Previous | Home | EndoTODAY | List | Next
![]() [Inserting endoscope (4). 내시경 삽입법]
[Inserting endoscope (4). 내시경 삽입법]
![]() 9. 환자에게 침을 삼키라고 요구하지 않는다.
9. 환자에게 침을 삼키라고 요구하지 않는다.
과거에는 환자에게 침을 삼키라고 요구하는 경우가 많았습니다. 그러나 환자가 침을 삼키는 등의 행동을 하면 오히려 upper esophageal sphincter가 조여지는 순간이 발생합니다. 내시경 의사와 환자가 정확하게 박자가 맞지 않으면 삽입이 힘들어집니다. 최근에는 환자에게 침을 삼키라고 요구하지 않는 경우가 대부분입니다. 여러번 시도하였으나 잘 되지 않을 때에 한하여 침을 삼키도록 요구하는 것이 좋습니다.
![]() 10. 환자와 적절한 거리를 유지한다.
10. 환자와 적절한 거리를 유지한다.
환자에 너무 접근하면 삽입부가 휘어지면서 내시경의 조작성이 떨어집니다 (아래 그림 참조). 적당하게 떨어져서 내시경이 항상 크고 부드러운 곡선을 유지하도록 해야 합니다.

그림설명: 환자와 거리가 너무 가까워 내시경 삽입부가 휜 모습. 한 발짝 뒤로 물러서야 합니다.
![]() 11. 선 자세로 검사한다.
11. 선 자세로 검사한다.
간혹 앉은 자세로 위내시경을 하는 매우 매우 나쁜 습관을 가진 분이 계십니다. (1) 삽입할 때 내시경을 섬세하게 조절할 수 없습니다. (2) 환자와 적절한 거리를 유지하기 어렵습니다. (3) 조작성이 떨어지므로 손가락, 허리, 어깨를 많이 써야 합니다. 의사 자신의 ergonomic problem이 발생합니다. 반드시 선 자세로 검사합시다.

![]() [2013 Yonsei Gastric Cancer Symposium]
[2013 Yonsei Gastric Cancer Symposium]
어제 2013년 9월 28일 연세대학교 2013 위암 심포지엄이 열렸습니다.


![]() 1. Diagnosis for major surgical complications - 연세대학교 영상의학과 임준석
1. Diagnosis for major surgical complications - 연세대학교 영상의학과 임준석
위암 수술 후 postoperatve leakage 진단에 oral contrast를 사용한 CT가 큰 도움이 됩니다 (아래 연세대학교 연구 결과 참조).
Clinical implication of positive oral contrast computed tomography for the evaluation of postoperative leakage after gastrectomy for gastric cancer JCAT 2010:34(4):537. There were 162 patients without extraluminal contrast leakage (77.1%), 13 with grade 1 leakage (6.2%), 19 with grade 2 (9.0%), and 16 with grade 3 (7.6%). Postoperative intervention rate, hospital stay, and mortality were significantly higher in patients with extraluminal contrast than those in patients without extraluminal contrast (P < 0.05). Postoperative hospital stays increased as the leakage grades increased (P = 0.0008). The matching accuracy between CT and other studies was 82.1% (n = 32/39).
출혈이 CT angiography에서 보이지 않으면 catheter angiography에서도 보이지 않는다고 합니다. CT angiography는 0.3-0.5ml/min의 민감도를 가지고 있기 때문에 catheter angiography의 0.5ml/min와 비슷하거나 우월합니다. 간혹 출혈이 의심되는 상황에서 oral contrast CT가 처방되는 경우가 있는데 이는 반드시 피해야 합니다.
![]() 2. Endoscopic treatment - 연세대학교 내과 이상길
2. Endoscopic treatment - 연세대학교 내과 이상길

수술 후 출혈에 대한 내시경치료와 관련된 연구결과는 매우 적습니다. 동아대학교의 자료입니다.
