EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric neuroendocrine neoplasms including carcinoid tumor] - 終
[Gastric neuroendocrine neoplasms including carcinoid tumor] - 終
2. Histologic diagnosis and clinical staging
3. Surveillance for small type I gastric neuroendocrine tumor (carcinoid)
5. KINGCA 2017 Pathologic findings of gastric NET - 조미연
10. Gastric neuroendocrine carcinoma
11. Lanreotide for metastatic neuroendocrine tumor
12. FAQ
13. References

![]() 1. Classification
1. Classification
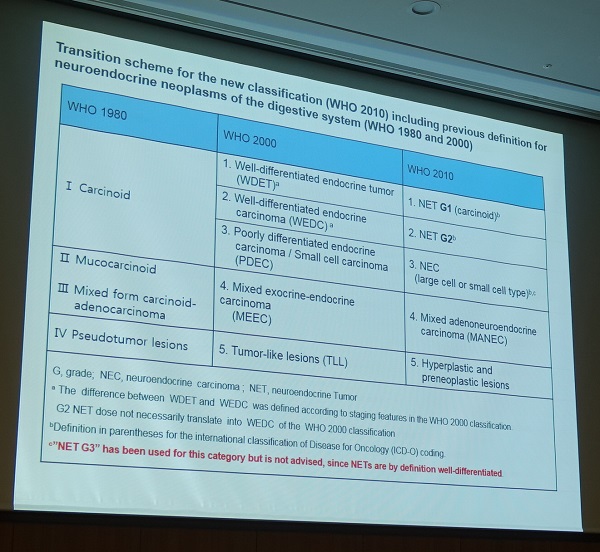
Neuroendocrine neoplasm의 분류는 약 10년을 주기로 계속 바뀌고 있습니다. 2019년 WHO 분류는 아래 표와 같습니다.
| Terminology | Differentiation | Grade | Mitotic count | Ki-67 index |
| NET G1 | W/D | Low | <2 | <2% |
| NET G2 | W/D | Intermediate | 2-20 | 3-20% |
| NET G3 | W/D | High | >20 | >20% |
| NEC, small cell type (SCNEC) | P/D | High | >20 | >20% |
| NEC, large cell type (LCNEC) | P/D | High | >20 | >20% |
| MiNEN | W/D or P/D | Variable | Variable | Variable |
췌장의 NET는 Ki-67이 20%를 한참 초과할 수 있습니다. 이 때문에 2019년 WHO 분류에 NET G3가 새롭게 추가되었습니다. 2010년 WHO 분류에서는 NET G1, NET G2, NEC만 있고 NET G3가 없었습니다. Unlike G3 NECs, G3 NETs usually have a Ki-67 index below 55% and a prognosis not as poor as G3 NECs (WJGO 2020). Gastric NET 중에도 G3가 있는지 잘 모르겠습니다. 저는 2023년 현재까지 Gastric NET G3, 즉 well-differentiated이면서 G3인 경우를 한 번도 본 적이 없습니다.
MiNEN (mixed neuroendocrine-non-neuroendocrine neoplasms)는 두 요소가 30%이상 차지할 때 사용합니다. 2000년 WHO 분류에서는 mixed exocrine-endocrine carcinoma (MEEC), 2010년 WHO 분류에서는 mixed adenoneuroenocrine carcinoma (MANEC)으로 불리던 것입니다. 이름이 계속 바뀌고 있습니다. 이유는 모르겠습니다.
NET와 NEC는 여러 측면에서 관련이 없습니다 (unrelated). 완전히 다른 질병으로 이해하는 것이 나을 것입니다. 과거에는 well-differentiated NET가 metastasis를 보이면 NEC로 불렀지만 지금은 poorly-differentiated neoplasm만 NEC로 부르고 있습니다.
Another characteristic feature of NETs is the expression of somatostatin receptors (in particular, abundant SSTR2), which can be detected by immunohistochemistry or using functional radiographical imaging, such as octreoscan and 68Ga-DOTATOC/DOTATATE/DOTANOC PET-CT.
Type 3 NET의 내시경 치료 후 국소재발을 DOTATATE PTE-CT로 확인 (위질환내시경아틀라스 136쪽)
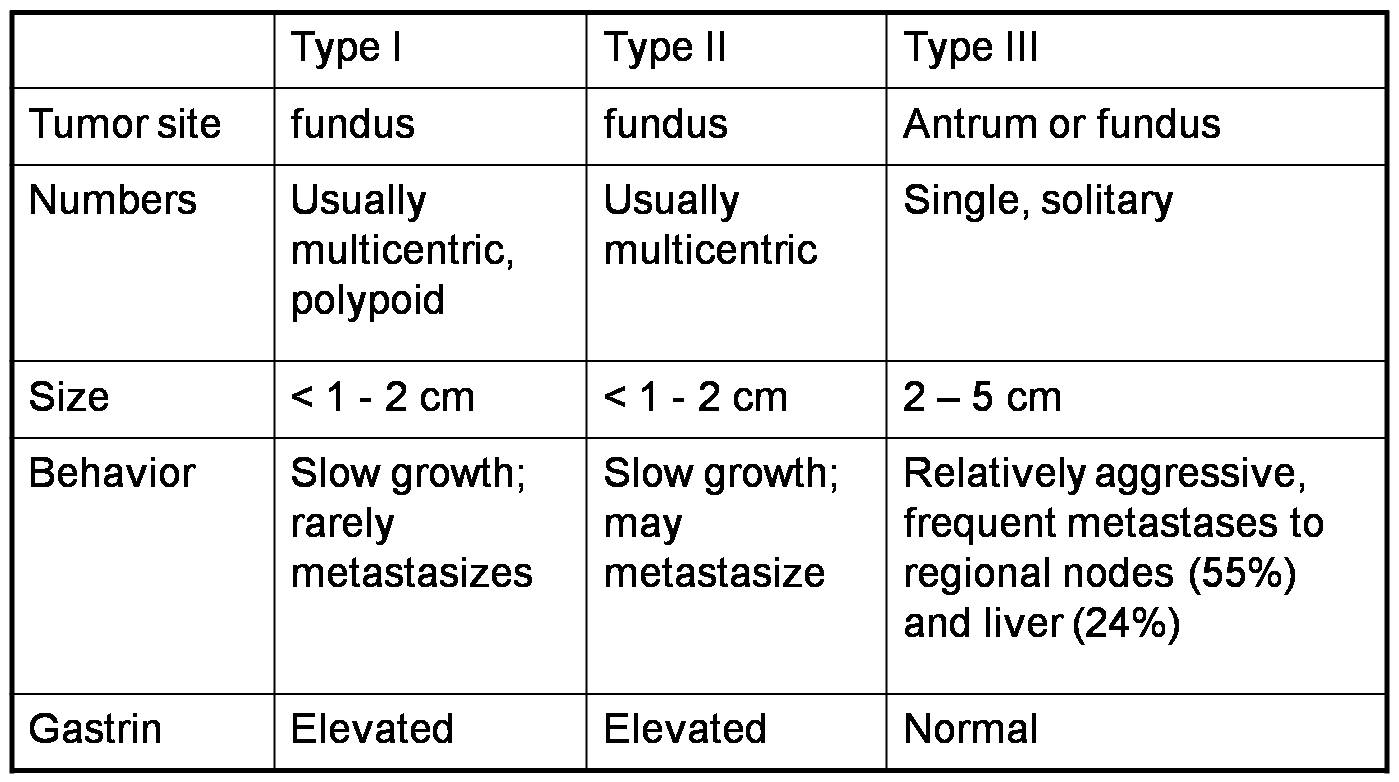
Gastric neuroendocrine tumor (NET)는 몇 가지 임상적 특징에 따라 세 종류로 나누고 있습니다. Neuroendocrine carcinoma (NEC)는 여기에 포함되지 않습니다. 전혀 다른 질병으로 이해하는 것이 나을 것 같습니다.
문제는 type 1의 정의입니다. 유명한 Rindi의 1993년 Gastroenterology 논문에서는 "twenty-eight cases, none metastatic, arose in a background of body-fundus atrophic gastritis and hypergastrinemia"와 같이 애매하게 씌여 있습니다. Serum gastrin이 더 중요한지 atrophy가 더 중요한지 언급되어 있지 않습니다.
Atrophic gastritis도 현저하고 hypergastrinemia가 있으면 1형으로 분류하는 것은 문제가 없습니다. Atrophic 하지도 않고 gastrin도 정상이면 3형으로 분류하는 것도 대강 받아들일 수 있습니다. 그런데 atrophic 하지만 gastrin은 정상이거나, atrophic하지 않은데 gastrin이 높은 경우는 애매합니다.
Original article에서는 gastrin을 중요시합니다. High gastrin이면 1형으로, normal gastrin이면 3형으로 분류합니다. 쉽고 명료하고 객관적이기 때문입니다. 2018년 삼성서울병원 민병훈 교수님께서 Br J Surg에 보고한 논문 Clinicopathological features and outcome of type 3 gastric neuroendocrine tumours에서도 3형의 정의는 "biopsy-proven gastric NET and a normal fasting serum gastrin level"이었습니다. 2016년 대한상부위장관헬리코박터학회지 발표된 우리나라 다기관 공동연구(Lee HS. KJHUGIR 2016)에서 1형의 기준을 hypergastrinemia로 삼았습니다 ("To classify tumors as type 1 gastric NETs, patients’ plasma gastrin levels were analyzed and other associations, such as Zollinger-Ellison syndrome (ZES) or multiple endocrine neoplasia type 1, were ruled out.")
Review article에서는 atrophy를 중요시합니다. 혹은 atrophy와 gastrin을 둘 다 언급하고 있습니다.
Rindi 분류에서 atrophic gastritis를 중요시하였던 문헌
치료법 결정에서 hypergastrinemia가 중요한 것처럼 되어 있지만 자세히 살펴보면 저자가 atrophic gastritis와 hypergastrinemia를 섞어서 기술하고 있는 문헌. 즉 normal gastrin + atrophic gastritis에 대한 설명이 없는 문헌
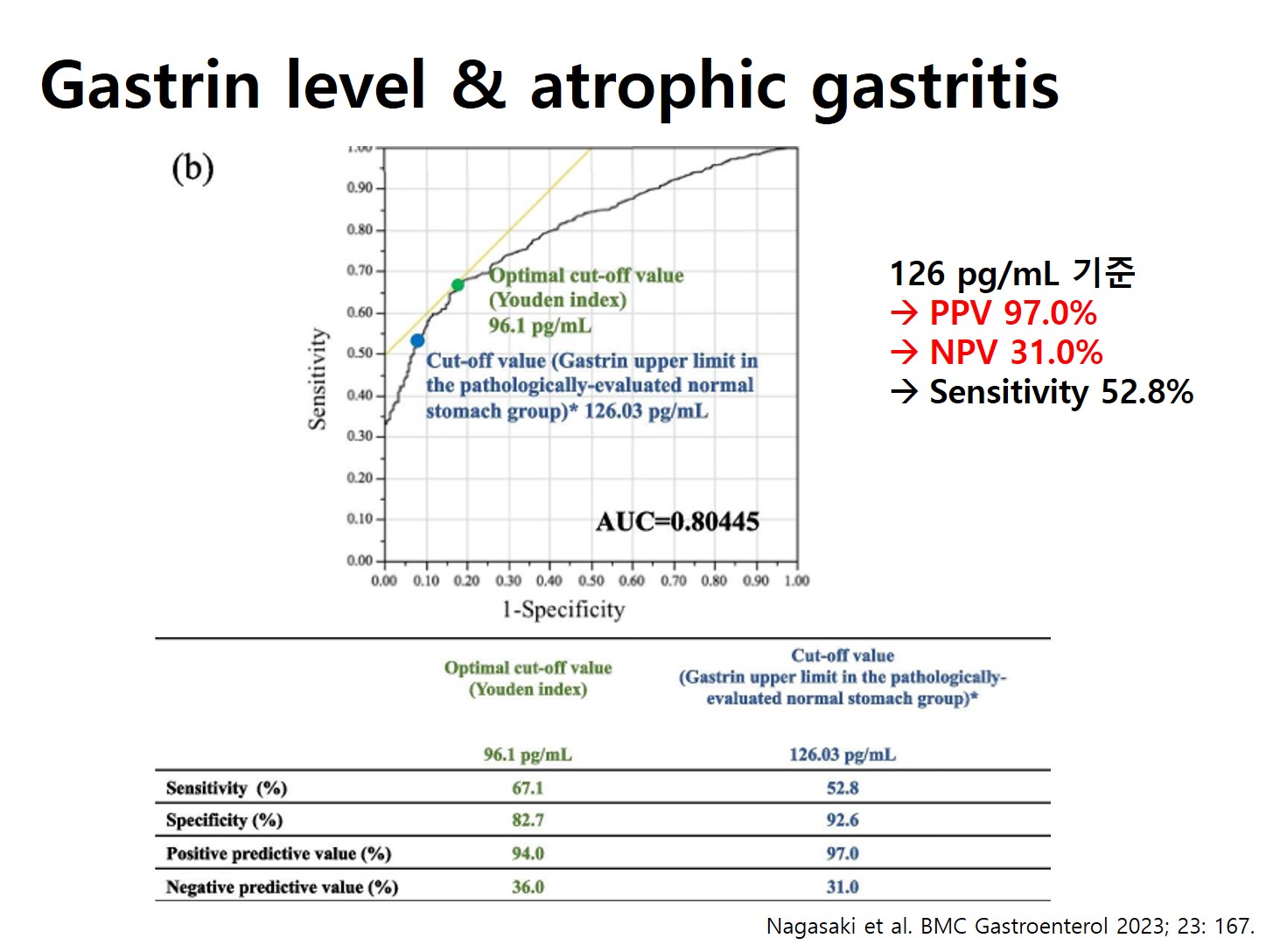
Gastrin과 atrophy와의 연관성을 분석한 자료는 아래와 같습니다.
이러한 내용을 정리하면 아래 표와 같습니다. Original article에서는 gastrin이 중요하고 review article에서는 atrophy가 중요합니다.
| Atrophic | Non-atrophic | |
| High gastrin | 1형 | Original article에서는 1형 Review article에서는 3형 |
| Low gastrin | Original article에서는 3형 Review article에서는 1형 | 3형 |
임상 현장에서는 애매한 경우가 많습니다. Gastrin level과 atrophy가 일치하지 않는 경우가 많기 때문입니다. Atrophy의 기준도 애매합니다. 내시경 소견의 관찰자간 차이도 걱정이고, pepsinogen을 고려할지 말지도 고민입니다. 그래서 case by case로 접근할 수 밖에 없습니다. 아래 증례를 참고하시기 바랍니다.
[증례: Rindi 분류가 애매한 경우 - Atrophic gastritis를 중요시 할 것인가? Gastrin level을 중요시 할 것인가?]
