵ��� �״�� �����ϴ� ���Դϴ�. �� "���ð����� ���� ��ü�� ������ �� ������ ������ ���� 5-33%�Դϴٸ�, �ƹ����� ȯ�ں��� ���� ���ɼ��� �����ϴ�. ��� ���� ������ ���� �� �����ϴ�"��� �����ϴ� ����Դϴ�. �������� � ����� �����ϰڽ��ϱ�?
���� ù��° ����� �ַ� �̿��մϴ�. �ǻ� ���忡���� 5%, 33%�� �ǹ��ִ� ����������, ȯ�ڿ��Դ� ��¥�� �� �� �ϳ��̱� �����Դϴ�. ���̰ų� ���� �ƴϰų�... ���� ���� �ϴ� �ִ��� ���������� �����ϸ鼭 ���� ��������� ���� �߰� ġ�� �ʿ� ���θ� ��Ȯ�� �������� �����ϰ� �ֽ��ϴ�.
���� ���ɼ��� ���ٰ� ���ߴٰ� ���� �ƴ� ������ ������ "���� ���̳� �ִ� �ǻ�"��, ���� ���ɼ��� ���� ���ٰ� ���ߴٰ� ������ ������ "������ �ƴ����� �� ������"�� ��� �� �ֽ��ϴ�. ���� '���� ������ ������'���� ���� ����� ���Դ� ���մϴ�.
���� ���� �ʽ��ϴ�. 1-2�� �Ƿ��������� ù��° ����� ����ϴٴ� ���� �� �˰� �ֽ��ϴ�. ȯ�ڰ� � ������ ������ �� �� ���� �����̰�����. �ʹ� ���� ���ڸ� ���ϸ� ����ϰ� �߰� �˻�� ġ�Ḧ ���� �ʴ� ȯ�ڵ� ���� ���Դϴ�. ���ٰ� �� �ʹ� ���ִ� ����� ���� ���� �� �����ϴ�. ��Ȳ�� ���� ������ �����ϴ� �� �ۿ� ���ڽ��ϴ�.
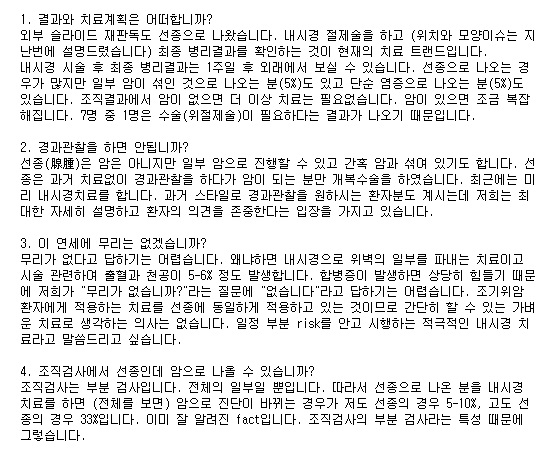
�̷��� �����Ѵٸ� ��ڽ��ϱ�? "���� �ǽɺ��Ұ� �־����ϴ�. ���� �����˻� ����� �� ���ܰ��� �������� ���Խ��ϴ�. �����˻�� �κ� �˻��Դϴ�. ��ü�� ���캸�� ���� �� �ֽ��ϴ�. ���� ���ð� �������� �ʿ��� �� �����ϴ�. ������ ���ð����� �����ϸ� 5-33%���� ������ ���ɴϴ�. ��� �Ƿ����� ��õ�ϰڽ��ϴ�. ���ð� �����, ���ð� ����, �����˻� �����, �����˻� ���� �����̵�, ���� �Ұ��� ì�ܵ帳�ϴ�. ���� ��� �ٶ�ڽ��ϴ�."
P.S. �鿪���������˻�� ������ �ǻ簡 �ʿ信 ���� �߰��ϰ� �� ����� �����Ͽ� ���� ���� ������ ���ϴ�. ��κ��� ��� �ӻ��ǻ簡 �鿪���������˻� ����� ���� Ȯ���� �ʿ�� �����ϴ�.
[2017-4-15 ��õ�����ð漼�̳�. ����]
�ܺν����̵� ���ǵ��� �߿伺�� �����ϼ̴µ���... ���� �����̵尡 �ƴ� paraffin block�� ��û�ϴ� ��찡 ���� �ִ�����.
[������ �亯]
��κ� �ܺ� ���� �����̵�� ������ �ֽ��ϴ�. Paraffin block�� �������� ���� Ư���� ��쿡 ��û�ϱ �մϴٸ� �ſ� �幮 ���Դϴ�. Paraffin block�� �̿��� �߰� �˻簡 �ʿ��� ���� ��κ� �� ���� ���ð� ��˿��� ���� ������ �̿��ϰ� �ֽ��ϴ�.
[2017-4-15 ��õ�����ð漼�̳�. ����]
ġ�� ���� ġ�� �� ���������� ���̿� ���Ͽ� �� ������ �̴ּµ���.... �������� ��� ������ ESD�� ġ���ϰ� ��ô�����? Ȥ�� EMR-C�� ���� �������� ������� ġ���ϴ� ���� ������ �ñ��մϴ�.
[������ �亯]
�ü� �� �����˻翡�� ���� �����̾��� ���� ��� 1/3���� �ü� �� ������ ������ �ٲ�ϴ�. ���� ��Ģ������ ���� ������ ��� ESD�� ġ���ϰ� �ֽ��ϴ�. ���� ������ less invasive�� ������ �����ϴٰ� �����մϴ�. �۰�, flat�ϰ� pale�� ���� ������ ablation���� ġ���� �� �ֽ��ϴ�. �� �ܴ̿� ��κ� �������� �����ϰ� �ֽ��ϴ�. ���� ESD�� ġ���ϴ� ��찡 ������ ��쿡 ���� EMR-P, inject and cut�� ���� ���� �������� �������� ����ϱ �մϴ�.