Endoscopic treatment and risk factors of postoperative anastomotic bleeding after gastrectomy for gastric cancer. Of 2031 patients with gastric cancer who underwent radical gastrectomy (R0 resection) between January 2002 and December 2010, postoperative anastomotic bleeding was observed in 7 patients...... The bleeding sites were as follows: Billroth-I anastomosis using a circular stapler (n = 1), Billroth-II anastomosis by manual suture (n = 5), and esophagojejunostomy using a circular stapler (n = 1). All patients were treated with endoscopic clipping or epinephrine injection. There was no further endoscopic intervention or reoperation for anastomotic bleeding.
Leakage에 대한 연세대학교 병원의 결과입니다. 2 cm 이상이면 내시경치료가 어렵습니다.
Endoscopic management of anastomotic leakage after gastrectomy for gastric cancer: how efficacious is it? The authors retrospectively reviewed 33 patients with anastomotic leakage who had underdone endoscopic treatment among 5249 patients with gastric cancer who underwent radical total or subtotal gastrectomy. The size of the tissue defect was the only factor that had statistically significant differences among the cases with complete closure, partial closure and failure (p = 0.005). For tissue defects smaller than 2 cm in size, complete closure was achieved in 19 (73.1%), partial closure in 5 patients (19.2%) and 2 failed (7.6%). For those larger than 2 cm in size, one (14.3%) was completely closed, four (57.1%) were partially closed and two (28.6%) failed.
최근에는 leakage에 대하여 기존의 내시경치료뿐만 아니라 stent를 많이 이용하고 있습니다. 그리고 over-the-scope clip (OTSC)이 시도되고 있습니다. 아래는 독일의 결과입니다.
The Over-The-Scope Clip (OTSC) for the treatment of gastrointestinal bleeding, perforations, and fistulas. Since April 2006, 50 patients have been treated for different indications with the OTSC clip in our department. Besides hemostasis (n = 27) in the colon and the upper GI tract, the clip has been used for closure of esophageal and gastric perforations and adaptation of covered and free perforations after colonoscopy (n = 11). Furthermore, the OTSC has been used to close fistulas (n = 8) and for preoperative marking (n = 4). The primary treatment was successful in all cases. There were two secondary bleedings that required endoscopic interventions. Closure of iatrogenic perforations of the upper and lower GI tract was successful in all cases. A permanent closure of fistulas could not be achieved in all cases with the OTSC clip.
이용찬 좌장님 comment: 연세대학교에서는 endoscopic vacuum-assisted closure를 3예 정도 적용한 경험이 있습니다. 주로 식도에서 사용하는 방법이지만 위암 수술 후에도 사용할 수 있습니다. 아래는 독일의 결과입니다.
Endoscopic closure of esophageal intrathoracic leaks: stent versus endoscopic vacuum-assisted closure, a retrospective analysis. In a retrospective analysis we were able to identify 39 patients who were treated with SEMS or SEPS and 32 patients who were treated with EVAC for intrathoracic leakage. In addition to successful fistula closure, we analyzed hospital mortality, number of endoscopic interventions, incidence of stenoses, and duration of hospitalization. In a multivariate analysis, successful wound closure was independently associated with EVAC therapy (hazard ratio 2.997, 95 % confidence interval [95 %CI] 1.568 - 5.729; P = 0.001). The overall closure rate was significantly higher in the EVAC group (84.4 %) compared with the SEMS/SEPS group (53.8 %). No difference was found for hospitalization and hospital mortality. We found significantly more strictures in the stent group (28.2 % vs. 9.4 % with EVAC, P < 0,05).
