EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Metachronous gastric cancer after ESD for EGC. РЬНУМК РчЙп] - №ћ
[Metachronous gastric cancer after ESD for EGC. РЬНУМК РчЙп] - №ћ
Clin Endosc 2018:51:253
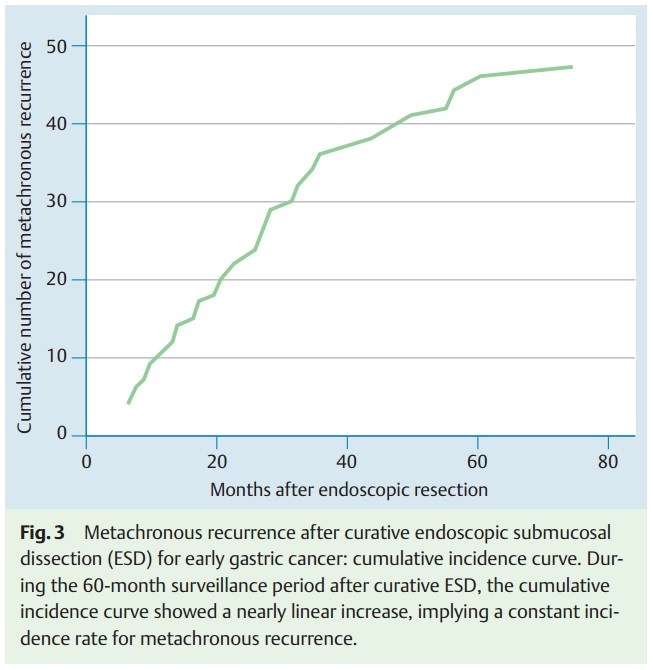
![]() 2015Гт ЛяМКМПяКДПј. ГЛНУАцРИЗЮ ФЁЗсЧб differentiate-type EGC ШЏРк 2,036Иэ Сп curative resectionРИЗЮ ГЊПдДј 1,692Иэ (83.2%) Сп ESDЗЮ ФЁЗсЧЯПДАэ 1Гт РЬЛѓ УпРћАќТћРЬ АЁДЩЧЯПДДј 1,306ИэПЁ ДыЧб long-term follow-up dataАЁ ЙпЧЅЕЧОњНРДЯДй (ЙЮКДШЦ. Endoscopy 2015).