[2017-4-15 ��õ�����ð漼�̳�. ����]
������ ������ ������ �����ϴ�. ���� ��Ȥ ����, �ߵ (intermediate grade), ������ ���� ���� ������� �����ϴ�. �ߵ (intermediate grade) ������ ��� �����ϴ� ���� ���ڽ��ϱ�?
[������ �亯]
���� �ǻ���� ǥ��ȭ ����� ������ ���� ���� �ɰ��� �����Դϴ�. �ߵ (intermediate grade) �������� �Ƿڵ� ��� �ܺ� �����̵� ���ǵ��� �ϸ� ��κ� ���� �������� ���ɴϴ�. ���� ���� �ߵ ������ �ϴ� ���� ������ ���Ͽ� �����ϰ� �ֽ��ϴ�.
[2017-4-15 ��õ�����ð漼�̳�. ����]
ġ�� ���� ġ�� �� �������� ������ ���ο� ���Ͽ� ��� �����Ͻô�����.
[������ �亯]
�����̳� ������ ESD�� ������ �� non-neoplastic pathology�� ������ �ణ �����մϴ�. ���� �幮 ���� �ƴմϴ�. 2015�� ���ִ� ������ ���� (Yang MJ. Endoscopy. 2015) ���� ������ ��� 6%, ���� �����̳� ������ ��� 3%���� ESD �� non-neoplastic pathology�� ������ �ֽ��ϴ�.
Biopsy LGD HGD or cancer No neoplasia at ESD 39 (5.5%) 13 (2.7%) Neoplasia at ESD 664 470 �̷��� ������ ũ�� �� ������ �����ϰ� �ֽ��ϴ�. (1) ���� ������ �����˻�� ���ŵǴ� ��찡 �ֽ��ϴ�. (2) ������ �� ǥ���� 2 mm �������� �߶� ���� specimen�� ����� ������ 2 mm ������ ������ ������������ �߰����� ���� �� �ֽ��ϴ�. (3) ���ð� ���� ��� mislocalization�� �����մϴ�.
Forcep���� ���� ������ ���� ��ĥ �� ���ð��� �� ���� �ǿܷ� ū �˾��� ������� ��찡 �ֽ��ϴ�. �����˻�� ����� ū ���Ұ� ���ŵǴ� �� �ְڴٴ� �����Դϴ�. Mislocalization (���� ���� '�����'�̶�� �մϴ�^^)�� �ſ� �幮 �� �����ϴ�.
* ����: EndoTODAY Nonneoplastic pathology after ESD
[2019-8-7. ������ ȥ�㸻] ���� ���� �����մϴ�. �ʹ� ����.
70 years old lady visited my clinic due to an adenoma of the cardia involving at least 3/4 of the circumference, which was detected during the screening endoscopy. In the local hospital, endoscopic resction was tried but failed. Actually the procedure stopped in the middle of the marking step. Surgical treatment was recommended in that hospital. What's your option for this woman?

I decided to try endoscopic resection again, although the procedure would be very difficult. I gave full information about the advantages and disadvantages of the endoscopic treatment in this challenging situation.
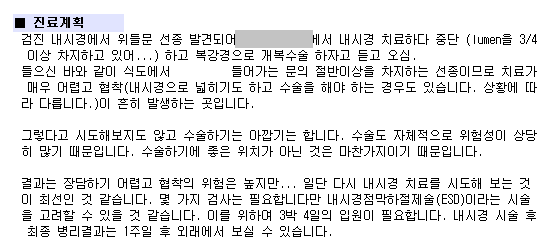
Endoscopic resection (multiple piecemeal) followed by APC ablation was done. The procedure time was 42 minutes. PPI with oral steroid (4 weeks course) was given for the prevention of the stricture.
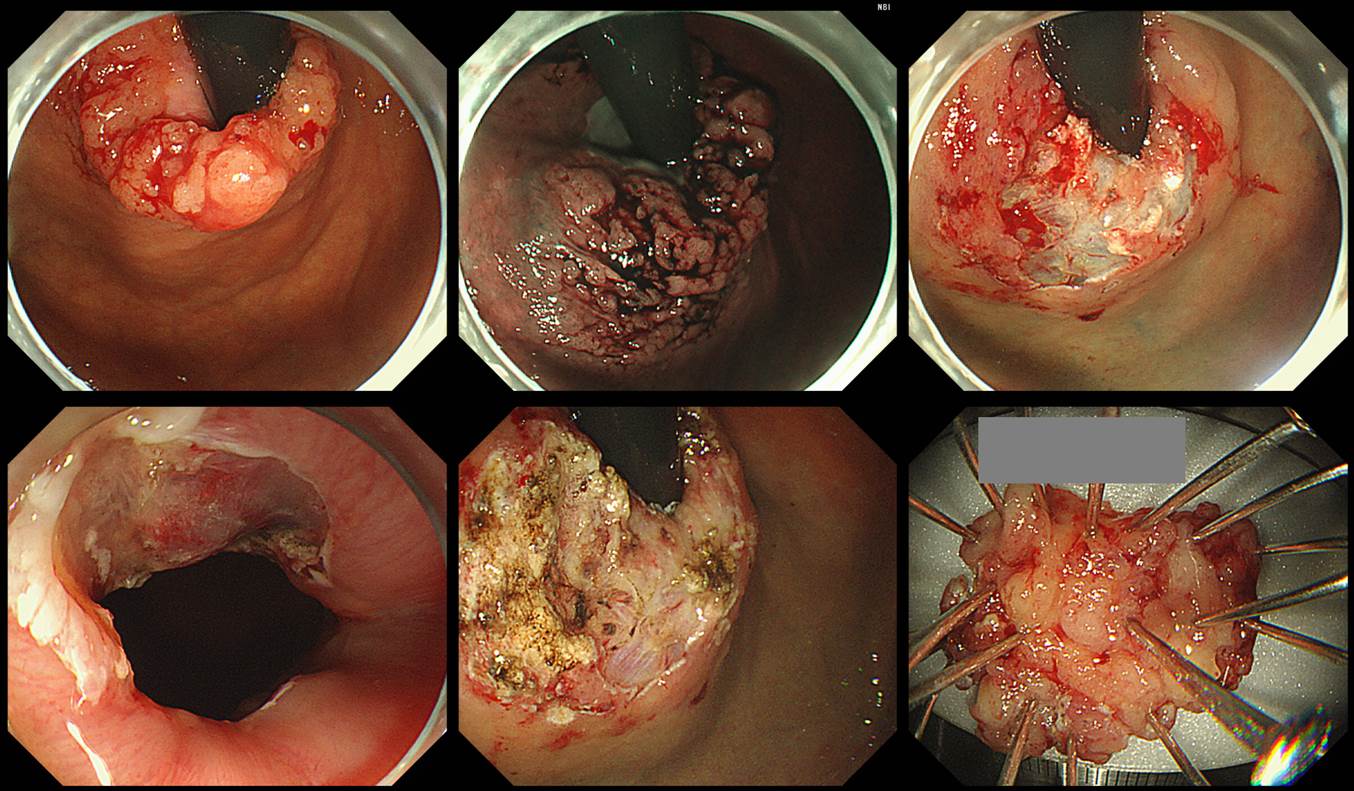
The final pathology was acceptable.