![]() 3. Radiologic treatment - 가톨릭대학교 영상의학과 이해규
3. Radiologic treatment - 가톨릭대학교 영상의학과 이해규
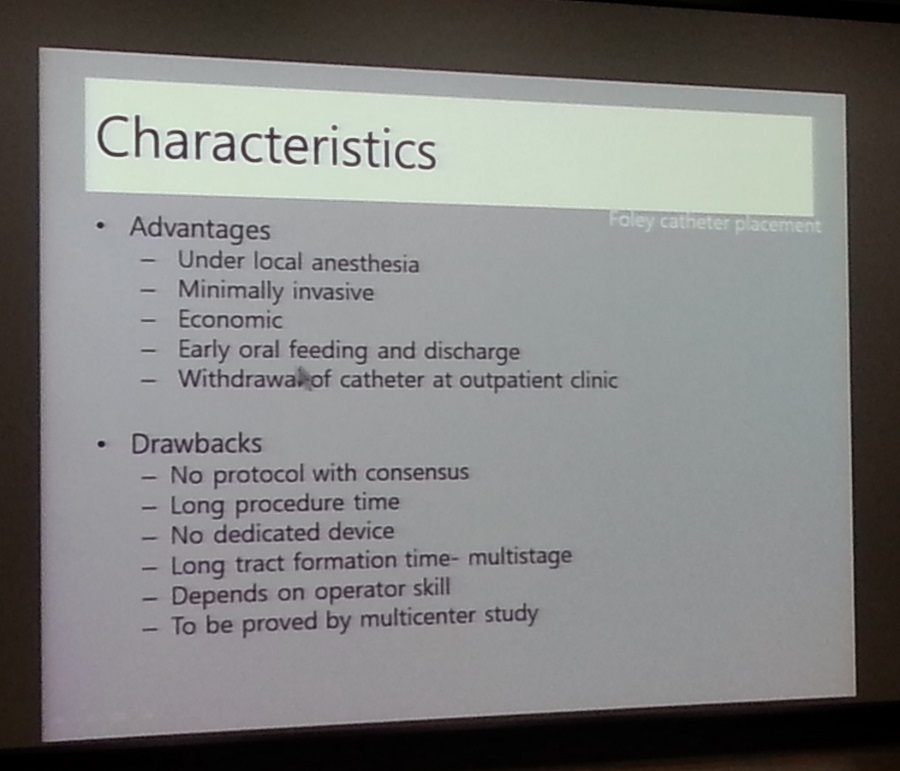
Duodenal stump leakage에서 Foley catheter를 이용한 drainage가 유용합니다.
Percutaneous management of postoperative duodenal stump leakage with foley catheter. Ten consecutive patients (M:F = 9:1, median age: 64 years) were included in this retrospective study. The duodenal stump leakages were diagnosed in all the patients within a median of 10 days (range, 6-20). At first, the patients underwent percutaneous drainage on the day of or the day after confirmation of the presence of duodenal stump leakage, and then the Foley catheters were replaced at a median of 9 days (range, 6-38) after the percutaneous drainage. Foley catheters were placed successfully in the duodenal lumen of all the patients under a fluoroscopic guide. No complication was observed during and after the procedures in all the patients. All of the patients started a regular diet 1 day after the Foley catheter placement. The patients were discharged at a median of 7 days (range, 5-14) after the Foley catheter placement. The catheters were removed in an outpatient clinic 10-58 days (median, 28) after the Foley catheter placement.
상부위장관 transarterial catheter embolization에서는 collateral이 많기 때문에 ischemic damage를 크게 걱정하지 않습니다. 그러나 Whipple 수술 등 큰 수술 후에는 collateral이 거의 없기 때문에 ischemic damage 가능성을 고려해야 합니다.
첫 연자께서 "출혈이 CT angiography에서 보이지 않으면 catheter angiography에서도 보이지 않는다"고 하셨지만 postsurgical bleeding 상황에서는 약간 다르다고 생각합니다. Pseudoaneurysm이 많기 때문입니다. Pseudoanuerysm은 아무리 작아도 치료를 하는 것이 원칙입니다. Pseudoaneurysm을 막을 때에는 colleteral이 많기 때문에 한 곳만 막으면 재출혈이 많습니다. Isolation technique (front door와 back door를 모두 막는 것)이 중요합니다. 최근에는 blood flow를 유지시키기 위하여 stent graft를 사용하기도 합니다.
![]() 위암 심포지엄이 열린 연세대학교 병원 로비에서 우연히 오래된 카메라들이 전시된 것을 보았습니다. 여러 교수님들과 환자들이 기증한 것이었습니다. 대한기능성질환운동학회 전 회장님이신 박효진 선생님께서 기증한 Pentax 카메라도 있었습니다. 박효진 교수님. 존경합니다.