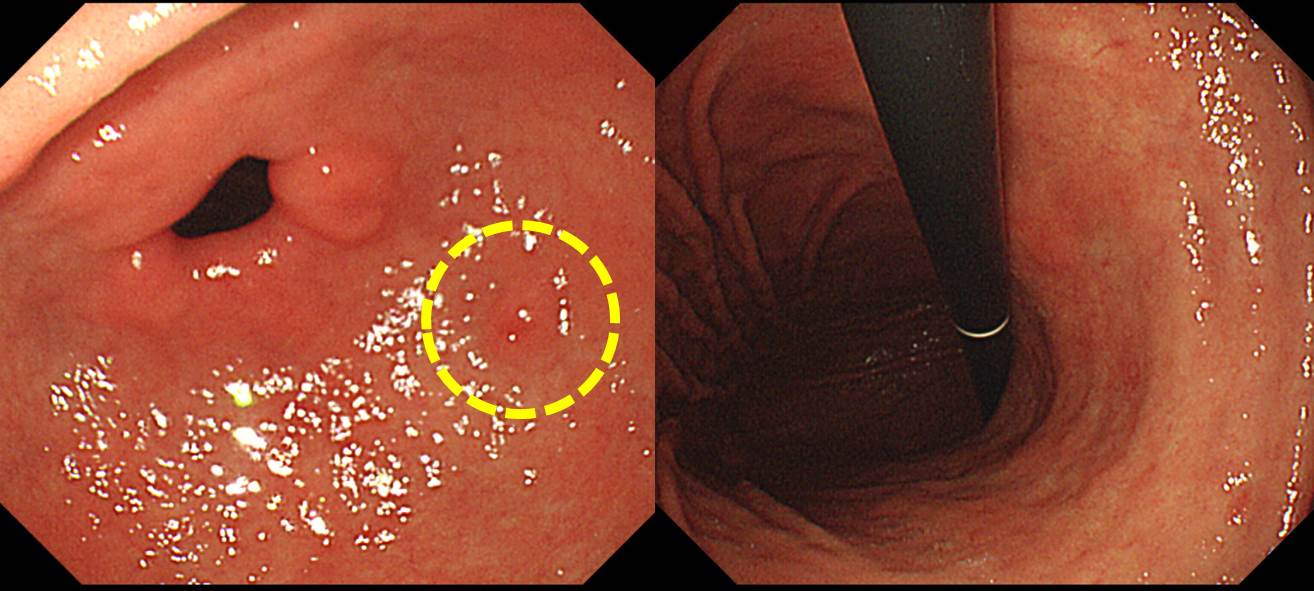
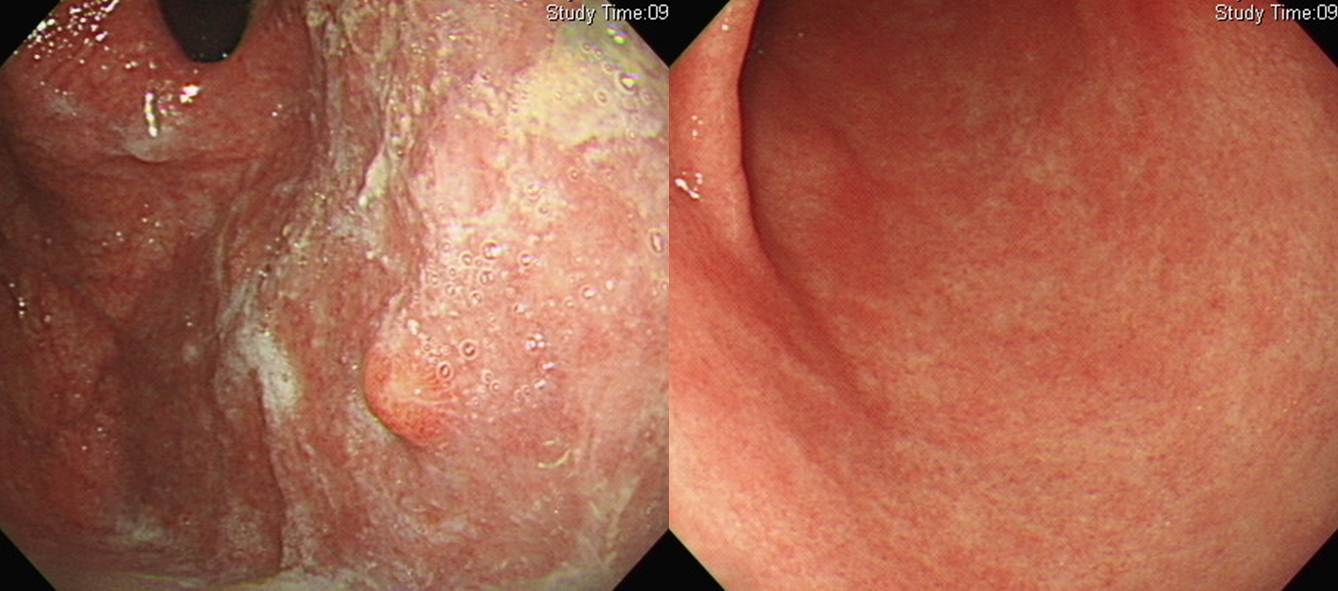
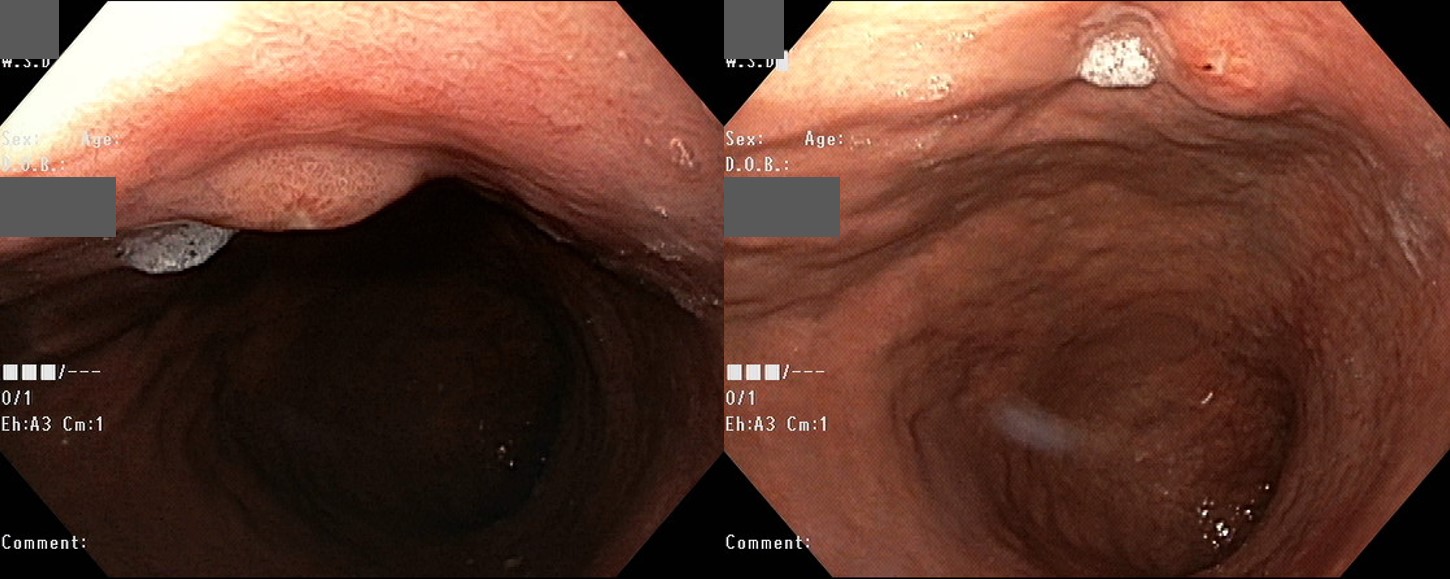
대장암 수술 후 경과관찰 중인 분에서 우연히 발견된 neuroendocrine tumor입니다. 매우 작았습니다. 조직검사는 WELL DIFFERENTIATED NEUROENDOCRINE TUMOR로 나왔습니다. 과거 유암종으로 불렀던 것입니다. 헬리코박터 양성이었습니다. Gastrin은 31.5로 정상이었습니다. 여러분은 어떻게 하시겠습니까?
상황은 단순하지 않습니다. 왜냐하면 내시경 사진을 보면 뚜렷한 위축성 화생성 위염이 있기 때문입니다 (화생성 위염은 조직검사로도 확인되었습니다). 위축성 위염을 기준으로 하면 1형이고 gastrin level을 기준으로 하면 3형입니다. 1형은 '경과관찰 + 헬리코박터 제균치료' 정도면 충분하고 3형은 내시경 절제술이 필요한데 Rindi 분류가 애매하니 치료방침도 애매합니다.
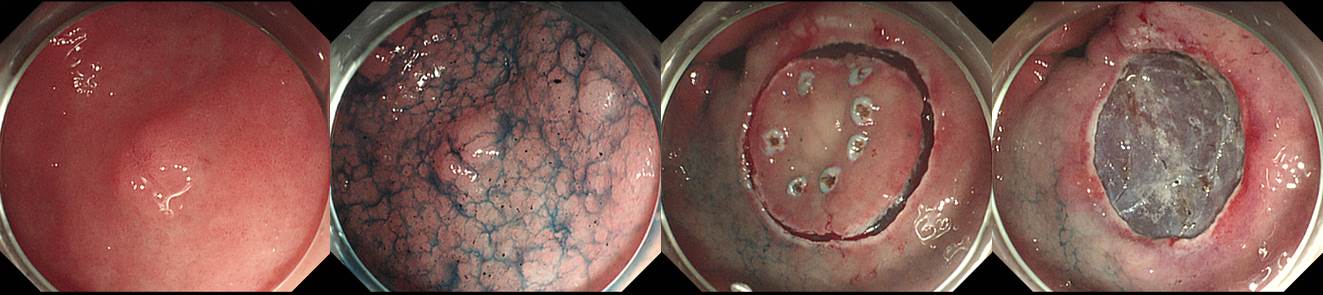
이럴 때에는 최대한 보수적으로 안전한 방향을 택합니다. Normal gastrin이라는 것을 고려하여 내시경 절제술을 하였습니다. 덤으로 헬리코박터 제균치료도 해 주었습니다. 물론 과잉 치료일 수도 있습니다. 여하튼 최대한의 치료를 하였습니다. 경과관찰 필요성도 적어서 마음도 편합니다.
내시경 절제술을 쉽고 안전하게 할 수 있는 상황이라면 그냥 복잡하게 생각하지 않고 절제술을 하면 되겠습니다 (실제 이 환자는 10여분 걸렸습니다). 내시경 절제술이 매우 까다로운 부위라면… 그때는 이런 저런 고민이 필요합니다. 비록 gastrin 수치는 정상이지만 현저한 atrophic gastritis를 고려하여 헬리코박터 제균치료만 하고 경과관찰을 할 수도 있지 않나 생각됩니다.
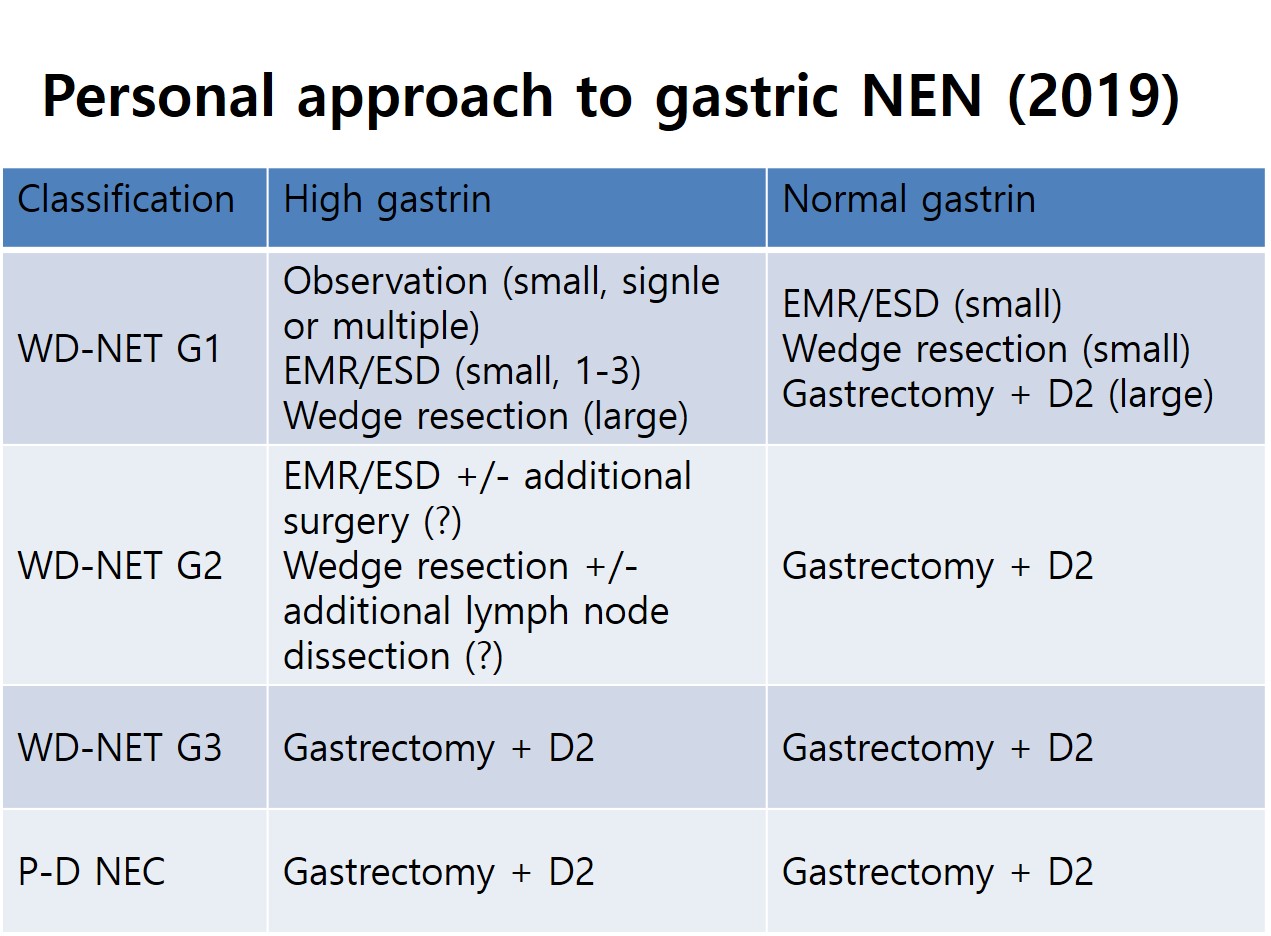
분류상의 모호한 점을 고려하여 저는 아래와 같은 방법으로 치료원칙을 정하고 있습니다. Gastrin을 중시하되 크기가 작으면 1형과 비슷한 방법으로 접근하는 방식입니다. 여전히 모호한 점이 적지 않지만...
![]() 2. Histologic diagnosis and clinical staging - G2를 중심으로
2. Histologic diagnosis and clinical staging - G2를 중심으로
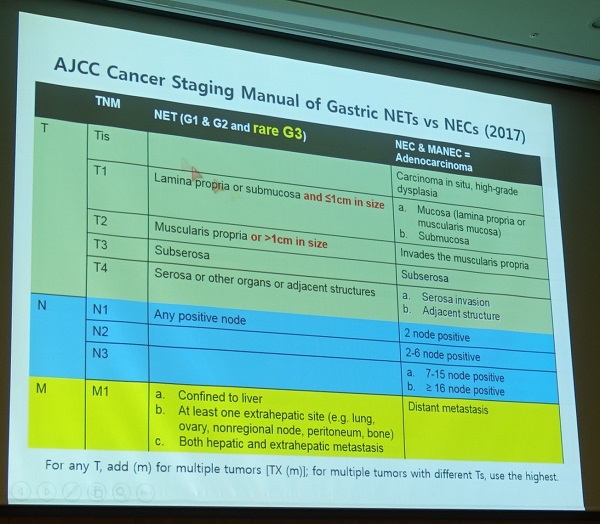
[TNM classification for gastrid well-differentiated NETs (G1 and G2)
T1: tumor invades mucosa or submucosa and 1cm or less in greatest dimension (크기가 포함된다는 점이 특징입니다.)