Tubulovillous adenoma with high grade dysplasia ;
1. Location : cardia
2. Gross type : elevated
3. Size of adenoma : (1) longest diameter, 24 mm (2) vertical diameter, 15 mm
4. Resection margin : involved distal resection margin by adenoma negative other resection marginsEndoscopic resection of the gastric neoplasms is getting more and more difficult for me, because easy cases are treated in the local clinic. Challenging cases are referred so often. It is time to think about early retirement.
[2019-9-3. ������ ȥ�㸻]
Tubular adenoma�� ��ջ����̶�� �θ�������.
[2020-5-30. �ֵ��� ����] ����������high grade dysplasia�� ���� ���ɼ��� �����ϱ�?
������. High grade dysplasia �� �������� �� ������ �� ������ �����̶� ���� �ִٰ� �˰� �ֽ��ϴٸ� �ӻ��� ���̰��ɼ��� ���ٰ� ����. �̰� �´� �ǰ���?
[2020-5-31. ������ �亯]
��. ��Ģ�� �½��ϴ�. High grade dysplasia�� ���� intraepithelial lesion�̰� epithelial cell�� basement membrane�� ħ������ ���� ���� �ǹ��� non-invasive pathology�Դϴ�. ���� ���ɼ��� ���ٰ� ���� ���� �½��ϴ�. ���� �� ���� tricky�� ���� �ֽ��ϴ�.
1) �����ǻ��� inter-observer variation�Դϴ�. � �����ǻ�� ���ݸ� �̻��ϸ� ������ �����ϰ�, �� �ٸ� �����ǻ�� �����ؼ��� ������ �θ��� �ʽ��ϴ�. Inter-continental difference�� �� �˷��� �ְ�, inter-national difference�� �� ����������, �� ���� �ȿ����� Ȥ�� �� ���� �ȿ����� inter-oberserver variation�� ��� ���� ������ ������ �Ҹ�Ȯ�մϴ�. �ᱹ ���� �����˻� sample�� ���� �ǵ��ϰ� �ִ���, ���� ������ ��� �ľ��ϰ� �־�� �մϴ�. �ñ��ϸ� ��ȭ�� ������ �� ���� ������ communication�� �����ؾ� �մϴ�. ���� �������� �ٹ��ϰ� �ִ� ���忡�� �����帮��, ���� ������ �����˻縦 ���� �����ǻ簡 �ǵ��ϰ� �ֽ��ϴ�. ���ð� �Ұ߰� ���� �Ұ��� ��ġ���� ���� ������ �켱 ���� �ǵ��ϼ̴����� Ȯ���ϰ� �ֽ��ϴ�.
2) �����˻� ����� ESD ����� ����� �ٸ��ϴ�. �����˻�� �κ� �˻��̰� ���� �����̹Ƿ� �����ǻ� ���忡���� '��'���� �θ��� ����� ��Ȳ�� �����ϴ�. �� ����� �ѵ� ���̶�� �ܾ��ϱ� ����� ��Ȳ ���Դϴ�. �� ��� ���� ���������� �����DZ �մϴ�. ESD ��ü������ �� ������ �����ϴ�. ��ü �˻��̰� ���� ġ�Ḧ ��ģ �����̹Ƿ� �����ǻ� ���忡���� '��'�̶�� ������ ���̴µ� �ɸ��� ������� ���� ���Դϴ�.
���� �� �̽�(ESD ���� ���� ����� ����)�� Diagnostic Group Classification�̶�� �������� �����ϰ� �ֽ��ϴ� (Lee JH. Surg Endosc 2016).
Results: The study patients belonged to the following pretreatment diagnostic groups; LGDs in 162, HGDs in 164, AI-EGCs in 396, BAI-EGCs in 824, and AGCs in 495 cases. Posttreatment diagnostic groups were LGDs in 140, HGDs in 121, AI-EGCs in 322, BAI-EGCs in 947, AGCs in 505, and no residual tumor in 6 cases. In general, 6.9% (141/2,041) of cases were down-graded, and 15.9% (324/2,041) were up-graded. Thirty-four percent of pretreatment HGDs (56/164) were changed to cancers after endoscopic resection. Thirty-three percent of pretreatment AI-EGCs (131/396) were re-grouped as posttreatment BAI-EGCs.The additional surgery rate in each pretreatment group was 0.6% in LGD, 4.3% in HGD, 15.7% in AI-EGC, 23.6% in BAI-EGC among the patients with initial endoscopic resection (p < 0.01).