2015Гт ЛяМКМПяКДПј. ГЛНУАцРИЗЮ ФЁЗсЧб differentiate-type EGC ШЏРк 2,036Иэ Сп curative resectionРИЗЮ ГЊПдДј 1,692Иэ (83.2%) Сп ESDЗЮ ФЁЗсЧЯПДАэ 1Гт РЬЛѓ УпРћАќТћРЬ АЁДЩЧЯПДДј 1,306ИэПЁ ДыЧб long-term follow-up dataАЁ ЙпЧЅЕЧОњНРДЯДй (ЙЮКДШЦ. Endoscopy 2015).
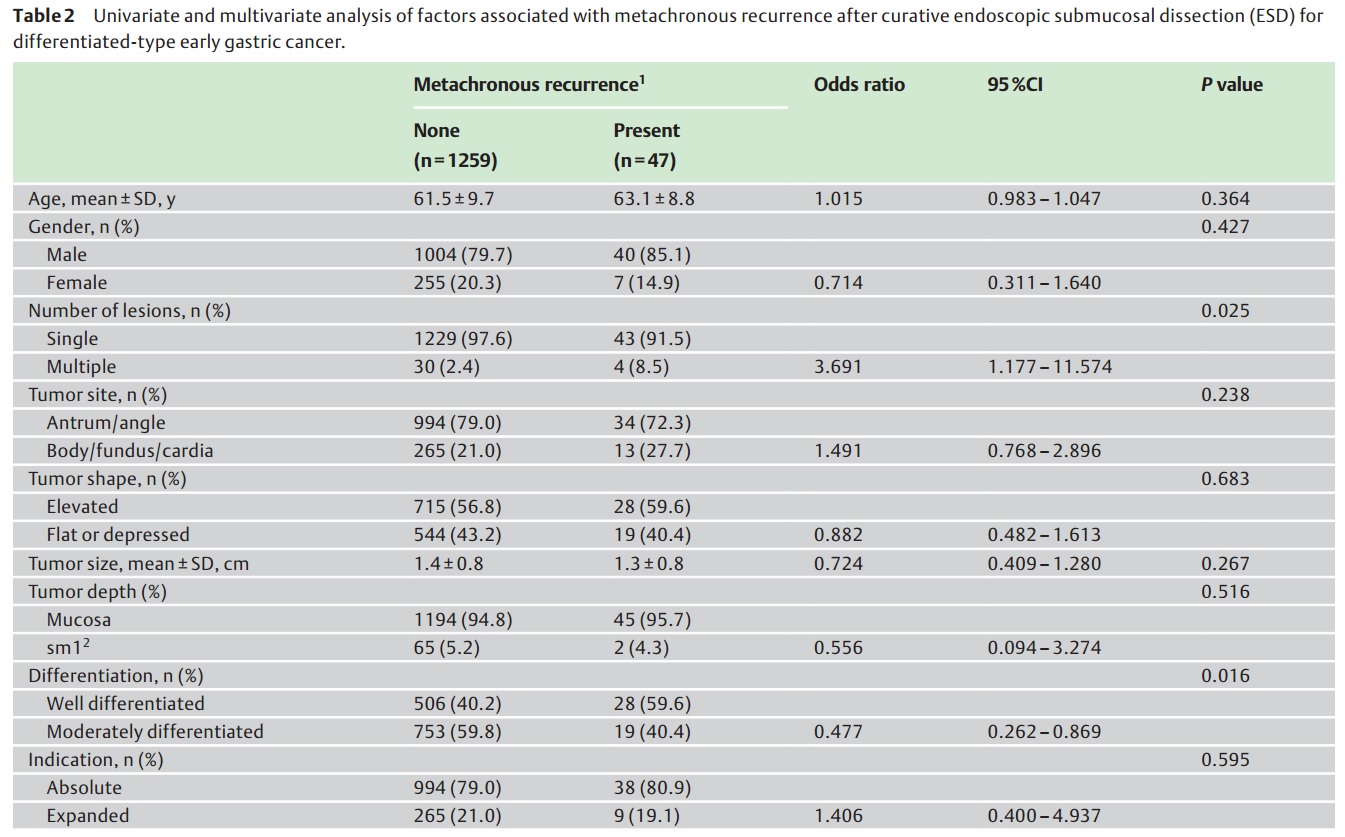
Metachronous recurrenceДТ 47Иэ (3.6%, 47/1306)ПЁМ ЙпАпЕЧОњНРДЯДй. СЖБтРЇОЯРЬ 44ПЙ (93.6%), СјЧрМКРЇОЯРЬ 3ПЙПДРИИч, 28ПЙ(60.0%)ДТ ESDЗЮ 19ПЙ(40.0%)ДТ МіМњЗЮ ФЁЗсЧЯПДНРДЯДй.
Metachronous recurrenceДТ УГРНПЁ ДйЙпМК КДМвПДДј ШЏРкПЭ КаШЧќРЬ well differentiatedПЁМ ИЙОвНРДЯДй.