위암 심포지엄이 열린 연세대학교 병원 로비에서 우연히 오래된 카메라들이 전시된 것을 보았습니다. 여러 교수님들과 환자들이 기증한 것이었습니다. 대한기능성질환운동학회 전 회장님이신 박효진 선생님께서 기증한 Pentax 카메라도 있었습니다. 박효진 교수님. 존경합니다.

서민 교수님의 '기생충열전'을 읽고 있습니다. 문득 EndoTODAY에서 소개드렸던 기생충에 대한 정보를 모아보자는 생각이 들었습니다.
![]() [EndoTODAY Parasitology. 엔도투데이 기생충학]
[EndoTODAY Parasitology. 엔도투데이 기생충학]
![]() 1. 엔도투데이 기생충학 요점
1. 엔도투데이 기생충학 요점
1) 리뷰 (text): 내시경 검사 중 만나는 기생충 (PDF. 0.6 M)
2) 강의 Powerpoint: 내과 의사를 위한 위장관 기생충질환 (PDF. 6.5 M)
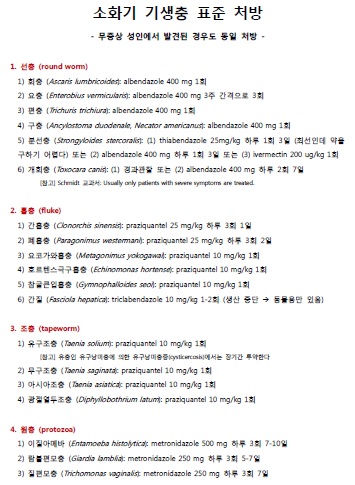
3) 기생충 표준처방전 (PDF. 0.1 M)
![]() 2. 위장관 기생충 GI parasites
2. 위장관 기생충 GI parasites
1) 기생충의 분류
2) 기생충의 역학
![]() 3. 선충 Round worms
3. 선충 Round worms
3) 편충 Trichuris trichiura - 어떤 질문
4) 구충 (=십이지장충) Hook worms - 어떤 질문
6) 분선충 Strongyloides stercoralis
8) 장모세선충 Capillaria philippinensis (암호: smcgi)
10) 스파르가눔
![]() 4. 흡충 Trematodes
4. 흡충 Trematodes
1) 간흡충 Clonorchis sinensis - C. sinensis egg in ENBD fluid (암호: smcgi)
2) 간질 Fasciola hepatica - triclabendazole
4) 요코가와 흡충 Metagonimus yokogawai
![]() 5. 조충 Tapeworms
5. 조충 Tapeworms
2) 아시아조충 Taenia asciatica (암호: smcgi)
![]() 6. 원충 Protozoas
6. 원충 Protozoas
1) 이질아메바 Entamoeba histolytica
![]() 7. 의용절지동물
7. 의용절지동물
1) 머릿니와 옴
2) 돌아온 빈대 (암호: smcgi)
3) SFTS (severe fever with thrombocytopenia syndrome, 중증열성혈소판감소증후군) and tick. 살인진드기
![]() 8. 기생충증의 치료
8. 기생충증의 치료
1) 소화기 기생충 표준 처방 (무증상 성인에서 발견된 경우도 동일 처방)
2) Albendazole과 mebendazole의 차이
3) 요충이 계속 재발합니다
4) 개회충에 의한 호산구성 농양은 치료가 필요합니까?
6) 간흡충에 대하여 praziquantel을 투약했는데 대변검사에서 계속 충란이 나옵니다
![]() 9. 기타
9. 기타
1) PDF EndoTODAY on GI Parasites
2) Paradox of the hygiene (암호: smcgi)
3) 단국대학교 서민 교수님 - 서민 on YouTube, 기생충같은 이야기 (blog) - 기생충열전
4) 기생충과 내시경 (서종옥)
5) 임상 기생충학 (채종일 편저)
6) 동아의대 기생충학 교실
![]()