�ᱹ ���ð� �����˻翡�� �������������� ���Դٴ� �����δ� ���� �Ƚ��� �� �����ϴ�. �ּ��� ESD �������� ���� �ƴ� ���� Ȯ���� �� ���� ���ɼ��� ���ٰ� ���ؾ� �� �� �����ϴ�.
3) ������ ������ ũ�� ���ΰ� ���̵� ������ �� ���� �����Դϴ�. 2014�� �DZ����б� �������� ���� ���Ǹ� �غ��ϸ鼭 ���� ������ �ֺ� ������ �ü� ���� ���� upgrade(ESD �� ��������, ESD �� ��)�� ������ ������ �˾ƺ� �� �ֽ��ϴ�. �� �Ҽ� ������ 1/3 �����̾��� 1/2�� ���� �Ѵ� ����� �־����ϴ�. ���������δ� �� 60% ������ ������ �˰� �ֽ��ϴ�. �� ���� �ڱ� ���� �ǻ��� ������ �� �˾ƾ� �Ѵٴ� ���� �����ִ� �ڷ��Դϴ�.
4) ���������� �ſ� �������ʹ� ���ʸ� �Ұ��մϴ�. ESD �� extragastric recurrence�� ������ �ſ� �����ϴ�. ���� 0%�� �ƴմϴ�. �ſ� ���� ȯ�ڸ� ġ���ϴٺ��� �Ҽ��� ��Ÿ��� ���ʵ��� ������ �˴ϴ�. �Ʒ� ȯ�ڰ� �� ����Դϴ�.
�����˻翡�� �������������� �ǷڵǾ���, ESD�� �Ͽ���, 38mm�� lamina propria ������ ����, ũ�� �̿��� �ٸ� risk factor�� ������, ���������� �����˻縦 �Ͽ������� �ұ��ϰ� ESD �� multiple hepatic metastasis�� ���Ͽ����ϴ�. 9���� �� ���ð�� CT�� �����̾��µ��� ���Դϴ�.
ESD 5�� �� multiple metastasis. Initial ESD pathology: M/D adenocarcinoma, 38x22mm, lamina propria, RM (-), L/V (-/-)
5) ������������ �������� �ʴ� ���Դϴ�. ����� ���ٴ� ���Դϴ�. ���� ���� ������ �ʿ��մϴ�. ESD �� �������������� Ȯ�ε� ȯ�ڿ� ���ؼ��� ���ð� �����˻�� ������ CT �����˻�� ���� �ʰ� �ֽ��ϴ� (���� ���������� ȯ�ڿ��� CT �����˻縦 �ϴ� ������ �ֽ��ϴ�). �������� under-estimation �� ��츦 �����Ͽ� ���������� ȯ�ڿ� ���ؼ� CT�� �����Ͽ��� �Ѵٴ� ������ �� �˰� ������ CT�� �Ѵٰ� ��� ��Ȳ�� ���������� �͵� �ƴմϴ�. CT�� ���������� ġ���� �� ���� ����� �߰��ϴ� �˻� �ƴմϱ�... CT���� ���� ������ ��κ� �̹� �� ���� ��Ȳ�Դϴ�. (Regional node only�� ������ ���� �幮 ��� ����)
����մϴ�. ���ð� �����˻翡�� �������������� ���� ���� �뷫 ���� ���� ���Դϴ�. ESD �� �������������� ��е� ���� �������� �ʽ��ϴ�. ���� �ణ�� ���ܴ� ���� �� �ֽ��ϴ�. ���п��� ���ܰ� ���� ���� �����ϴ�.
[2020-7-10] �� ESD �� adenoma with HGD�� ���� ȯ�ڰ� �ܷ����� D37 �ڵ带 �� �� �ִ°� �����Ͽ� D13.1�� �ϰ� �ִٰ� ������Ƚ��ϴ�. �ڵ�� ���� �����ϴ�. ���������� �ٸ��� �������� �ٸ��ϴ�. ���� �� style�� �ϰ��� �ְ� �����ϴ� ���� ���Դϴ�. ȯ�ڿ� ���ص帰�ٰ� �ڵ带 �����ϰų� ��� �� ���� �ڵ带 ���� ȯ�ڿ��� �ذ� �Ǵ� ��찡 ��κ��Դϴ�. ȯ�ڿ��� �ذ� ���� �ʴ��� �ǻ� ���ο��� �ذ� �˴ϴ�. �׳� �����ϰ� �սô�.
* ����: EndoTODAY �ڵ�
[2021-12-4. �ֵ��� ����] low-grade(moderate) dysplasia
������ �ȳ��Ͻʴϱ�? ��Į���� ���ð��ϴ� �ǻ��Դϴ�. ���� ������������ ������, Tubular adenoma with low-grade(moderate) dysplasia ��� ������ ��찡 ���� �ֽ��ϴ�. �̷��� ������ �� �Ű��� ���Դϴ�. ?
Low-grade(moderate) dysplasia �� low grade dysplasia �� �� � �ӻ����� �ǹ� �� ���� ���̰� �ִ� �Ұ����� �ñ��մϴ�. ���������Բ� ���ǵ帮��, �������� 3�ܰ� �з����̾��ٰ� 2�ܰ� �з������� ����Ǿ��ٰ� �����Ͻð�, 3�ܰ��϶��� moderate �� 2�ܰ迡���� mild �� �Ǿ��ٰ� �����ϼ̽��ϴ�. 3�ܰ� �з����� moderate �� 2�ܰ� �з��������� mild�� �Ȱ��� �ӻ��� ���� �� ���İ� mild�� ����ϱ� ������ ũ�� �Ű澵 �ʿ䰡 ���� ������ ���� ����Ȱ����� �ؼ��ص� �Ǵ�����?
���������� low-grade(moderate) dysplasia ��� ������, �Ű��� ���� ���Դϴ�. ���������Ǿ����� ������ �ǰ���. Ȥ�� ���� �������� ��� ���� low-grade(moderate) dysplasia ��� ��� ���� �ʰ�, ���ǹ� ���ٰ����� �׳� low-grade dysplasia �� ���� ���������Ե� ���� ������ ������ ��ϴ�. ?