T2: Tumor invades muscularis propria or is more than 1 cm in greatest dimension
T3: Tumor invades subserosa
T4: TUmor perforates visceral peritoneum (serosa) or invades other organs or adjacent structures
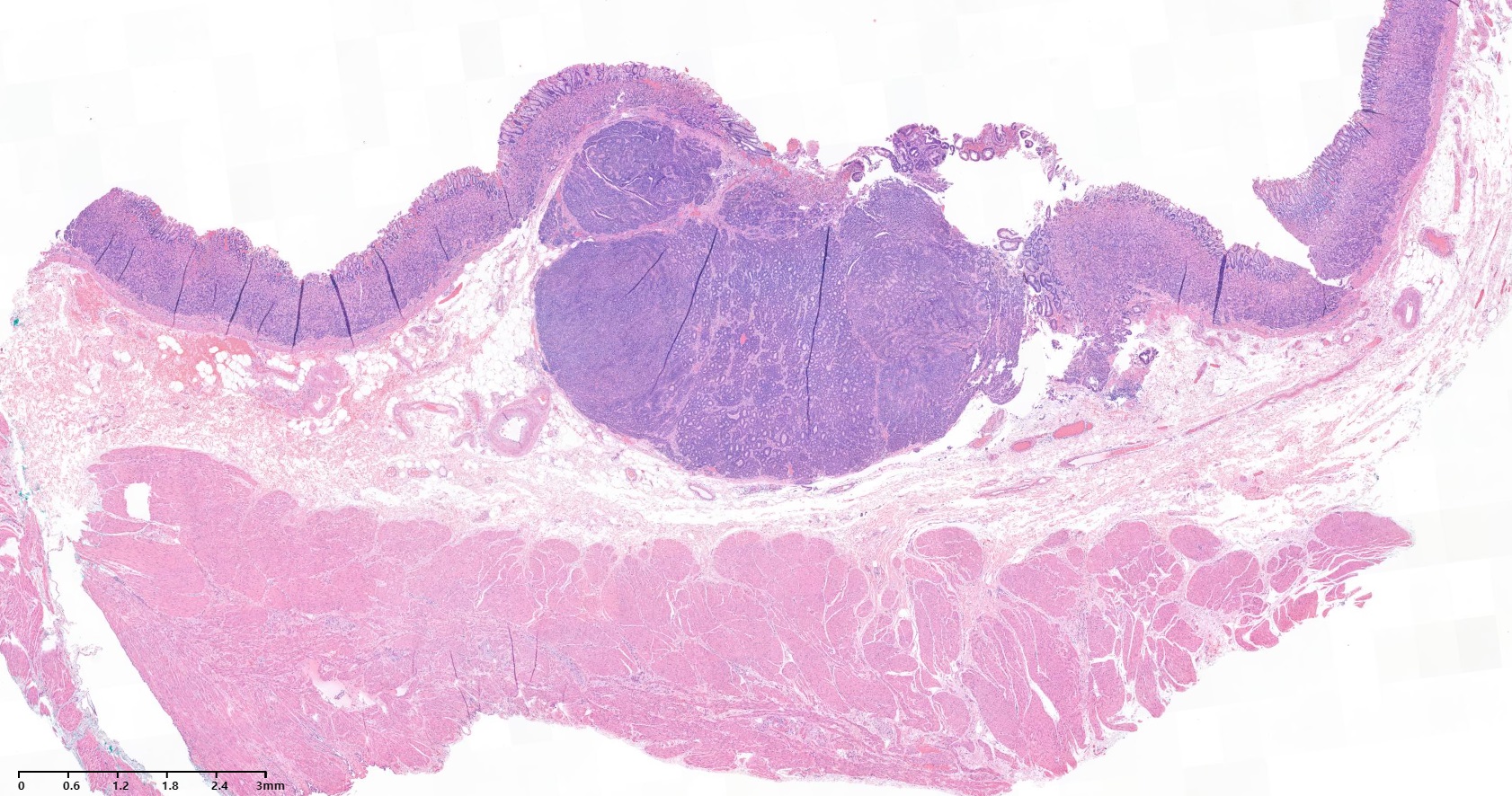
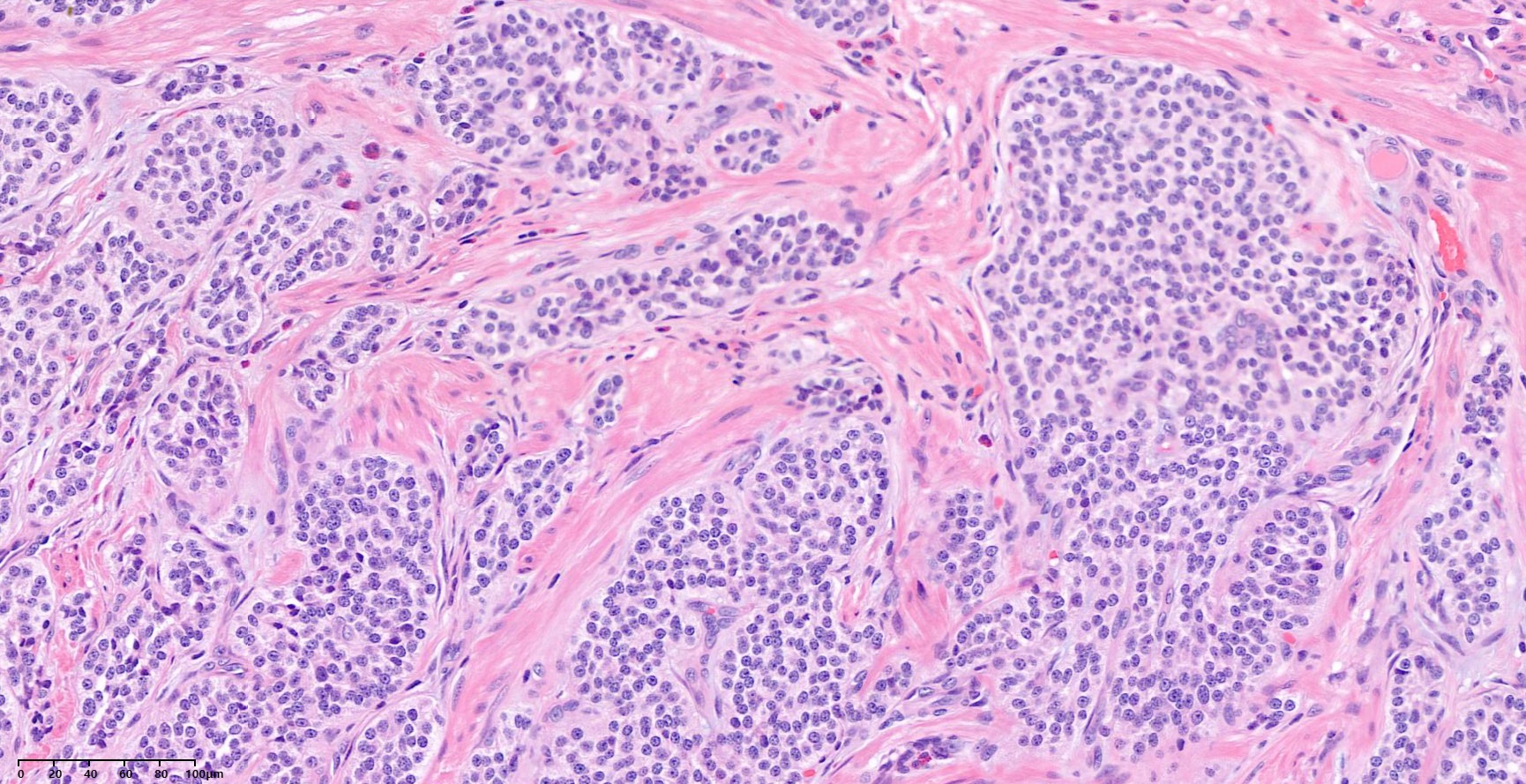
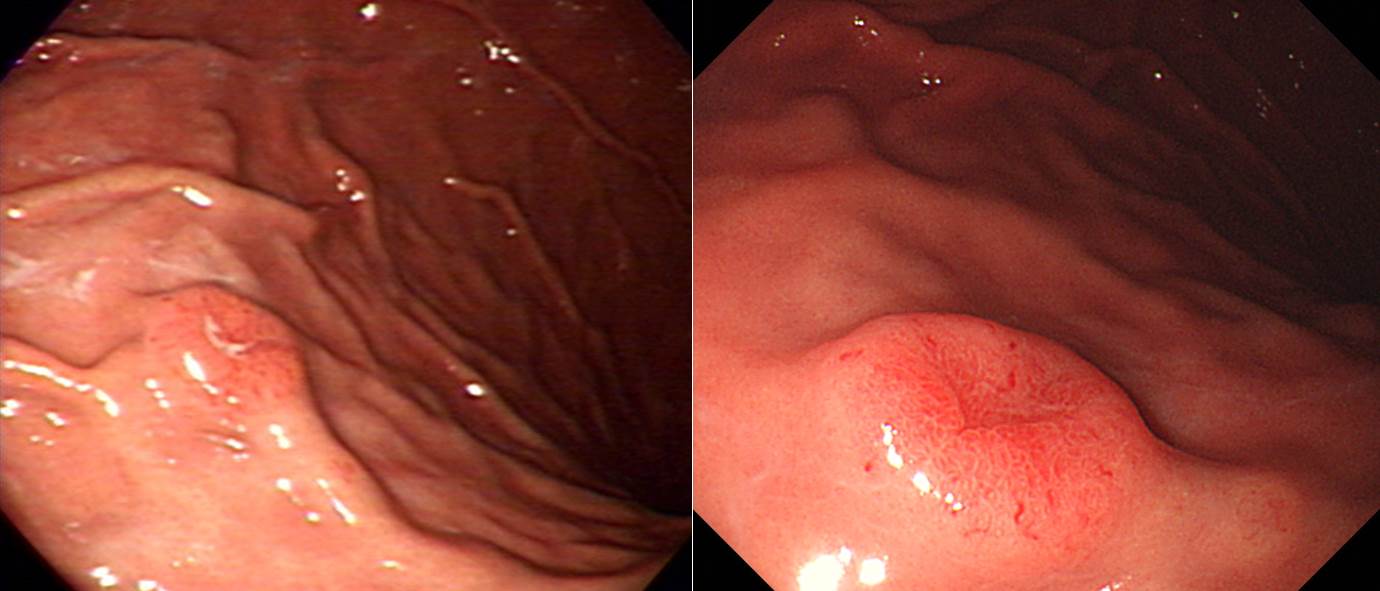
Granular cell tumor 같다는 조직검사 결과로 의뢰된 분으로 ESD를 시행하였습니다.
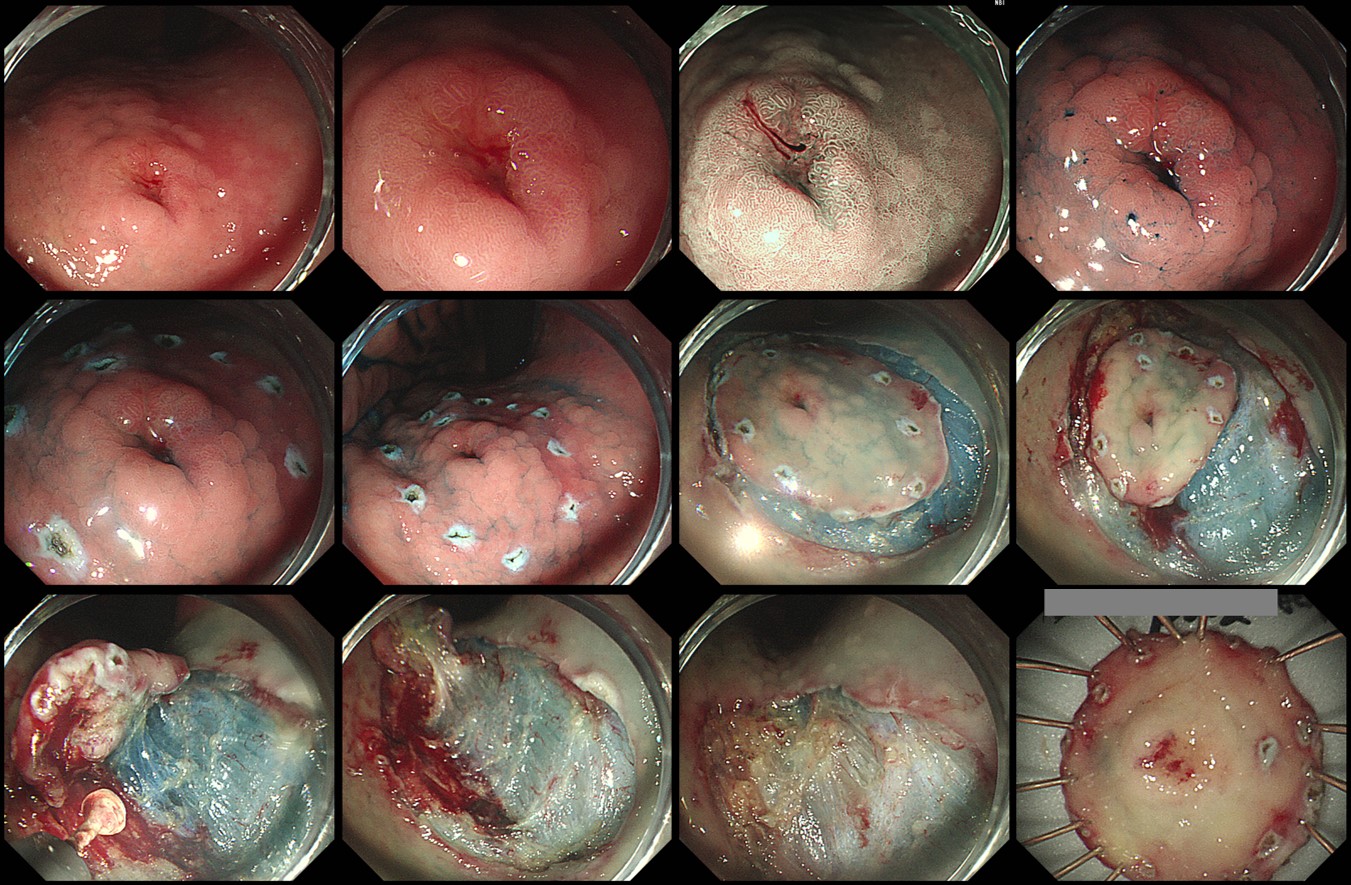
ESD: Well differentiated neuroendocrine tumor (G2)
1. Name of Procedure: ESD
2. Site of Tumor: Stomach (anterior wall of mid body)
3. Diagnosis: Neuroendocrine tumor
4. WHO classification(2010): Well-differentiated Neuroendocrine tumor (G2)
5. Multiplicity: Single
6. Size: 1.0x0.8x0.3 cm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic Count(/10HPF): 2-20, Ki-67 labeling index: 4%
9. Immunohistochemical Stains: 1) Synaptophysin : Positive, 2) Chromogranin A: Positive
10. Lymphovascular invasion: Not identified
11. Perineural invasion: Not identified
12. Lymph node metastasis: not evaluated
13. Resection Margins: Negative
위 신경내분비종양은 무척 혼동스러운 질병입니다. 우선 이름부터 헷갈립니다. Neuroendocrine tumor와 carcinoid의 경계가 불명확하기 때문입니다. 치료 원칙도 staging에 따라 결정되지 않고 type과 grading이 중요하고 staging이 보조적인 역할을 하기 때문에 grey zone이 많습니다. 그리고 문헌에서 제시된 방법대로 임상에서 적용되고 있는 것도 아닙니다. 암인지 아닌지 명확하지 않기 때문에 coding에서도 논란이 많습니다.