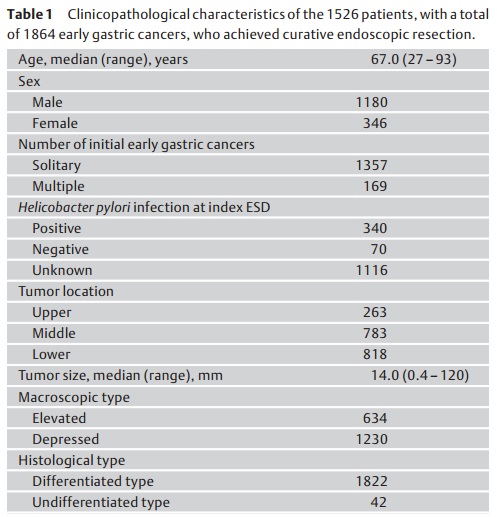
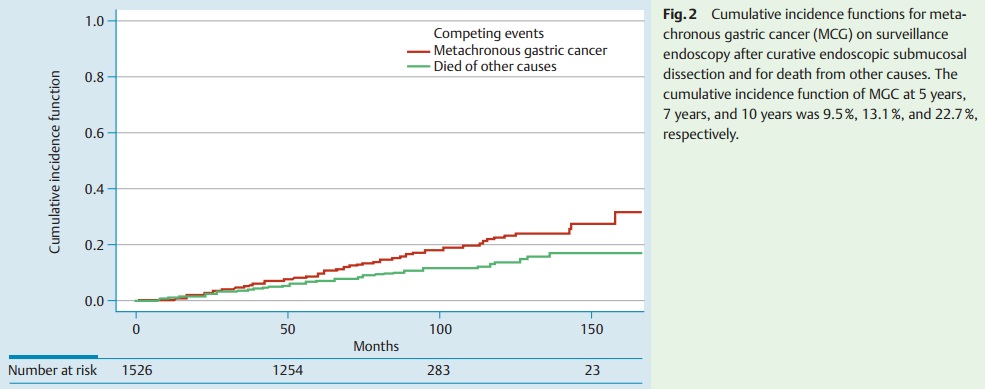
![]() 2015Гт ЕПАцОЯМОХЭ. РЬМвМК РЇОЯПЁ ДыЧб АЁРх ДыБдИ№ ПЌБИАЁ ЙпЧЅЕЧОњНРДЯДй (Abe S. Endoscopy 2015 Dec).
2015Гт ЕПАцОЯМОХЭ. РЬМвМК РЇОЯПЁ ДыЧб АЁРх ДыБдИ№ ПЌБИАЁ ЙпЧЅЕЧОњНРДЯДй (Abe S. Endoscopy 2015 Dec).
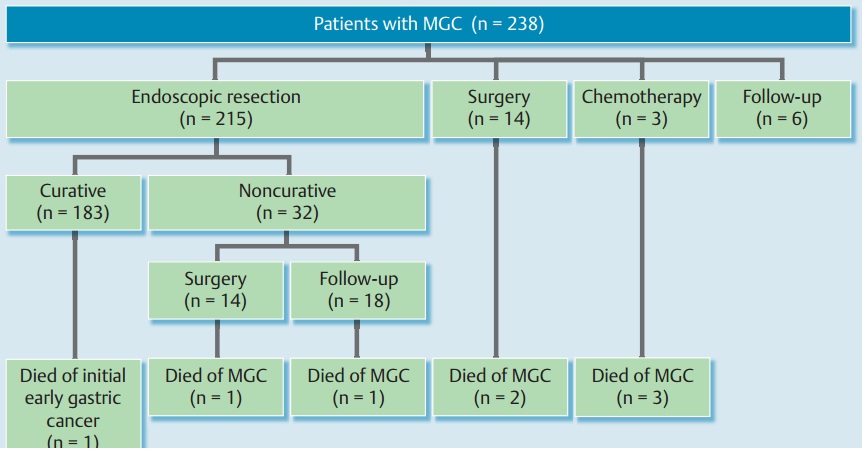
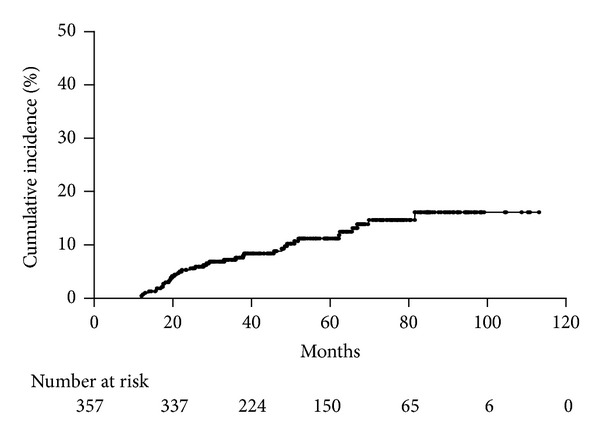
During a median follow-up period of 82.2 months, 238 patients developed MGC post-ESD resection of EGC. The 5-year, 7-year, and 10-year cumulative incidence functions of MGC were 9.5%, 13.1% and 22.7%, respectively. Male sex and multiple initial EGCs were independent risk factors for MGC in the Cox proportional hazard model. Of the 238 patients with MGC, 215 were treated with endoscopic resection, of which 183 achieved curative resection, although one patient later died of his initial EGC. A further 14 patients were treated surgically, three had metastatic disease and received palliative chemotherapy, and the remaining six were observed without any intervention. A total of seven patients died of MGC, five at least 5 years after their index ESD. The 5-year, 7-year, and 10-year DSSs were 99.2%, 98.6%, and 92.5%, respectively.