�׳� ���������� �� ���� ������, �ӻ��� �ǹ�, ���Ĵ� �׳� low grade �� �� ���� ���ٰ� ���� �Ǵ�����? �ƴϸ� high grade�DZ� ���� �ܰ��̴� �����ؾ� �ȴ� �̷��� �����ؾ� �Ҹ�����? ?
���� ������ �� �� ��� �ٻڽ� �����Բ� ���ǵ帮�� �Ǿ����ϴ�. ��� ���������̷� ���� ����ħ�� �ּż� ���� �ִ� ��ȸ�� �ּż� �� ����帳�ϴ�.
[2021-12-4. ������ �亯]
EndoTODAY ���������� ����/���� ��� �з��� ���Ͽ� ���� �� �ֽ��ϴٸ� �̻����� ���� ���ٰ� �����մϴ�. �ٺ������� interobserver variation�� ����� ��Ȳ���� 2�ܰ�� ������ 3�ܰ�� ������ ������ ������ �����Ƿ� �׳��� �����ڰ� ���̰� ���� 2�ܰ� ��� ���й��� ä�õ� ������ �����ϰ� �ֽ��ϴ�.
������ analogue�ε� �ؼ��� digital�̴� �ָ��� ��찡 ���� �� ������ �� ��� low-grade(moderate) dysplasia��� ��ȣ�� ������� ���´ٰ� �����˴ϴ�. �����ϰ� �����Ͽ� ȯ�� ���κ��� ����ȭ�� ������ �ϴ��� �״��� ��Ȯ���� ���� ���� ���������̹Ƿ� �ִ��� �ܼ��ϰ� �����ϴ� ���� ��ڽ��ϱ�? ���� �׳� low grade dysplasia�� ���Ͽ� ������ �� �����ϴ�.
����ϸ�, low-grade(moderate) dysplasia = low grade dysplasia�� ���� ���� ���ڽ��ϴ�. Keep it simple!
[2022-4-18. YouTube ����]
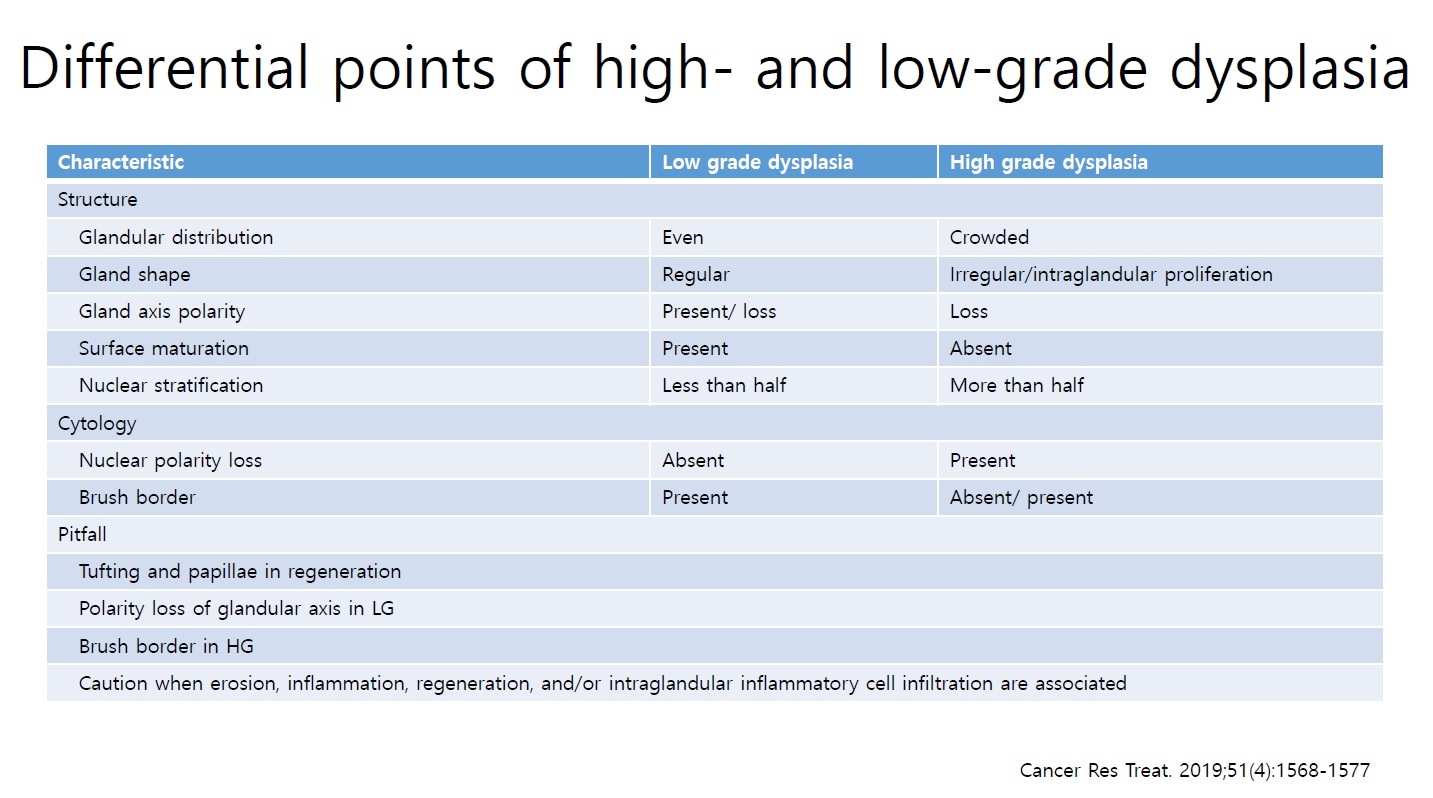
�ȳ��ϼ��� ������ �ٸ��� �ƴ϶� ���庸�� ���� �� �ֽ��ϴ�. ���� ������ ���Ǵ� dysplasia �� �� ũ��� ����� �پ��� pleomorphism�� ���� ��� �ֳ���? Low grade �� high grade �� �����ϴ� ô���� ����, ���� ���������� �����ϴ°Ŷ�� ������µ� �´°��� �ڽ��ϴ�.