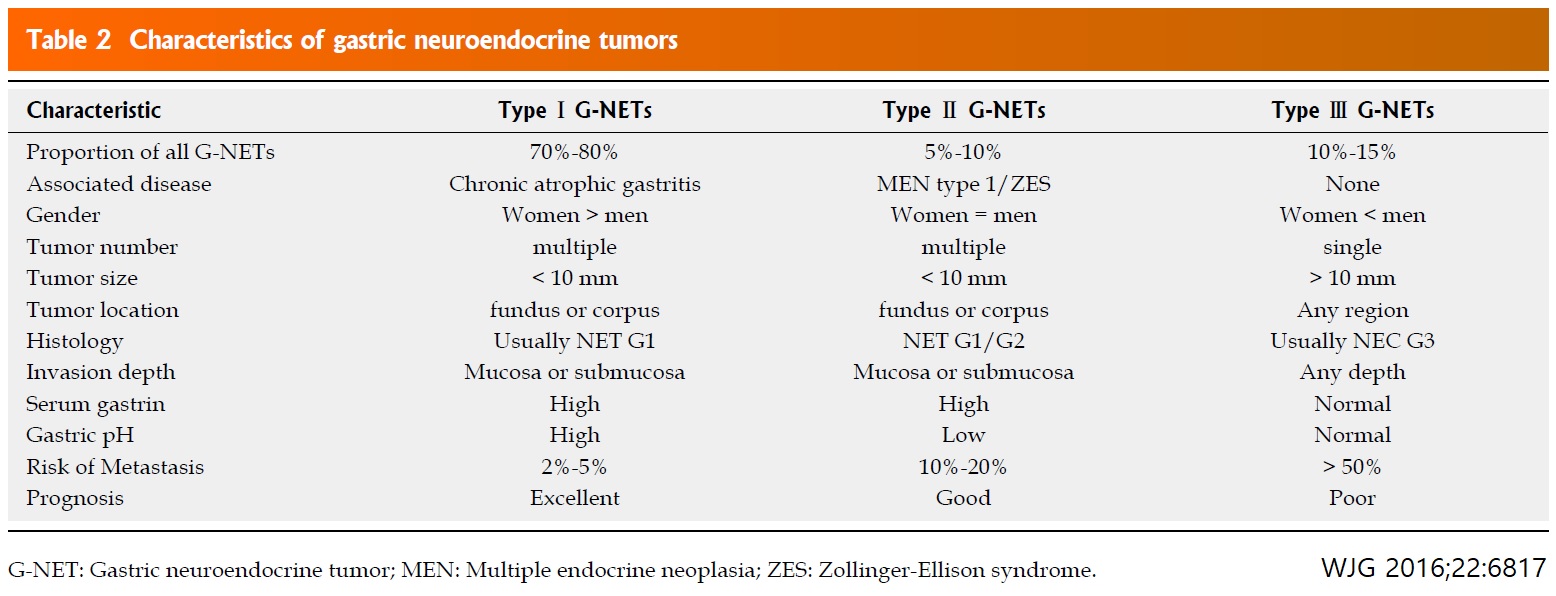
고신대학교병원 박무인 교수님의 Endoscopic treatment for early foregut neuroendocrine tumors에서 잘 정리된 table 두개를 아래에 옮깁니다.
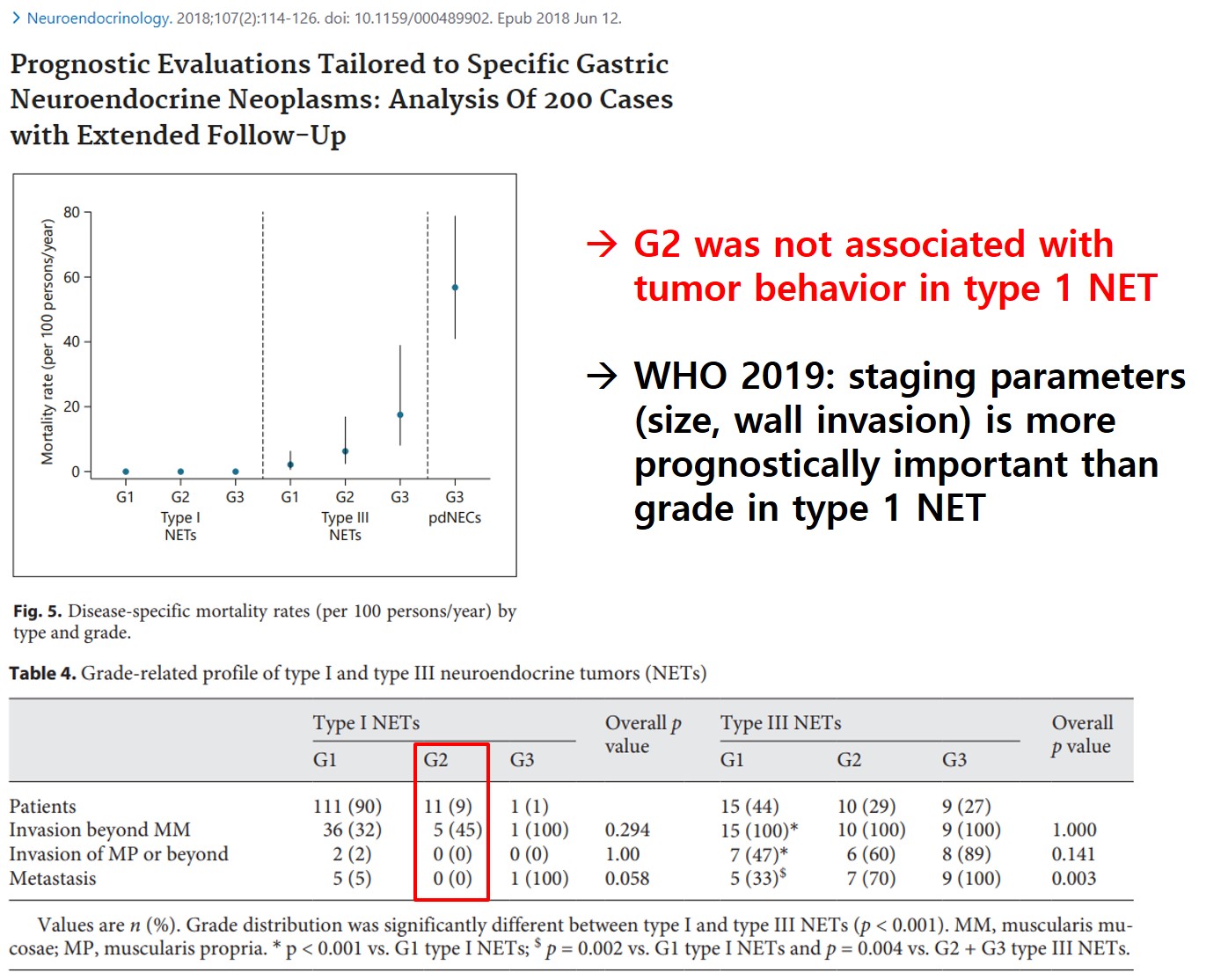
저는 위 신경내분비종양을 일종의 spectrum으로 생각하고 있습니다. 가장 좋은 종류는 (1) Rindi type 1, (2) T1N0M0, (3) 1cm 이하, (4) 병리학적 grade 1인데 경과관찰을 선택할 수 있습니다. 가장 나쁜 형태는 neuroendocrine carcinoma입니다. 문제는 그 중간도 많고 애매한 경우도 적지 않다는 것입니다. 특히 '경과관찰 - 내시경 절제술 - 수술'이라는 세 치료법의 경계에 해당하는 환자들에게 어떠한 치료를 권하는 것이 좋을지 늘 고민하고 있습니다. 예를 들어 fundus의 작은 병소에 대한 조직검사에서 병리학적 grade 2로 나온 경우 앞 table에 따르면 surgery를 권해야 합니다. 그런데 grade 2로 나온 근거가 mitotic index 2/10 HPFs (기준: 2-20) Ki-67 labeling index 3-4% (기준 3-20%)로 기준의 하한선을 살짝 넘은 것이 전부라면 어떻게 해야 좋을까요?
G2는 type 1 NET의 tumor behavior에 큰 영향이 없다는 주장도 적지 않습니다.
원칙을 따르는 수 밖에 없을 것 같습니다. 애매한 경우의 원칙은 늘 이러합니다. 최대한 자세히 설명하고 환자의 선택을 존중한다.
[환자 설명문 - Small and Grade 2 (G2)]
작은 위신경내분비종양에 대한 내시경절제를 하였는데 병리학적으로 grade 2(G2)가 나온 상황입니다. 일단 암 코드로 변경하겠습니다.
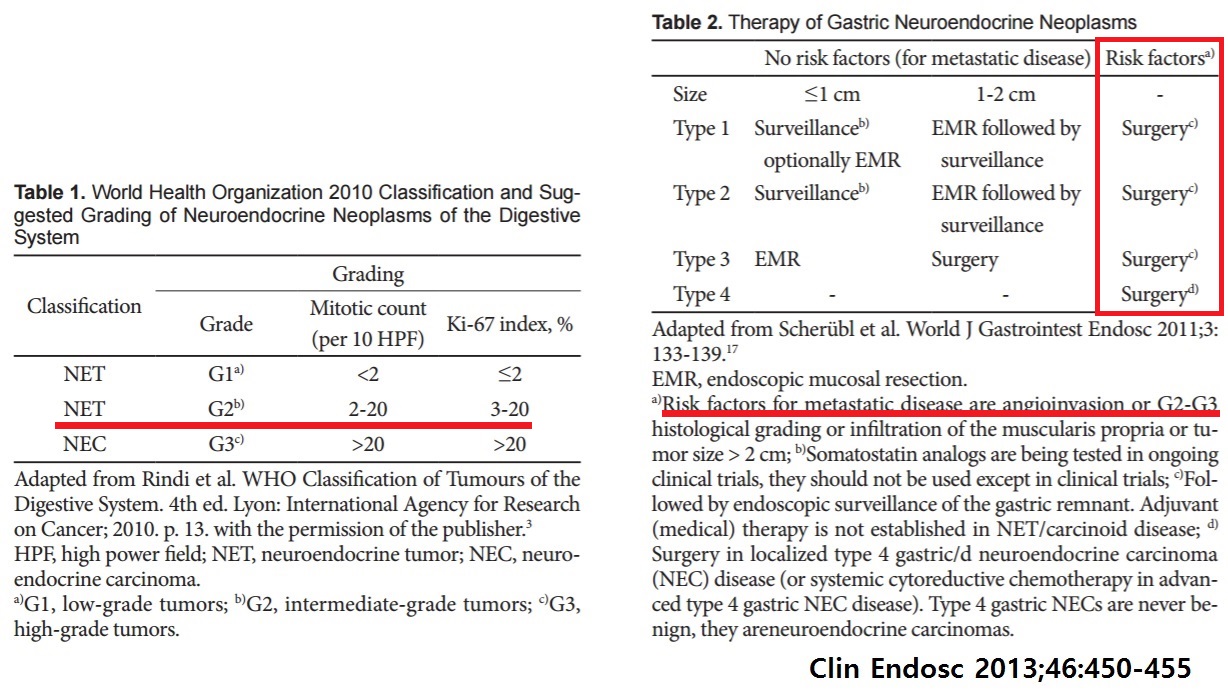
전문가의 글에서 가져온 Table에 따르면 수술을 권해야 마땅합니다. 왜냐하면 신경내분비종양은 재발위험인자 (G2는 유명한 재발 위험인자입니다)가 있으면 모든 경우 수술을 하도록 되어 있기 때문입니다. 그런데 작은 G2라면 위험인자 중에는 약한 편에 속합니다. 이 정도까지 꼭 수술을 권해야 하는지 의사마다 의견이 다양할 수 있습니다.
수술을 하게 되면 재발률을 약간 줄일 수 있을 것입니다. 그러나 수술은 수술입니다. 위를 전부 (혹은 최소한 2/3) 잘라야 하고 주변 림프절까지 박리하기 때문에 수술에 따른 합병증과 수술 후 삶의 질 저하를 함께 고려해야 합니다. 전신마취의 위험도 무시할 수 없습니다.
제일 큰 문제는 데이타가 없다는 것입니다. 양쪽 극단은 많습니다. 매우 작고 G1인 경우나 매우 커서 틀림없이 암인 경우는 종종 만날 수 있습니다. 그런데 작은 종양인 G2는 무척 드문 상황입니다. 몇 년에 한 명 뵐까 말까 합니다. 현대 의학은 근거 중심으로 이루어집니다. 그런데 자료가 없으니 정확한 판단 근거가 없는 상황인 셈입니다. 이러한 경우 의사들은 전문가 의견을 따르는 경우가 많습니다. 앞서 설명드린 table입니다. 수술을 권하는 것이 표준입니다. 수술 이외의 선택을 하였을 때 어떤 결과가 예상되는지를 알 수 없습니다. 의사의 감으로는 안 해도 될 것 같은데... 표준 지침은 수술이니... 이러지도 못하고 저러지도 못하는 상황, 의사마다 추천이 다른 상황일 수 밖에 없습니다.
의사마다 추천이 다른 수 밖에 없는 상황입니다. 그래서 저희는 최대한 자세히 설명하고 환자의 선택을 존중하고 있습니다.
일단 1주일 후 외래를 잡아놓겠습니다. 가족간 잘 상의하시고 최종 결론을 가지고 1주일 후 외래를 방문하여 주시기 바랍니다.
현실적으로 작은 NET이고 비록 점막하침윤이 있더라도 병리학적 완전절제가 된 경우 G2에서 수술을 선택하는 환자는 많지 않습니다.
[2026-5-28] 위암학회 다학제 집담회. (1) 간이식 환자의 위암 ESD, (2) LECS


위 NET에 대한 메타분석(Dig Endosc 2025)에서 림프절 전이는 type 1에서 6.0%, type 2에서 38.5%, type 3에서 23.2% 였으며, 위험인자는 tumor size >10 mm (4.18), tumor invasion into the muscularis propria or deeper (11.21), grade 2/3 (5.96), and lymphovascular invasion (34.50) 였습니다. 1.5cm 보다 작은 직장 NET 652예에 대한 우리나라 다기관 후향적 연구 (Gut Liver 2021)에서 75예 (11.5%)에서 lymphovascular invasion이 있었고, 수술을 시행한 41예의 48.8% (20/41)에서 림프절 전이가 있었습니다.
