EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 829. ESD for gastric tube cancer]
[Gastric cancer 829. ESD for gastric tube cancer]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
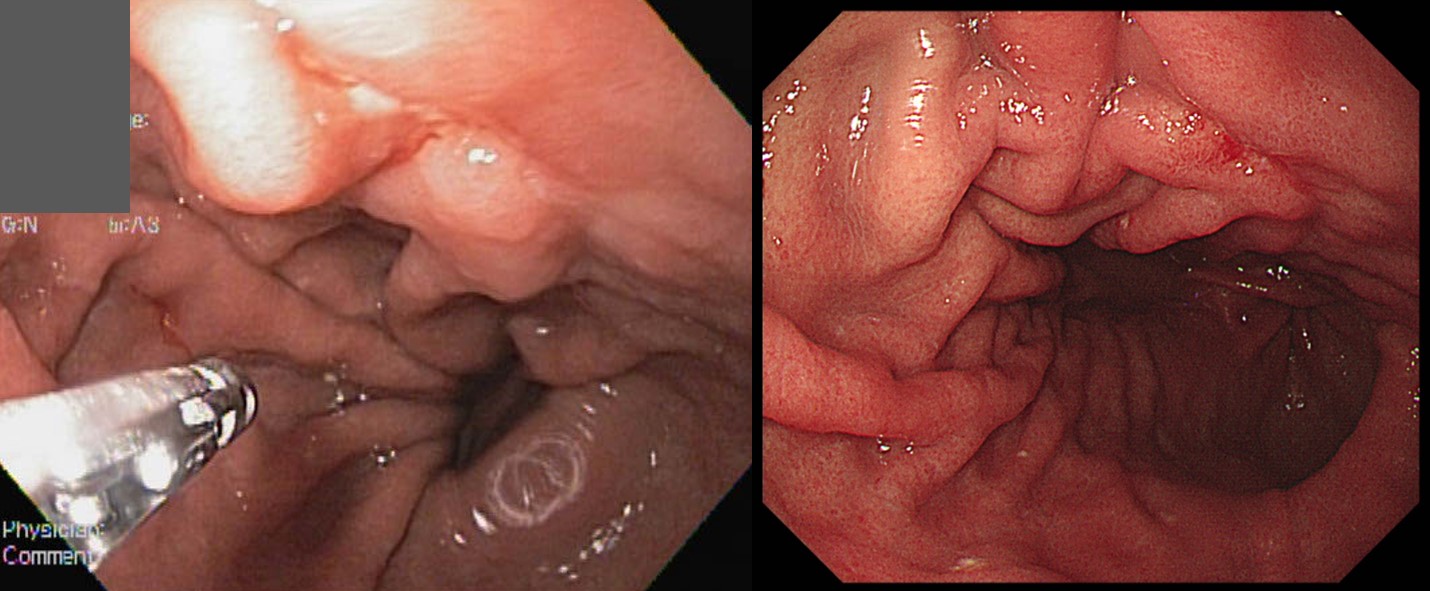
13 years after Ivor Lewis operation and chemotherapy for upper esophageal cancer (squamous cell carcinoma, pT3N1), gastric tube cancer was found at 37 cm from the incisor teeths. Biopsy showed tubular adenocarcinoma, moderately differentiated with focal poorly differentiated component.
Based on the endoscopic findings (depressed lesion, converging folds) and histologic findings, I recommended surgery. However, the surgeon recommended performing ESD due to the high surgical risk. ESD was done.
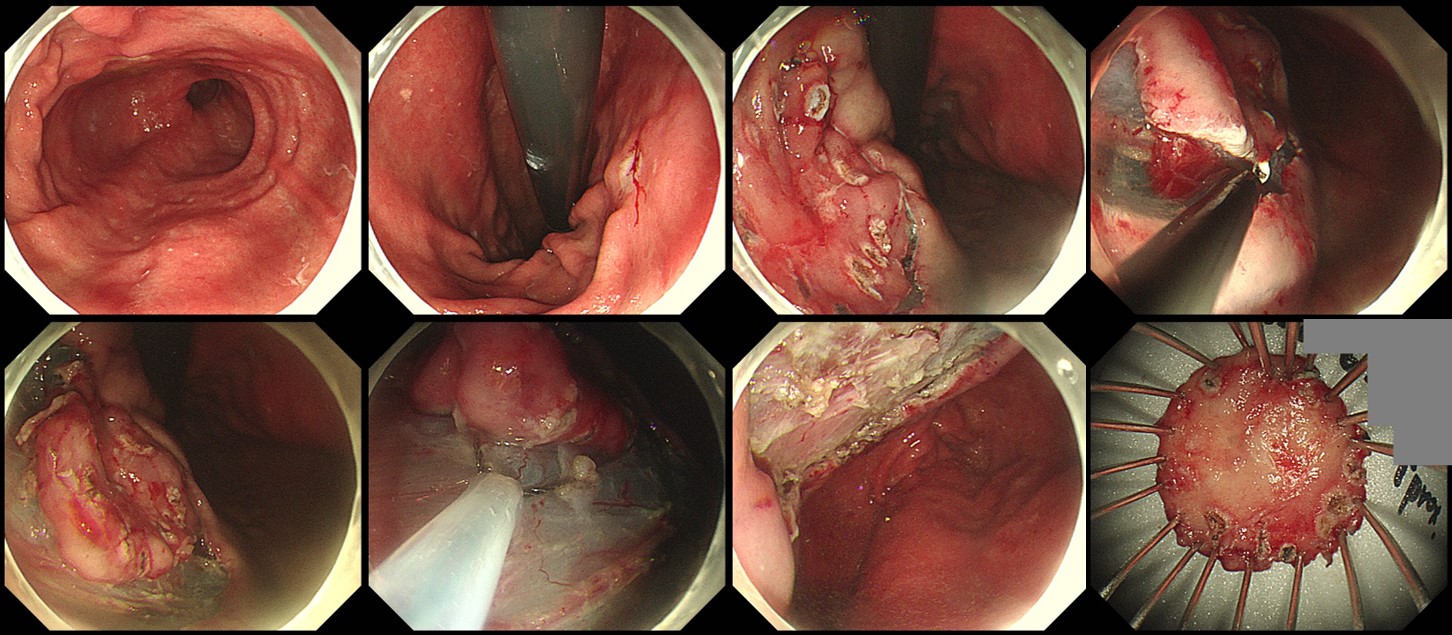
ESD: Early gastric carcinoma
1. Location : Intrathoracic stomach, IT 37cm
2. Gross type : EGC type IIa+IIb
3. Histologic type : tubular adenocarcinoma, moderately differentiated, >> tubular adenocarcinoma, poorly differentiated (poorly cohesive)
4. Histologic type by Lauren : mixed
5. Size of carcinoma : (1) longest diameter,14 mm (2) vertical diameter, 18 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion : 2000 ) (pT1b)
7. Resection margin : involved deep resection margin by carcinoma, safety margin : distal 4 mm, proximal 1 mm, anterior 4 mm, posterior 2 mm, deep 0
8. Lymphatic invasion : present (+++)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: present
Based on the pathology, surgery is necessary. The problem is the surgical risk. Surgical consultation was done. I explained the situation to the patient in detail.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2020-2-11)