[2022-4-19. ������ �亯]
Dysplasia�� ��� ���� ������ �پ��ϰ� �ణ �ְ����� �� �ֽ��ϴ�. ���� �Ʒ��� ���� �ڷḦ �����ϰ� �ֽ��ϴ�. ������ �ǻ簡 �ƴ� ���忡�� ���� �߿��ϰ� �����ϴ� ���� nuclear stratification�Դϴ�. ���������� ���忡�� ���� ũ�Ⱑ ���Ǽ����� ���� �����̸� ����, ���� �̻��̸� ������ �����ϰ� �ֽ��ϴ�.
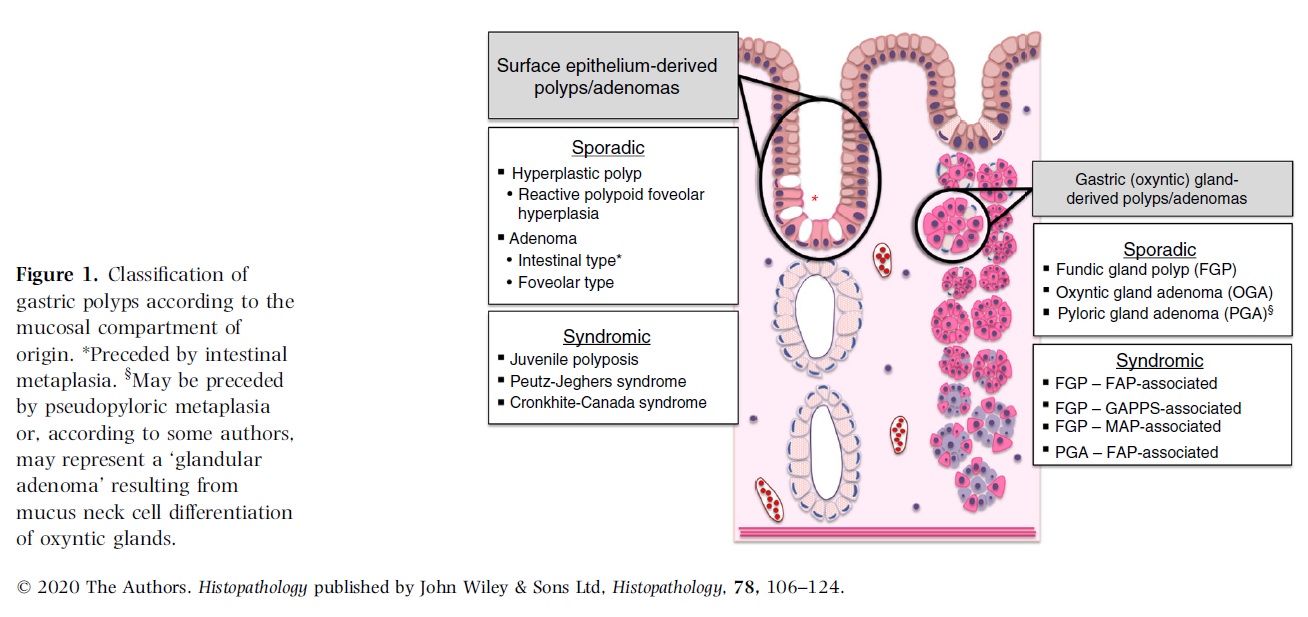
[2025-5-30. �ֵ��� ����] Oxyntic gland adenoma
Oxyntic gland neoplasm�� ���� �����Դϴ�. �ñ��� ���� �����߿� fundic gland polyp�� �ᱹ oxyntic mucosa���� ���ϴ� ���ε� fundic gland dysplasia�� oxyntic gland neoplasm���� �� ���� ���� ������ ���ذ� �� ������ �ʽ��ϴ�. Oxyntic gland neoplasm�̶� �ϸ� Oxyntic gland adenoma �� ADC of fundic gland type�� ���ϰ� fundic gland dysplasia ���� ��� ã�ƺ��� FAP ȯ�ڿ��� �����ؾ��� �����̶���� ���ϰ� �־ ���� ��ü�� ���ϴ�. ���������̿� ����ȯ ���ð� ��Ʋ������ Oxyntic gland adenoma ��ʷ� fundic gland dysplasia�� �Ұ����̴ּµ�, Ȥ�� FAP ȯ�ڰ� �ƴ� ��� fundic gland dysplasia��� ���� �ǵ��� ���´ٸ� oxyntic gland neoplasm���� �� �� �ִ� ���ϱ��? �������� ���� �˼��մϴ�.
[2025-5-30. ������ �亯]
���� ���� �����մϴ�. ���� ���� ��Ȯ�� ����� �� �������� ���߽��ϴ�. �ϴ� ������ ���� WHO blue book (5��)�� tumors of the stomach�� ������ �� ���ñ� �ٶ��ϴ�.
WHO blue book 5��
Gastric gland�� pyloric gland�� fundic gland (= oxyntic gland)�� ���������ϴ�. �� �� ���� gland ��� pit (= foveola)�� proper gland�� �����˴ϴ�. Neoplasm�� pit (= foveolar epithelium)�� proper gland ��ο��� ���� �� �ֽ��ϴ�. ���� �Ʒ��� ���� ������ ������ �ֽ��ϴ�.