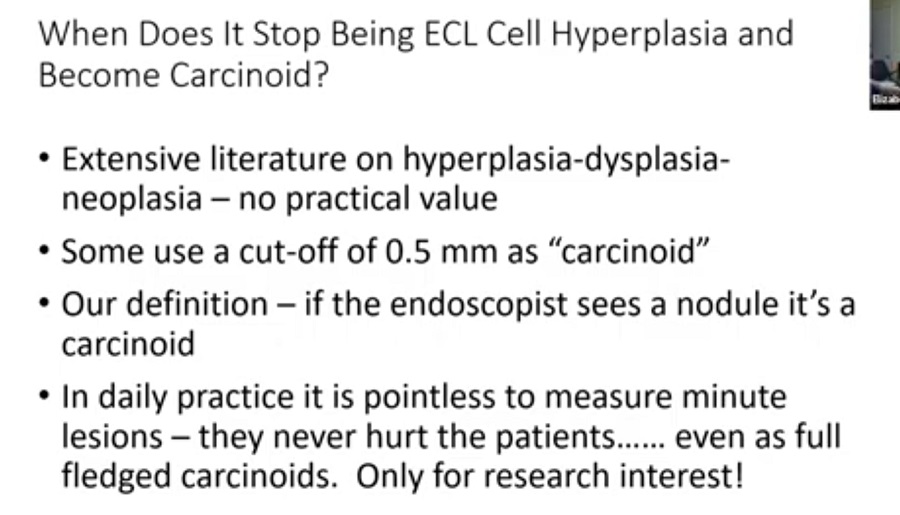
[한 병리학자의 신선한 주장] Neuroendocrine hyperplasia, neuroendocrine dysplasia, carcinoid의 구분이 그다지 중요하지 않다는 것입니다. 자가면역성 위염 autoimmune gastritis 환자에서 type 1, hypergastrinemia를 동반한 NET에 대한 이야기 같습니다. Helicobacter-associated에서는 어떻게 하는 것이 좋을지 고민입니다.
![]() 3. Surveillance for small type I gastric neuroendocrine tumor (carcinoid)
3. Surveillance for small type I gastric neuroendocrine tumor (carcinoid)
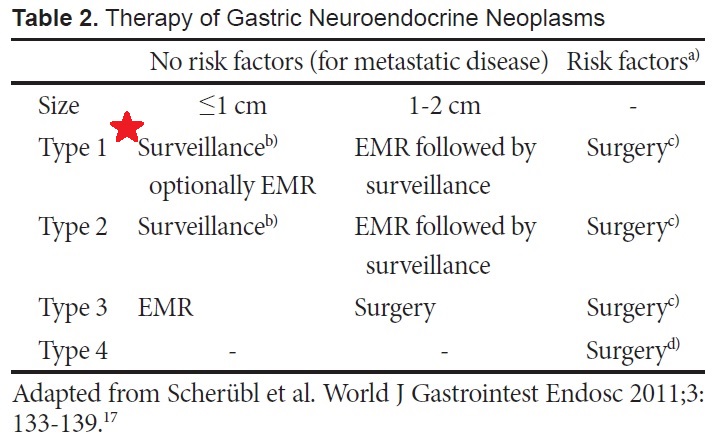
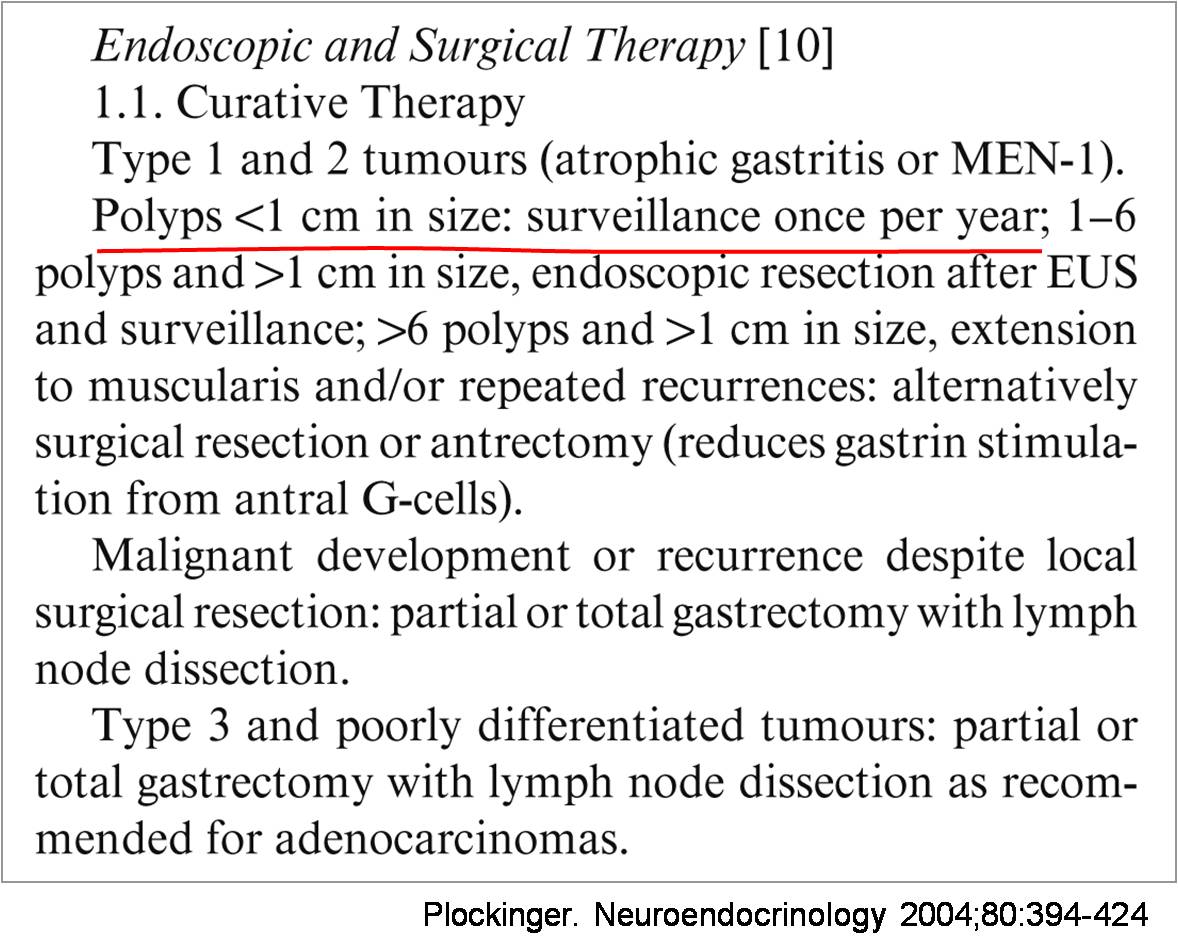
우리나라 영문 내시경학회지인 Clinical Endoscopy에서는 2013년 IDEN을 정리한 Special Issue를 냈습니다. 저는 고신대학교병원 박무인 교수님의 Endoscopic treatment for early foregut neuroendocrine tumors을 흥미롭게 읽었습니다. 여러분에게 소개하고 싶은 내용은 1 cm 이하의 type I NE tumor는 치료를 하지 않는다(surveillance only !)는 것입니다. 표를 보시면 surveillance를 하게 되어 있습니다 (빨간 별표). Type I은 atrophic gastritis (+) and/or hypergastrinemia인 형태입니다.
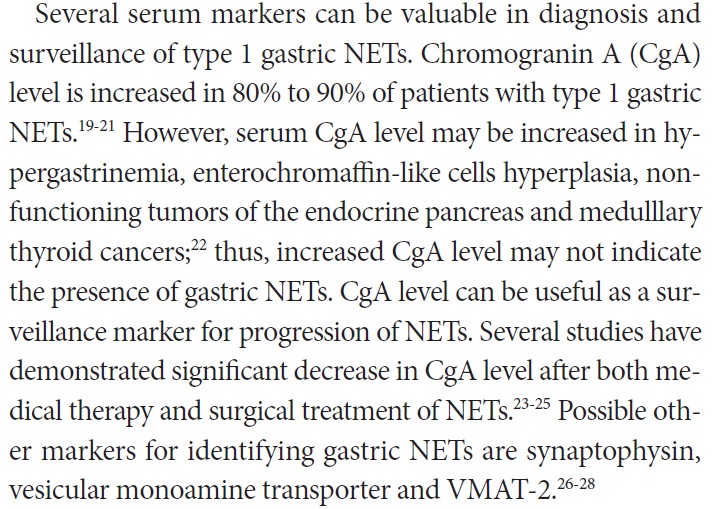
Serum marker의 역할은 아직 불명확합니다. 몇몇 연구는 있지만, 통상의 임상 protocol에는 들어가 있지 않습니다. 박무인 교수님 종설의 해당 내용입니다.
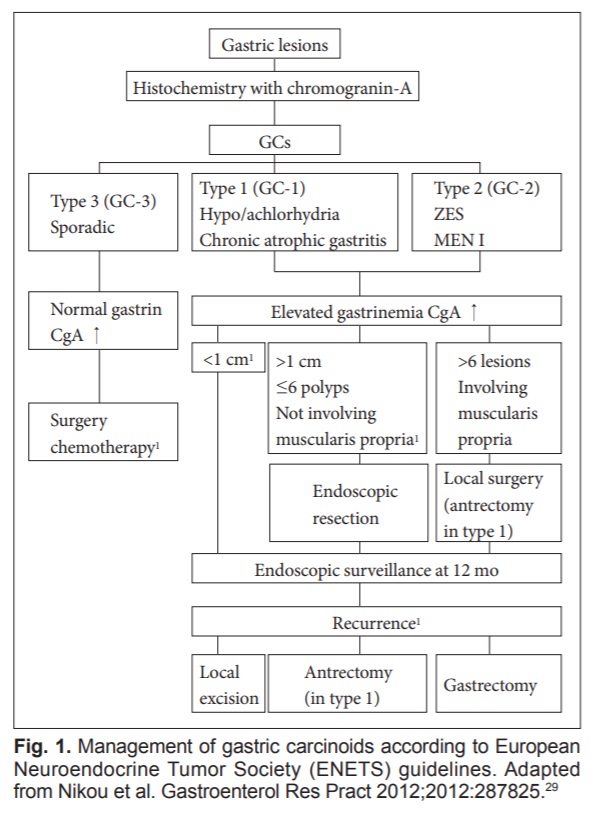
약간 오래된 자료이지만 Consensus statemenet on behalf of the European Neuroendocrine Tumore Society (ENETS) 에서도 비슷한 내용이 있습니다. 1 cm 이하의 type I NE tumor는 치료를 하지 않는다(surveillance only !)는 바로 그 내용입니다.
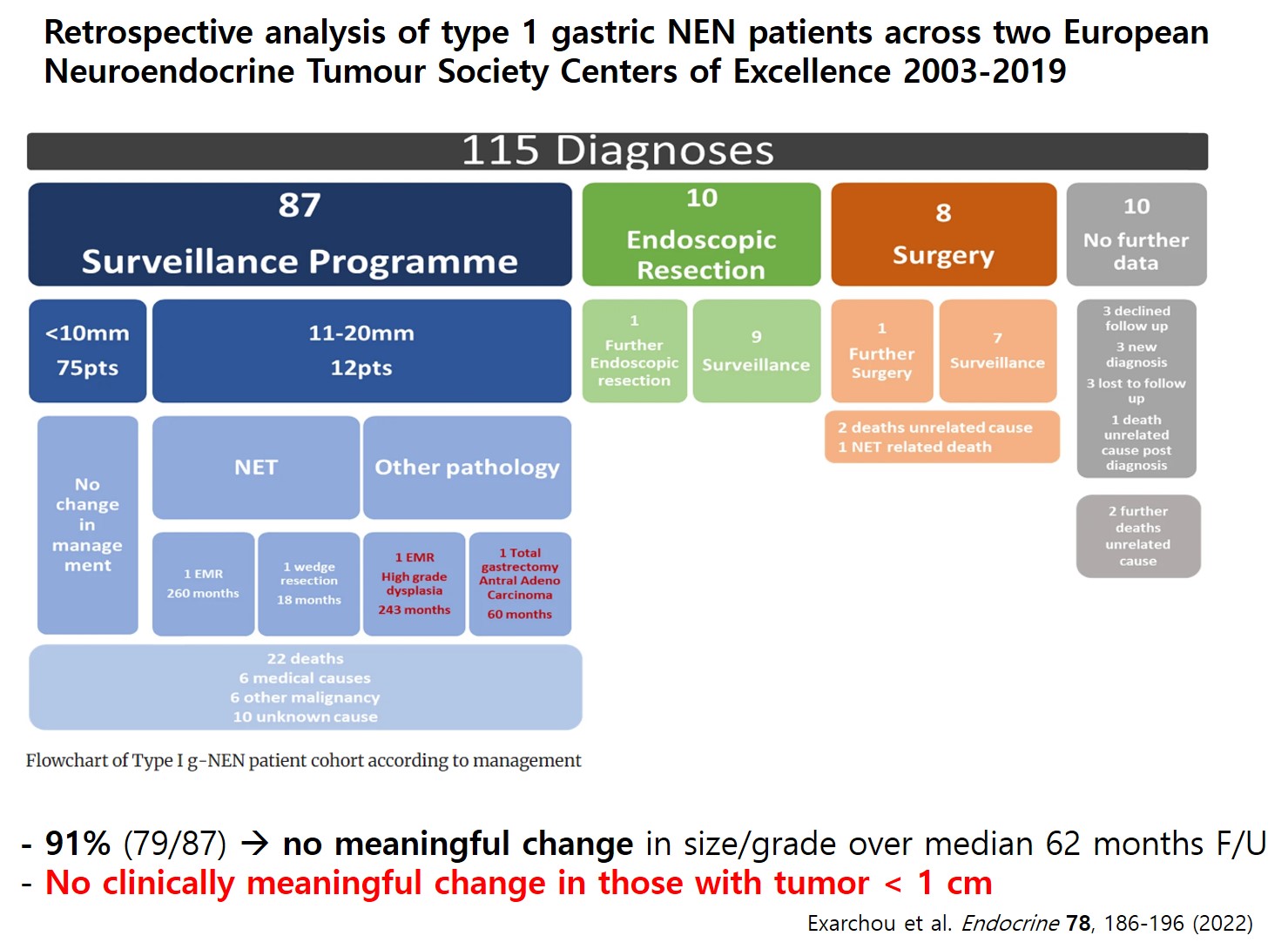
2024년 현재 가장 최근의 가장 큰 자료는 아래와 같습니다.