1999ГтКЮХЭ 2006ГтБюСі ЕПАцОЯМОХЭПЁМ ESDЗЮ ФЁЗсЧб EGC ШЏРкИІ КаМЎЧб РкЗсРдДЯДй. ЦђБе ПЌЗЩРЬ 67ММЗЮ ПьИЎГЊЖѓ ШЏРкКИДй ДйМв АэЗЩРЬОњНРДЯДй. РЬМвМК РЇОЯРЧ КѓЕЕАЁ 5ГтПЁ 9.5%ЗЮ ПьИЎГЊЖѓКИДй ПљЕюШї ГєОвДТЕЅ, Бз РЬРЏ Сп РЯКЮДТ adenomaАЁ cancerЗЮ СЖСїСјДмЕЧОњБт ЖЇЙЎРЯ АЭ ААНРДЯДй.
РЬМвМК РЇОЯ 238ПЙ Сп 28ПЙ(11.8%)ПЁМ МіМњРЬ РЬЗчОюСГНРДЯДй. 3ИэРЬ УЪФЁЗсЗЮ ЧзОЯФЁЗсИІ ЙоОвДйДТ СЁРЬ ЦЏРЬЧпНРДЯДй (РњШё БтАќПЁМДТ metastatic diseaseЗЮ ЙпАпЕШ РЬМвМК РЇОЯРК ОјОњНРДЯДй). 7Иэ(2.9%)РЬ РЬМвМК РЇОЯРИЗЮ ЛчИСЧЯПДНРДЯДй.
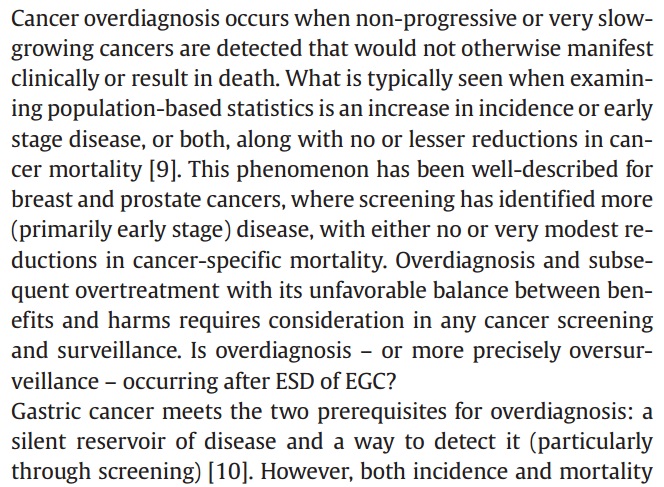
Abe ЕюРЧ ЕПАцОЯМОХЭ РЬМвМКРЇОЯ ПЌБИПЁ Imperiale ЕюРЬ editorialРЛ КйПДДТЕЅ ПТХы overdiagnosis issueРдДЯДй (Imperiale. Endoscopy 2015 Dec). АќСЁРЬ Тќ ИЙРЬ ДйИЃДйАэ Л§АЂЕЫДЯДй.
![]() РЯКЛ РхМв? Sugimoto T. Can J Gastroenterol Hepatol 2015 - Epub
РЯКЛ РхМв? Sugimoto T. Can J Gastroenterol Hepatol 2015 - Epub
The median follow-up period was 4.2 years. Metachronous gastric cancers were found in 23 of 155 patients (3.5% per year). No local recurrences were observed. The cumulative incidence of metachronous gastric cancer was significantly high in IM and NI in the corpus (P=0.0093 and P=0.0025, respectively [log-rank test]). The ORs for IM and NI in the corpus were 2.65 and 3.06, respectively, according to the Cox proportional hazards model (P=0.024 and P=0.0091, respectively).