Pit Proper gland ��ġ Antrum Body/Fundus Antrum Body/Fundus Non-dysplastic polyp Hyperplastic polyp ? Fundic gland polyp Dysplasia Intestinal type adenoma (=tubular adenoma) and foveolar type adenoma Pyloric gland adenoma Oxyntic gland adenoma Cancer Gastric adenocarcinoma Gastric type adenocarcinoma Adenocarcinoma of fundic gland type Pit (= foveolar epithelium)���� ���ϴ� �͵��� antrum�̳� body/fundus�� ���̰� �����Ƿ� �����ϴ�. WHO blue book 5�� 92�� gastric adenocarcinoma of fundic gland type ������ ���� "This type is assumed to develop from oxyntic gland adenoma."��� �и��� ���� �ֽ��ϴ�. ���� ����� oxyntic gland�� fundic gland�� ���� ���� �ǹ��̸� �ܼ��� ó�� �̸����� ���ʿ� ���� (1) non-dysplastic ���Ҵ� fundic gland polyp����, (2) non-cancer dysplasia ���Ҵ� oxyntic gland adenoma��, (3) cancer�� gastric adenocarcinoma of fundic gland type�� �θ��� ���� ���� �� �����ϴ�. ���� �� �ڴ�� ���� �̸��� ���´ٸ� fundic gland proper���� ���ϴ� ���� ��ȯ�� (1) fundic gland polyp = oxyntic gland polyp, (2) fundic gland adenoma = oxyntic gland adenoma, (3) adenocarcinoma of fundic gland type = fundic gland adenocarcinoma = oxyntic gland adenocarcinoma�� �����ϰ� �ͽ��ϴ�. ����� ������� pyloric gland proper���� ���ϴ� ���� (1) pyloric gland adenoma = gastric gland adenoma, (2) gastric type adenocarcinoma = pyloric adenocarcinoma�� �����ϰ� �ͽ��ϴ�.
�Ʒ��� ���� �����Դϴ�. �̷��� ������ �����ϸ� �� �������?