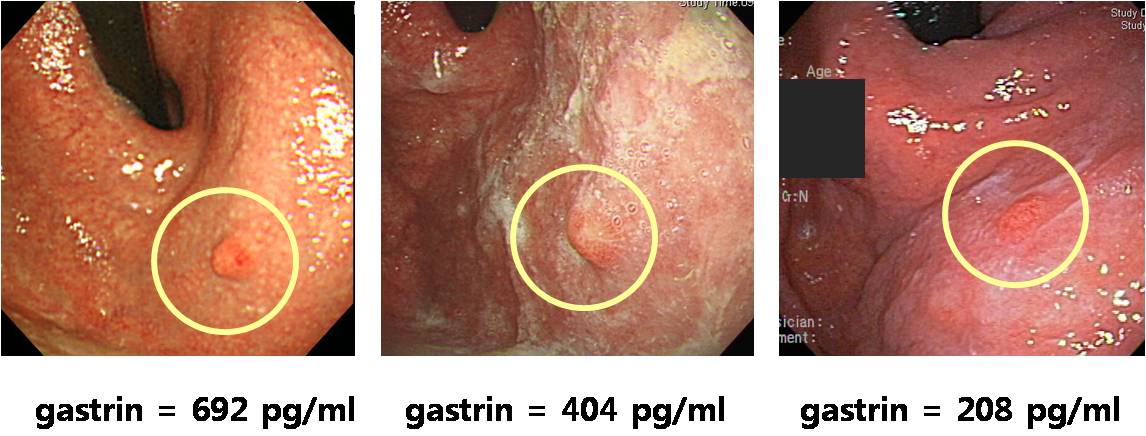
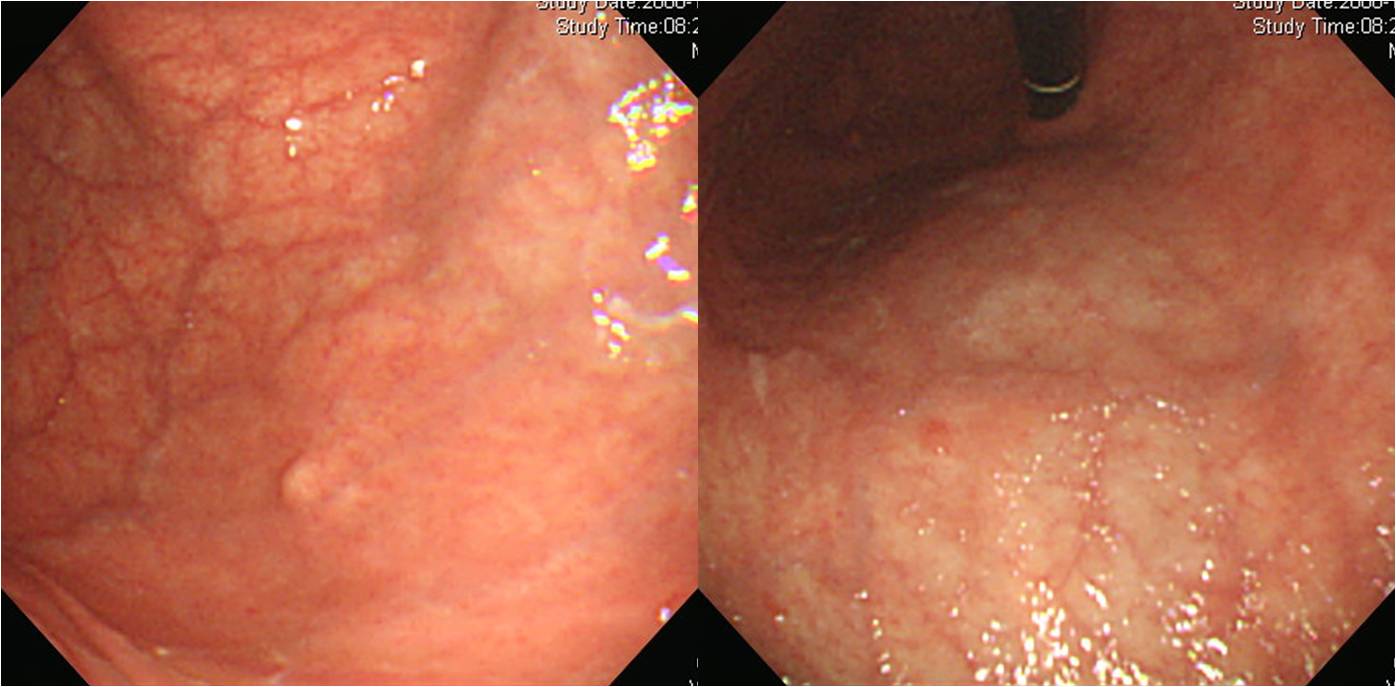
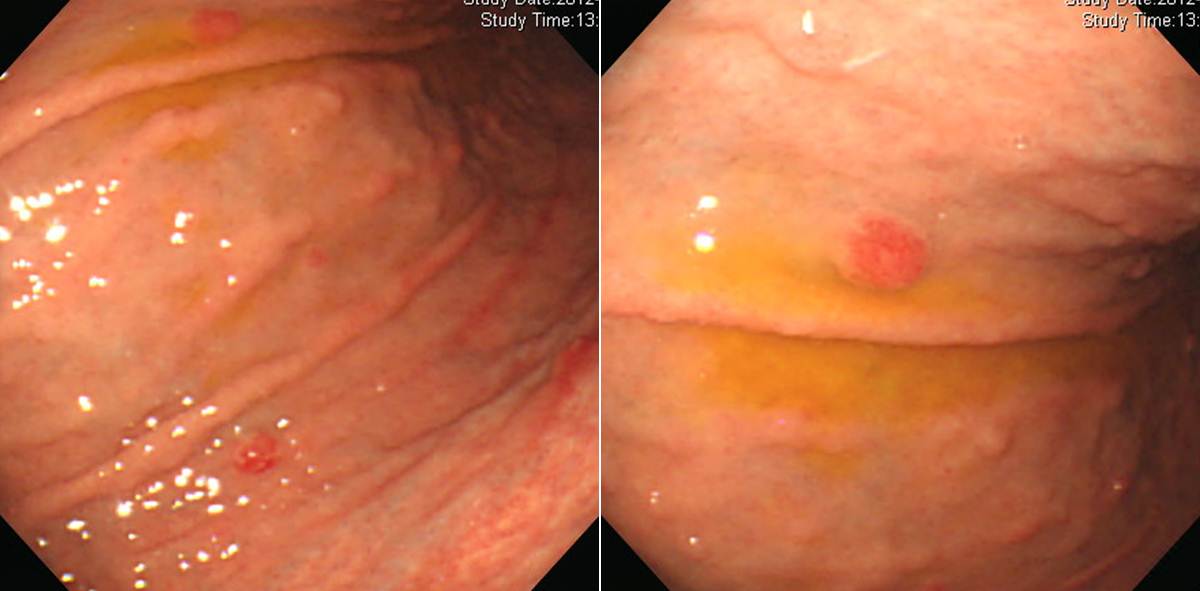
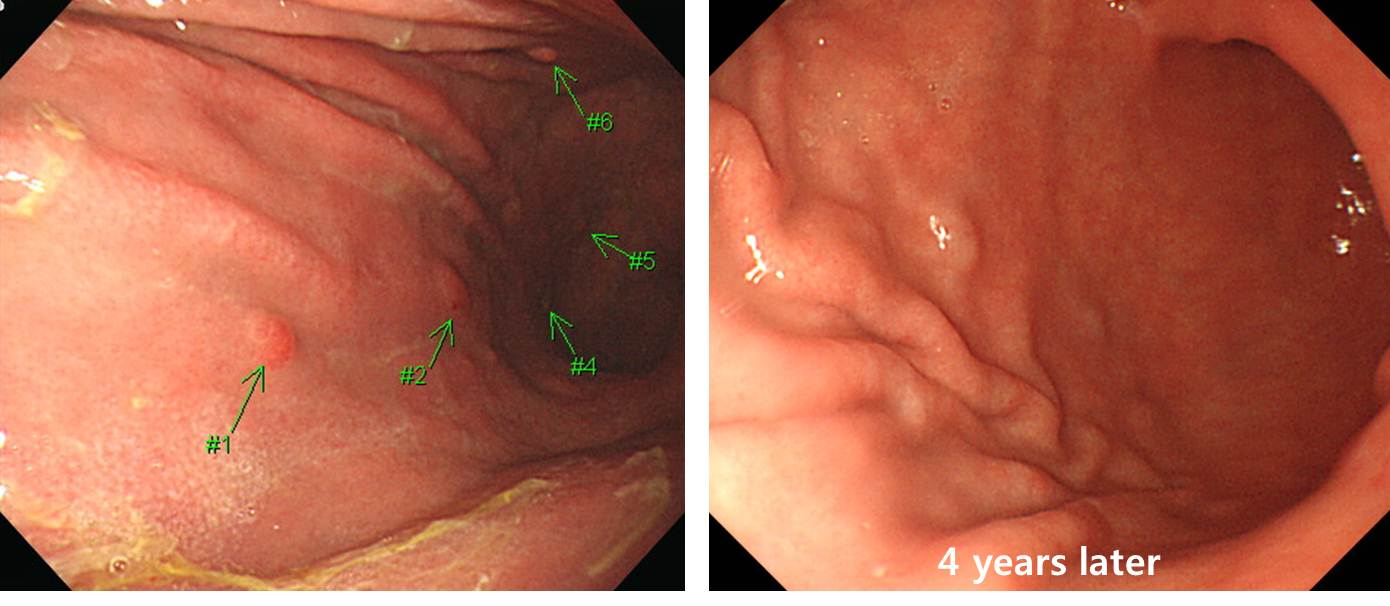
아래 예들은 모두 경과관찰이 가능하다고 생각합니다.
[More cases with observation]
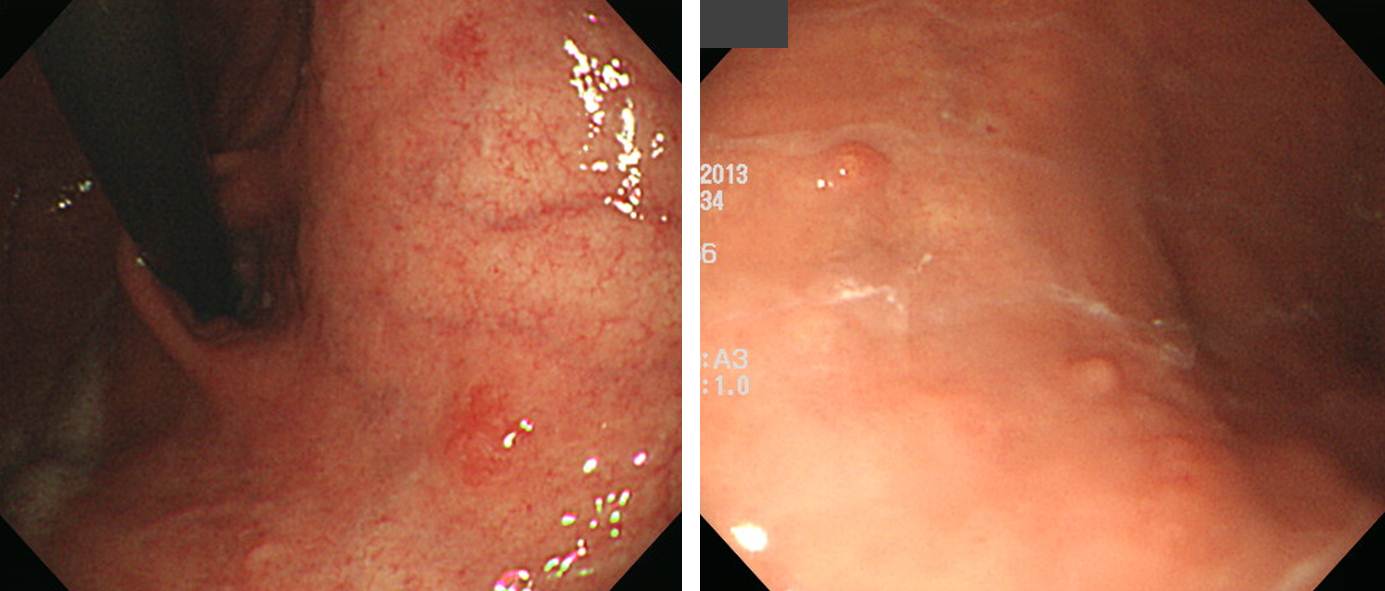
제 외래에는 수술적 혹은 내시경적 치료를 하지 않고 경과 관찰 중인 type I gastric carcinoid는 6-7명 정도 계십니다. (2015년 8월 현재)
1994년부터 경과관찰중인 multiple gastric carcinoids (gastrin = 386). 처음 total gastrectomy를 권유받고 오셨으나 10년 이상 아무 문제가 없음.
2번째 환자. Gastrin 119
3번째 환자. Gastrin 140
4번째 환자. Gastrin 404
5번째 환자. Gastrin 395
6번째 환자. Gastrin 530. 외국인
7번째 환자. Gastrin 410
![]() 4. Korean multicenter study
4. Korean multicenter study
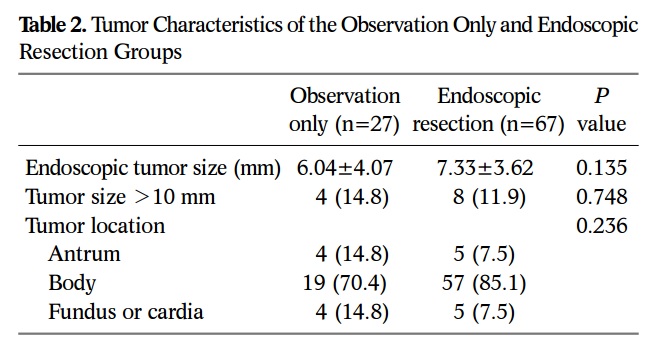
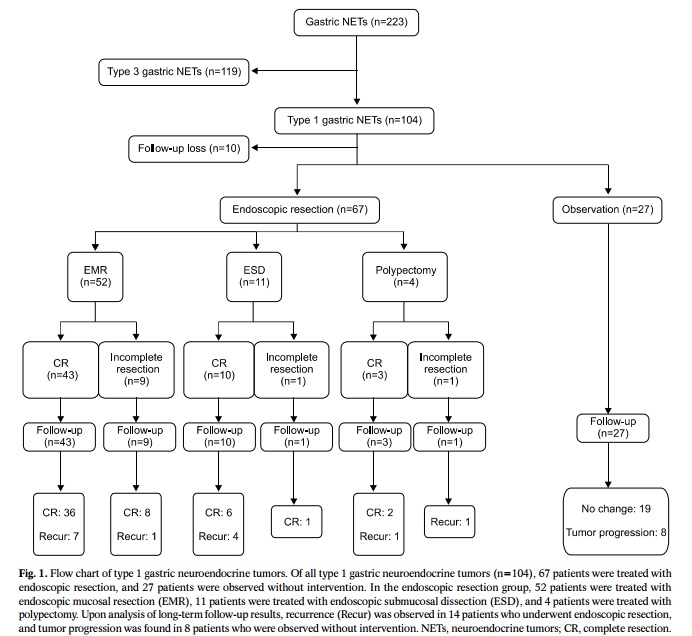
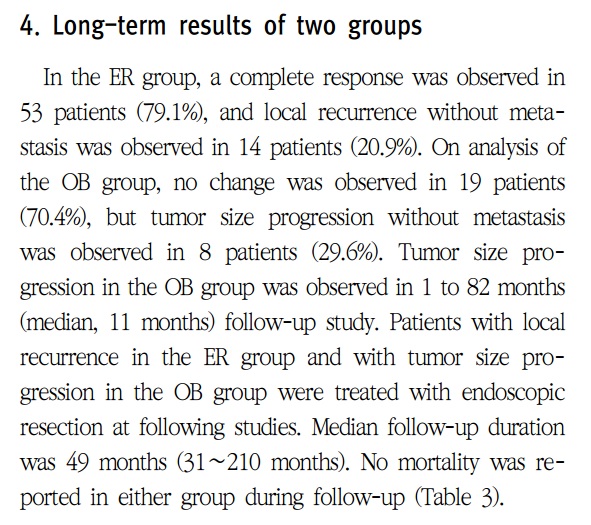
2016년 대한상부위장관헬리코박터학회지에 제1형 위유암종 치료성적에 대한 다기관 공동연구가 발표되었습니다 (Lee HS. KJHUGIR 2016).
위 신경내분비종양 223예 중 104예(46.6%)가 제1형이었으며, 94예의 추적관찰 결과가 분석되었습니다.67예는 내시경치료, 27예는 경과관찰되었습니다. 내시경치료군의 14예(20.9%)는 국소재발하여 내시경 치료가 추가되었고, 경과관찰군의 8예(29.6%)는 종양이 커져서 내시경치료가 필요했습니다. 모든 환자에서 원격 전이는 없었습니다.