Proper gland���� ���ϴ� ���ҿ� ���� ������ ���Ͼ� (������ ����. 2025-5-30) ��ġ Antrum Body/Fundus Non-dysplastic polyp ? Fundic gland polyp Dysplasia Pyloric gland adenoma Fundic gland adenoma Cancer Pyloric gland adenocarcinoma Fundic gland adenocarcinoma ���� fundic gland polyp�� �����Ͽ� antrum�� pyloric gland proper���� ���ϴ� polyp�� ���� Ư���� �̸��� ���� �� �����ϴ�. ���� ?ǥ �Դϴ�.
Dysplasia�� adenoma�� ���� ������ �� �ٸ� �����ε�, ���� ������ dysplasia�� ������ adenoma�� �θ��ٰ� �����մϴ�. �̿� ���ؼ��� EndoTODAY ���������� �ڼ��� ����� �ξ����ϴ�.
���� �� ���� �����Դϴ�. ���� ���� ��Ȯ�� ����� �� �������� ���� ������ �ᱹ �������ڵ��� ���� �����ϴٰ� �����ϴ¿� ����� ����Ͽ��µ� �̸� ��� �����ϴ� �۾��� ���� ���� ſ�� ū �� �����ϴ�. Ư�� stomach �κ��� �Ϻ� �����ǻ�� ���� �����ǻ���� �� �ǰ��� ������ ���ϰ� �־ ���� ���ϴ�. ���� �ֱ� WHO blue book�� ���� ���ź��ٴ� ���� ������ �Ǿ� �ֽ��ϴ�. �������� ���Ͼ��� ����������. ����� ���ϴ�.
![]() [References]
[References]
1) ���������� ���ܰ� ġ�� (text, PDF)
2) [Lecture note] Gastric adenoma: to resect, ablate, or not (2014-7-12. 2014 International Hub in Advanced Endoscopy at Konkuk University)
3) Lee SY. Gastric adenoma with low-grade dysplasia: two countries, two outcomes. Dig Dis Sci 2014 (PDF 0.2 M)
4) Shin-Fan Kuan. Pathology of gastric neoplasms (Available in the Internet, PDF 2.0 M)
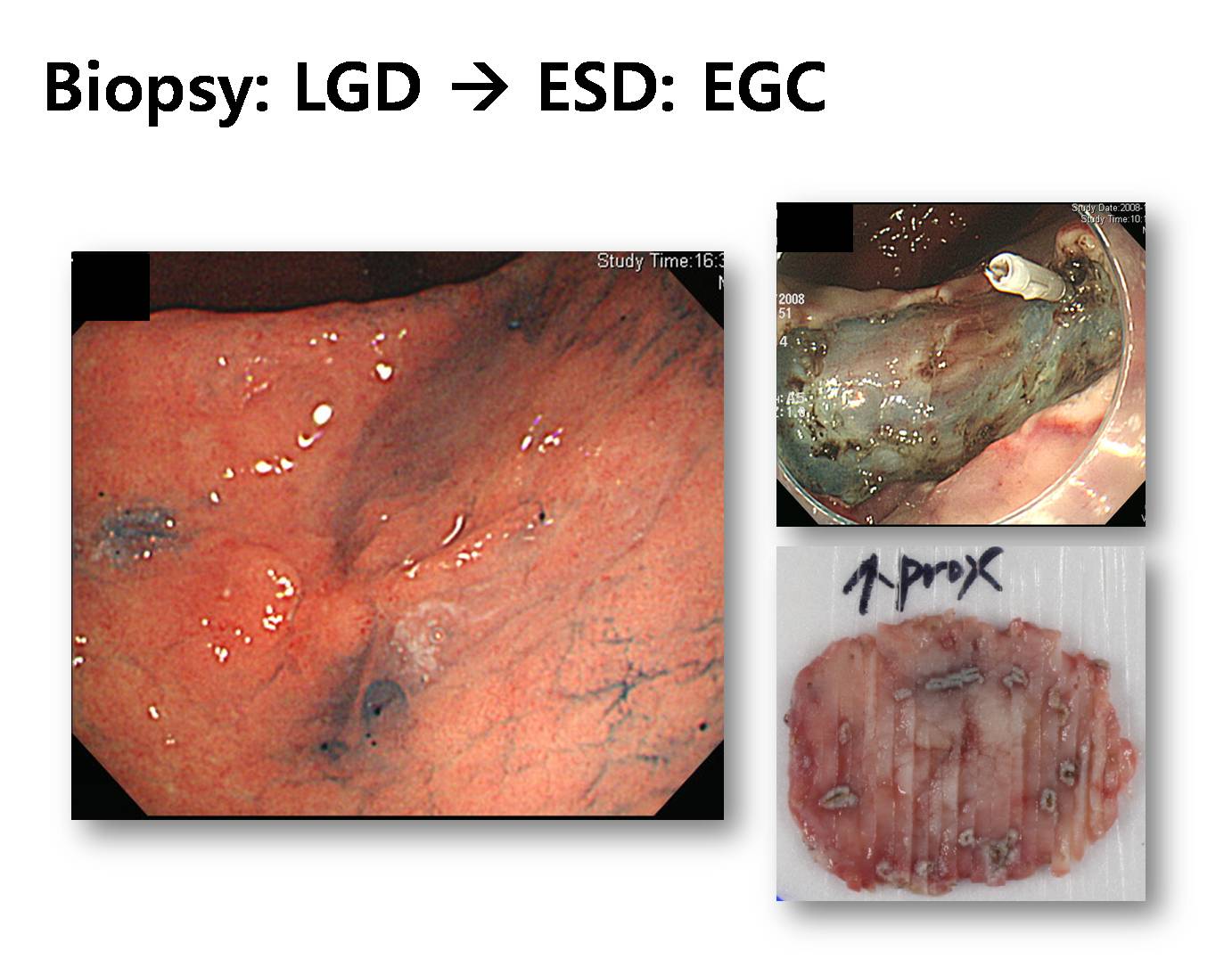
5) A representative case of ESD (biopsy: adenoma, ESD: EGC) (in Korean)
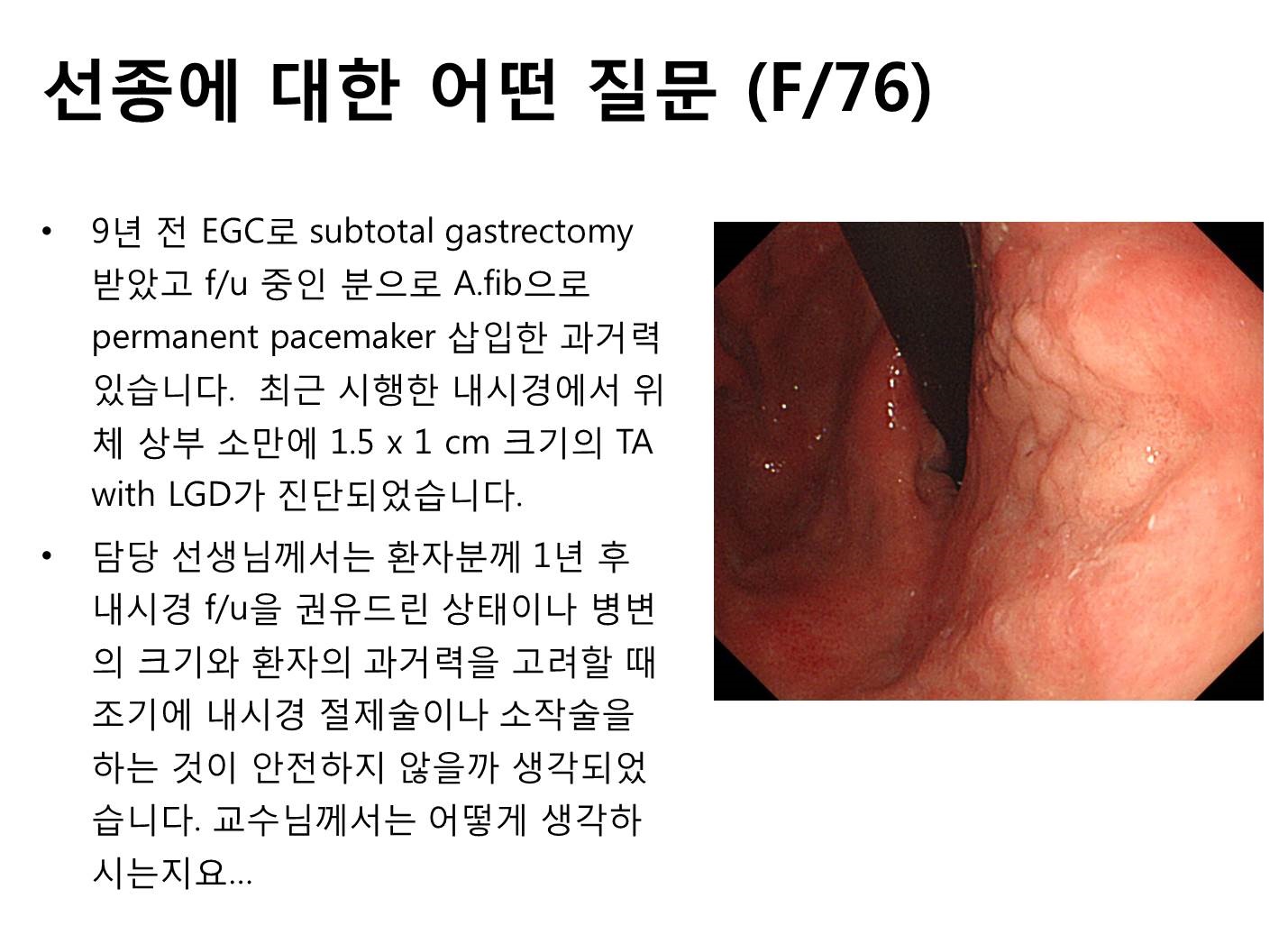
6) � ���� ���� ȯ�� (70��) ��ȣ���� ������ ���Ͽ����ϴ�.
© �Ͽ����ð汳�� �ٸ����ð濬���� ������. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.