![]() 5. [2017-3-25. KINGCA] Pathologic findings of gastric NET - 조미연
5. [2017-3-25. KINGCA] Pathologic findings of gastric NET - 조미연
Atrophic gastritis에 의한 ECL cell hyperplasia가 dysplasia로 되기 위해서는 몇 가지 추가적인 변화가 필요합니다.
Atrophic gastritis에 작은 neuroendocrine nodule을 만들었을 때에는 그 크기에 따라 hyperplasia와 dysplasia로 정의합니다.
Poorly-differentiated NEC와 NET G3는 비슷해 보일 수 있습니다.
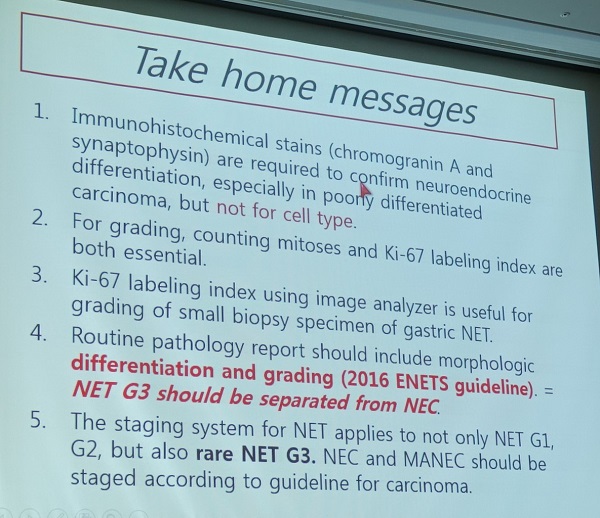
Differentiation (well differentiated vs. poorly differentiated)과 grading (G1, G2, G3)은 어떤 관계가 있을까요?
Ki-67과 mitosis는 어떤 상관관계가 있을까요? 둘 다 중요하다는 것이 일반적이지만, Ki-67 labeling index 검사법 자체에 상당한 limitation이 있습니다. 최근에는 digital image analyzer의 도움을 받으면 검사의 성적을 향상시킬 수 있다고 합니다. NET에서는 mitosis 측정이 매우 어렵습니다. 아주 짧은 시간에 cell cycle에서 escape를 할 수 있으므로 NET에서는 Ki-67이 중요합니다. 반면 GIST에서는 mitosis가 중요하고 Ki-67은 routine하게 측정하지는 않고 있습니다.
G3 NENs에는 NET G3 (세포형: well differentiated) 와 NEC (세포형: poorly differentiated)가 있습니다.
G3 NENs에는 속하는 NET G3와 NEC는 예후가 다르다는 매우 중요한 연구입니다.
2010년에는 G3를 carcinoma로 분류하였습니다. 그런데 well-differentiated NET 중 grade 3인 경우는 poorly differentiated와 확연히 다르다는 것이 알려졌습니다 (특히 췌장에서). 따라서 2017년에는 well differentiated G3를 NEC로 부르지 않고 NET G3로 부르도록 하고 있습니다.
![]() 6. 수술적 치료
6. 수술적 치료
첫 외부 내시경
조직검사. NET
의뢰 후 재검
기저질환이 있는지 혈액검사로 확인해 보았습니다.
수술은 wedge resection을 하였고 다행스럽게 G1으로 나왔습니다.

![]() 7. 내시경치료
7. 내시경치료

Stomach, endoscopic submucosal dissection:
Well-differentiated neuroendocrine tumor (G1)
1. Name of Procedure: ESD
2. Site of Tumor: Stomach (low body, greater curvature)
3. Diagnosis: Neuroendocrine tumor
4. WHO classification(2010): Neuroendocrine tumor(G1)
5. Multiplicity: Single
6. Size: 0.4x0.4 cm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic Count: 1/5 HPFs
Ki-67 labeling index: 2 %
9. Immunohistochemical Stains:
1) Synaptophysin : Positive
2) Chromogranin A: Positive
10. Lymphovascular invasion: Not identified
11. Perineural invasion: Not identified
12. Lymph node metastasis: not evaluated
13. Resection Margins: Negative
![]() 8. 조직검사 + 소작술로 치료한 유암종
8. 조직검사 + 소작술로 치료한 유암종
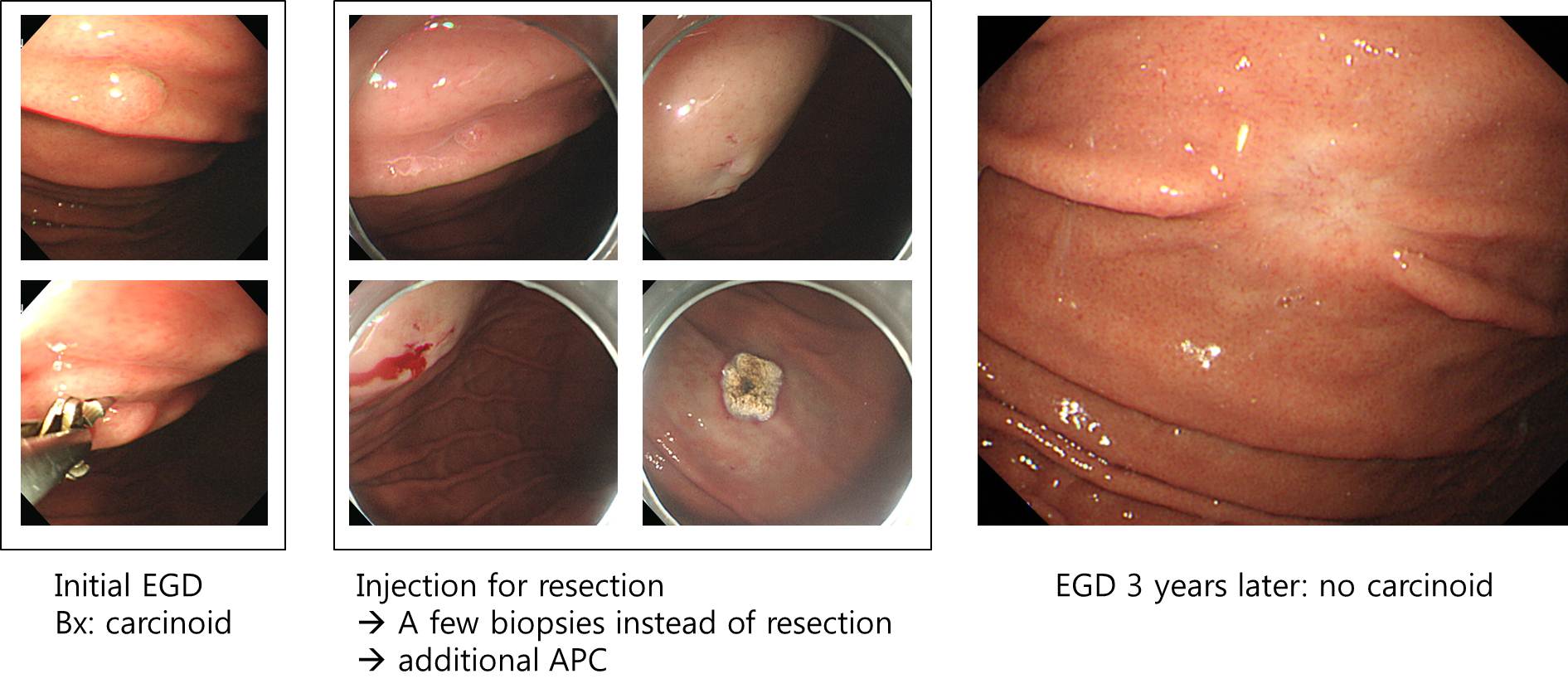
조직검사로 제법 조직을 제거할 수 있습니다. 소작술로 상당히 깊게 태워 없앨 수 있습니다. 절제술을 하려고 들어갔는데 막상 유암종이 너무 작아서 조직검사로 제거하였고 (이 또한 유암종으로 나왔음), 연이어 소작술을 하였습니다. 몇 년 뒤에 보았더니 깨끗한 반흔만 남아있었습니다.
![]() 9. Type III gastric carcinoid
9. Type III gastric carcinoid
제3형 유암종은 수술이 표준 치료입니다.
60세 여성 (2020). Gastrin 63.6 pg/ml
NET G1, 1.0cm, mucosa and submucosa, Ki 67 1%, mitotic count 1/10 HPF
Synaptophysin
Gastrin = 34.6 ng/ml로 수술 의뢰함
1. Name of Procedure: wedge resection
2. Site of Tumor: Stomach (high body and anterior wall)
3. Diagnosis: Neuroendocrine tumor, G2
4. WHO classification(2010): Neuroendocrine tumor(G2)
5. Multiplicity: Single
6. Size: 1.2x1.1 cm
7. Extent: Submucosa
8. Grading: Mitotic Count: 2-20 (2/10 HPF), Ki-67 labeling index: G2 3-20%
9. Immunohistochemical Stains: Synaptophysin : Positive, Chromogranin A: Positive, weak
10. Lymphovascular invasion: Not identified
11. Perineural invasion: Not identified
12. Resection Margins: Negative (Safety margin : 0.5 cm)
13. CEA: Negative
14. D2-40: Revealed no endolymphatic emboli
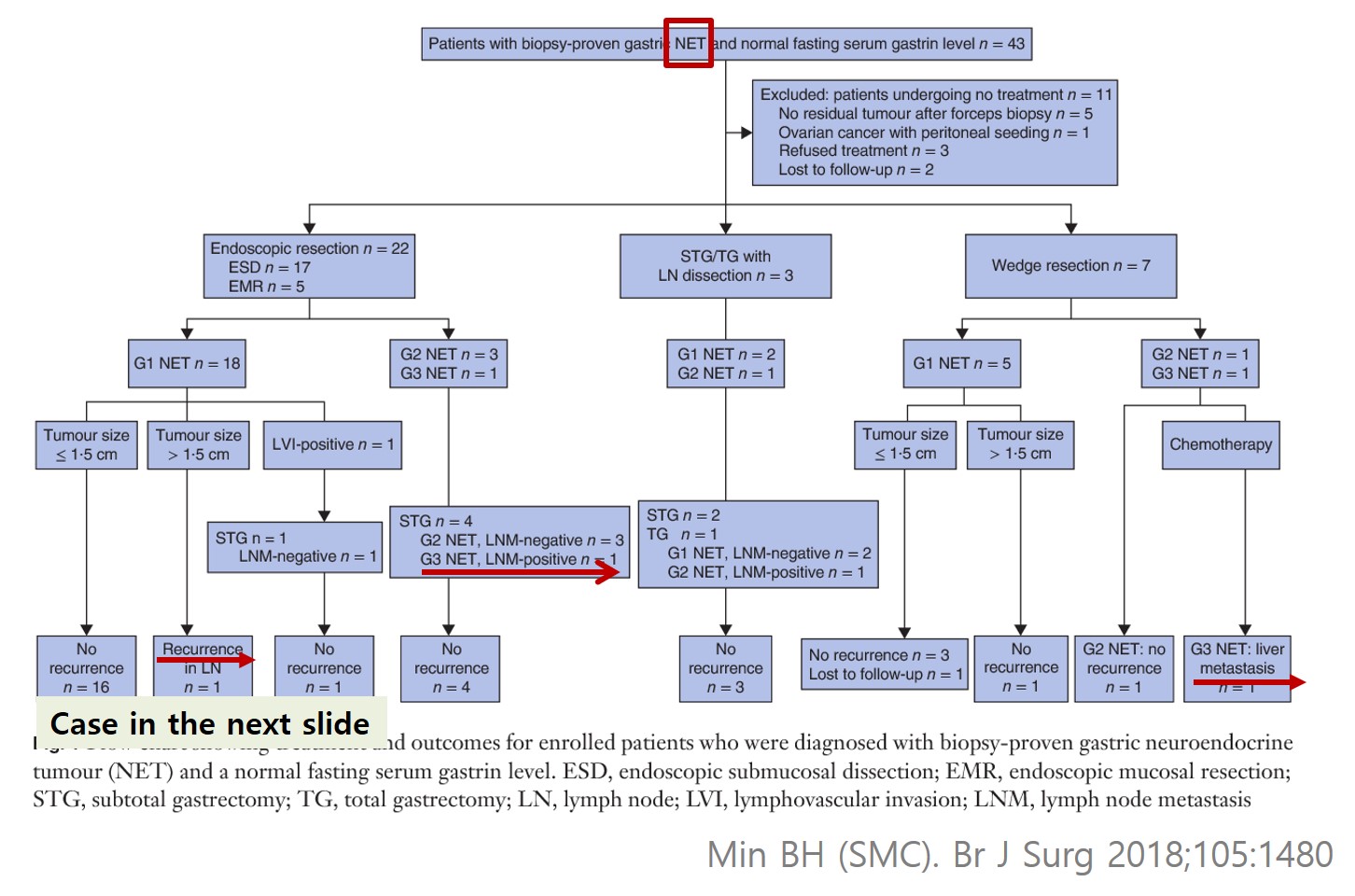
최근에는 무증상 성인에서 발견되는 작은 제3형 신경내분비종양을 내시경으로 치료하려는 시도가 있습니다 (Min BH. Br J Surg 2018). 그러나 내시경 치료의 적응증 선택에 상당히 주의해야 합니다.
50대 여성. Gastrin 23.5, 수술 권유하였으나 내시경치료 원하여 ESD. 5년 후 perigastric node metastasis로 다시 수술 권유
Stomach, high body, posterior, endoscopic submucosal dissection:
WELL DIFFERENTIATED ENDOCRINE TUMOR (CARCINOID TUMOR):
1) size: 1.6x1.5 cm
2) confined to mucosa/submucosa
3) lymphovascular invasion: not identified
4) mitosis: 0/10 HPFs
5) negative resection margins
Chromogranin : Strong positive
Synaptophysin: Positive
Ki-67 : Positive in less than 1% of tumor cells
Serum gastrin 41.9
Stomach, laparoscopic wedge resection: Well differentiated neuroendocrine tumor (CARCINOID) (G1)
1. Name of Procedure: laparoscopic wedge resection
2. Site of Tumor: Stomach (high body, greater curvature)
3. Diagnosis: Neuroendocrine tumor
4. WHO classification(2010): Well-differentiated Neuroendocrine tumor (G1)
5. Multiplicity: Single
6. Size: 1.7x1.5 cm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic Count(/10HPF): 0-1, Ki-67 labeling index: G1: <3%
9. Immunohistochemical Stains:
1) Synaptophysin : Positive
2) Chromogranin A: Positive
10. Lymphovascular invasion: Not identified
11. Perineural invasion: Not identified
12. Lymph node metastasis: not evaluated
13. Resection Margins: Negative, Safety margin : 1.5 cm
50대 남성입니다. ESD 후 lymphatic invasion 소견이 있어 G2였지만 수술을 권했습니다. 다행스럽게 residual tumor는 없었습니다. 림프절 전이도 없었습니다.
Stomach, endoscopic submucosal dissection:
Well-differentiated neuroendocrine tumor (G2)
1. Name of Procedure: ESD
2. Site of Tumor: Stomach (mid body, anterior wall-lesser curvature)
3. Diagnosis: Neuroendocrine tumor
4. WHO classification(2010): Neuroendocrine tumor(G2)
5. Multiplicity: Single
6. Size: 9x8 mm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic Count: 0-1/10HPF, Ki-67 labeling index: G2: about up to 3%
9. Lymphovascular invasion: Present
10. Perineural invasion: Not identified
11. Resection Margins: Negative, Safety margin: distal, 5 mm; proximal, 9 mm; anterior, 12 mm; posterior, 14 mm; deep, less than 100 ㎛
위신경내분비종양의 스펙트럼은 매우 다양합니다. Hypergastrinemia를 동반한 작은 type I은 경과관찰만 합니다. 그러나 metastasis를 보이는 심한 경우도 있습니다. 그 경계는 상당히 애매합니다.
조직검사에서 neuroendocrine carcinoma가 나와 의뢰되었습니다. Serum gastrin은 65.8 pg/ml로 정상이었습니다. 내시경 재검을 하였는데 놀랍게도 "tumor emboli of neuroendocrine tumor"라고 나왔습니다. 수술을 시행하였고 또 다시 놀랍게도 림프절 전이가 있었습니다. Tumor의 grade는 G2였습니다.
Well-differentiated neuroendocrine carcinoma (G2)
1. Name of Procedure: Subtotal gastrectomy
2. Site of Tumor: Stomach (body)
3. Diagnosis: Neuroendocrine tumor
4. WHO classification(2010): Neuroendocrine tumor (G2)
5. Multiplicity: Single
6. Size: 1.4x1.0 cm
7. Extent: Mucosa and submucosa
8. Graging: Mitotic count: 2-20/10 HPF, Ki-67 labeling index: G2 3-20%
9. Immunohistochemical Stains:
- Synaptophysin: Positive
- Chromogranin A: Positive
10. Lymphovascular invasion: Present
11. Perineural invasion: Not identified
12. Lymph node metastasis : metastasis to 1 out of 44 regional lymph nodes (pN1) (perinodal extension: absent) (1/44: LN3,5, 1/13; LN4,6, 0/9; "1", 0/0; "4sb", 0/1; "5", 0/1; "6", 0/5; "8a", 0/2; "7", 0/4; "9", 0/3; "11p", 0/4; "12a", 0/2)
13. Resection Margins: Negative, Safety margin : 1.5 cm(proximal), 14.5 cm(distal)
Subtotal gastrectomy with D2 lymph node dissection을 하지 않았으면 어떠한 결과가 나왔을까 생각해 보았습니다. 사실 hypergastrinemia를 동반한 작은 G1 NET는 내시경 치료나 수술을 하더라도 wedge resection을 하고 마는 경우가 많기 때문입니다.
요컨데 G2는 매우 주의해야 합니다. Serum gastrin이 정상일 때에는 더욱 그렇습니다. 문제는 forcep biopsy에서 grade를 나누기 어려운 경우가 많다는 점인데요...... 고민은 계속되는데 답은 없고...... 잠이 오질 않습니다. 환자 걱정에.
![]() 10. Gastric neuroendocrine carcinoma
10. Gastric neuroendocrine carcinoma
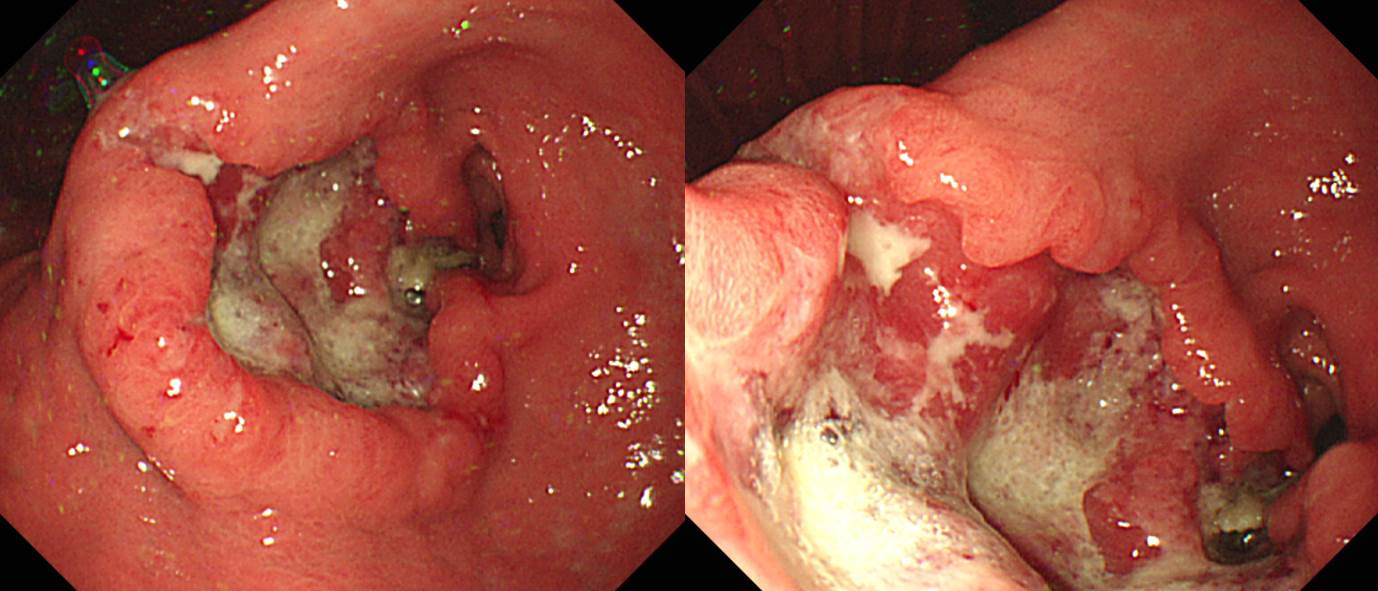
Regular endoscopic followup was done after endoscopic resection of early gastric cancer arising from adenoma. He suddenly developed upper abdominal discomfort. Endoscopy showed a large ulcerative lesion in the antrum, and the pathology was neuroendocrine carcinoma. There were multiple metastases in the liver. Previous endoscopic images (8 months ago) were reviewed, but there was no evidence of gastric cancer recurrence or neuroendocrine neoplasms. Only subtle erosions were suspicious. (위암 663)
NEUROENDOCRINE CARCINOMA, POORLY DIFFERENTIATED (grade 3)
. Mitosis: 12 / 10 HPF
. Synaptophysin: Positive in some tumor cells
. Chromogranin: Negative
. CD56: Diffuse strong positive
. Ki-67: Positive in about 30% of tumor cells
Poorly-differentiated neuroendocrine carcinoma (G3)
1. Name of Procedure: Organ resection+Node dissection (specify: subtotal gastrectomy)
2. Site of Tumor: Stomach (Antrum and pylorus)
3. Diagnosis: Neuroendocrine carcinoma
4. WHO classification(2010): Neuroendocrine carcinoma
5. Multiplicity: Single
6. Size: 2.5x1.8 cm
7. Extent: Mucosa and submucosa (pT1b)
8. Grading: Mitotic Count: >20/10HPF, Ki-67 labeling index: G3>20%
9. Immunohistochemical Stains: 1. Synaptophysin : Positive 2. Chromogranin A: Positive OPTIONAL : CD56 (+)
10. Lymphovascular invasion: Present (intra- and extramural)
11. Perineural invasion: Present
12. Lymph node metastasis: metastasis to 6 out of 71 regional lymph nodes (pN2) (perinodal extension: absent) (6/71: "1", 0/9; "3", 4/19; "4", 1/3; "4sb", 0/5; "5", 0/0; "6", 0/5; "7", 0/6; "8a", 1/3; "9", 0/8; "11p", 0/9; "12a", 0/3; "11d", 0/1)
13. Resection Margins: Negative Safety margin : proximal, 4 cm; distal, 2.8 cm
14. AJCC stage by 7th edition: pT1b N2
Stomach, subtotal gastrectomy:
Poorly-differentiated neuroendocrine carcinoma (G3)
1. Name of Procedure: Organ resection
2. Site of Tumor: Stomach (Antrum)
3. Diagnosis: Neuroendocrine carcinoma (G3)
4. WHO classification(2010): Poorly differentiated neuroendocrine carcinoma, large cell type
5. Multiplicity: Single
6. Size: 6x6 cm
7. Extent: Serosa
8. Grading: Mitotic Count(/10HPF): >20 (about 60/10 HPF)
9. Immunohistochemical Stains: Synaptophysin : Positive, Chromogranin A: Negative, CD56 (+)
10. Lymphovascular invasion: present
11. Perineural invasion: present
12. Lymph node metastasis: [Number of positive nodes/Total number of nodes(7/32)]
13. Resection Margins: Negative
14. Other Pathologic Components: Presence of tumor necrosis (60 %)
melena로 내원하여 수술을 의뢰하였습니다.
1. WHO classification(2010): Neuroendocrine carcinoma (G3)
2. Size: 7.5x4.5x4 cm
3. Grading: Mitotic Count: >20/10HPF, Ki-67 labeling index: G3>20%
4. Immunohistochemical Stains: Synaptophysin : Positive; Chromogranin A: Positive; CD56 (-)
5. Lymphovascular invasion: Present
6. Perineural invasion: Not identified
7. Resection margins: Negative
8. Other pathologic components: presence of tumor necrosis (20 %)
위암 698
Subtotal gastrectomy: Neuroendocrine carcinoma (G3)
1. Name of Procedure: Radical subtotal gastrectomy
2. Site of Tumor: Stomach (distal antrum and posterior wall)
3. Diagnosis: Neuroendocrine tumor
4. WHO classification(2010): Poorly differentiated Neuroendocrine carcinoma (G3)
5. Multiplicity: Single
6. Size: 1.9x0.5 cm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic Count(/10HPF): >20, Ki-67 labeling index: G3>20%
9. Immunohistochemical Stains: Synaptophysin : Positive
10. Lymphovascular invasion: Not identified
11. Perineural invasion: Not identified
12. Lymph node metastasis: 0/20: "3", 0/7; "4", 0/4; "5", 0/0; "6", 0/3; "7", 0/0; "9", 0/0; "8a", 0/5; "11p", 0/1; "12a", 0/1; "4sb", 0/0; "1", 0/6)
13. Resection Margins: Negative: Safety margin : 2 cm
14. AJCC stage by 8th edition: pT1 N0
MUO로 내원하신 분으로 전정부 병소 위내시경 조직검사와 transabdominal biopsy 모두 neuroendocrine carcinoma로 확인되었음 (2018)
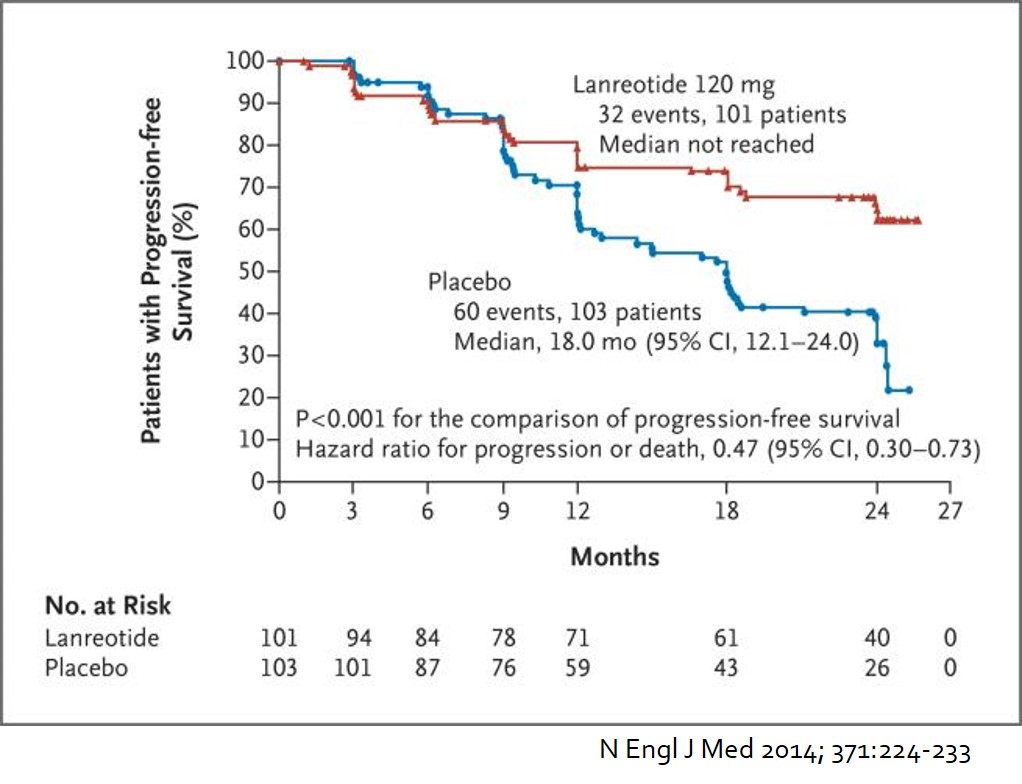
![]() 11. Lanreotide for metastatic neuroendocrine tumor
11. Lanreotide for metastatic neuroendocrine tumor
![]() [FAQ]
[FAQ]
[2016-9-6. 애독자 질문]
매일 교수님의 가르침 잘 받고 있습니다. 항상 감사드립니다.
진료 중 궁금한 것이 있어 질문드립니다. 간헐적인 속쓰림 환자로 내시경상 5mm 정도의 gastric neuroendocrine tumor 로 확인되어 경과관찰하려고 하였으나 증상이 심해 EMR 시행하였습니다. Resection margin negative 로 확인되어 경과관찰 중 간헐적인 속쓰림있고 내시경상 이상 소견 보이지 않으나 gastrin level이 1000으로 매우 높게 확인되었는데, 다른 부위에 대한 evaluation을 시행해야될지 PPI 쓰면서 경과 관찰해야될지 교수님의 고견부탁드립니다.
[2016-9-6. 이준행 답변]
경과관찰을 고려하였다는 점으로 보아 유암종에 대한 EMR 전부터 gastrin이 높았을 것 같군요. 유암종 치료 전 CT 등을 하셨을 것이구요.
CT에서 췌장이나 십이지장에 종양이 없고 (= gastrinoma가 아니고), gastrin치가 높으면서 위유암종이 있는 경우는 제1형 유암종이기 때문에 크기가 작으면 경과관찰을 할 수 있습니다. 증상이 있어서 치료하셨다고 하셨지만 사실 작은 제1형 유암종과 증상은 아무 관계가 없습니다.
우연히 발견된 고가스트린 혈증의 가장 흔한 원인은 atrophic gastritis입니다. PPI 사용이 두번째 원인입니다. 따라서 CT에서 이상이 없었다면 아무 것도 하지 않아도 무방할 것 같습니다. 환자에게는 향후 유암종이 또 발생할 수 있지만, 그렇다고 꼭 치료가 필요한 것도 아니다고 잘 설명하시면 되겠습니다.
[2026-5-7] 조선일보 신경내분비종양, 관리 가능한 암… 완치 강박 버리고 '건강한 共存' 모색해야
![]() [References]
[References]
1) The pathologic classification of neuroendocrine tumors (PDF) Nature Guidelines (2010)
2) Carcinoid tumor (PDF) 대한 Helicobacter 및 상부위장관 연구학회 춘계심포지엄 (이준행. 2009)
3) EndoTODAY Gastric carcinoid 위유암종
4) EndoTODAY Duodenal carcinoid 십이지장 유암종
5) EndoTODAY Colorectal neuroendocrine tumor 결장직장 신경내분비종양. 직장 유암종.
6) EndoTODAY Case: rectal carcinoid with metastasis 직장 유암종 림프절 전이 증례
7) 자가면역성 만성 위축성 위염과 연관하여 발생한 위 신경내분비종양 Neuroendocrine tumoe associated with autoimmune gastritis
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.