![]() Boda T. Gastroenterol Res Pract 2014
Boda T. Gastroenterol Res Pract 2014
The annual incidence of metachronous tumors after ESD was 2.4%.
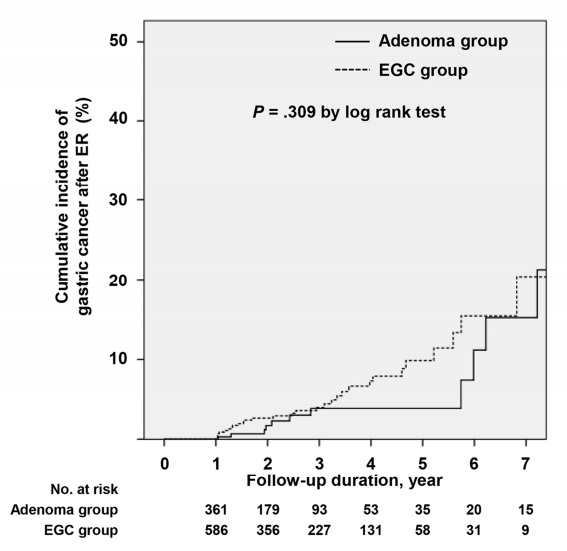
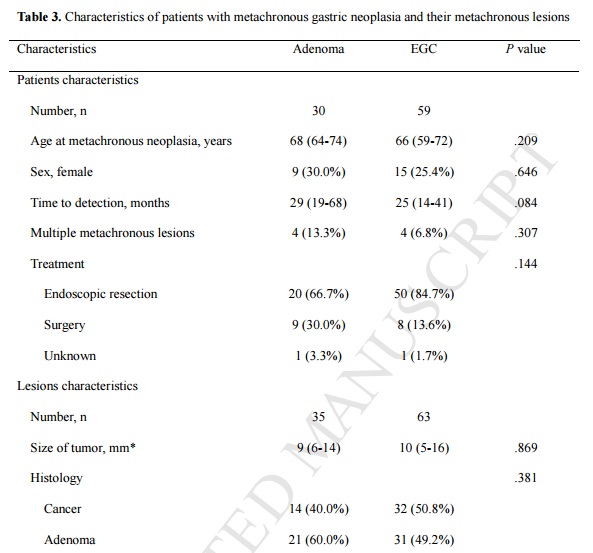
![]() 2015Гт 8Пљ АГВМКИ№КДПјПЁМ МБСОРЬГЊ РЇОЯ ГЛНУАц ФЁЗс ШФ РЬМвМК КДМвПЁ ДыЧб АсАњИІ ЙпЧЅЧЯПДНРДЯДй (Yoon SB. GIE). РњЕЕМБСОРЛ adenoma БКРИЗЮ, АэЕЕМБСОАњ ОЯРЛ EGC БКРИЗЮ ГЊДЉОњБт ЖЇЙЎПЁ ОрАЃ ШЅЕПЕЧДТ ИщРК РжНРДЯДйИИ... РњЕЕ МБСО ГЛНУАц ФЁЗс ШФПЁЕЕ ЛѓДчКЮКа РЬМвМК МБСОАњ РЬМвМК ОЯРЬ ЙпАпЕЧДйДТ СЁРЛ Рп КИПЉСжАэ РжНРДЯДй.
2015Гт 8Пљ АГВМКИ№КДПјПЁМ МБСОРЬГЊ РЇОЯ ГЛНУАц ФЁЗс ШФ РЬМвМК КДМвПЁ ДыЧб АсАњИІ ЙпЧЅЧЯПДНРДЯДй (Yoon SB. GIE). РњЕЕМБСОРЛ adenoma БКРИЗЮ, АэЕЕМБСОАњ ОЯРЛ EGC БКРИЗЮ ГЊДЉОњБт ЖЇЙЎПЁ ОрАЃ ШЅЕПЕЧДТ ИщРК РжНРДЯДйИИ... РњЕЕ МБСО ГЛНУАц ФЁЗс ШФПЁЕЕ ЛѓДчКЮКа РЬМвМК МБСОАњ РЬМвМК ОЯРЬ ЙпАпЕЧДйДТ СЁРЛ Рп КИПЉСжАэ РжНРДЯДй.
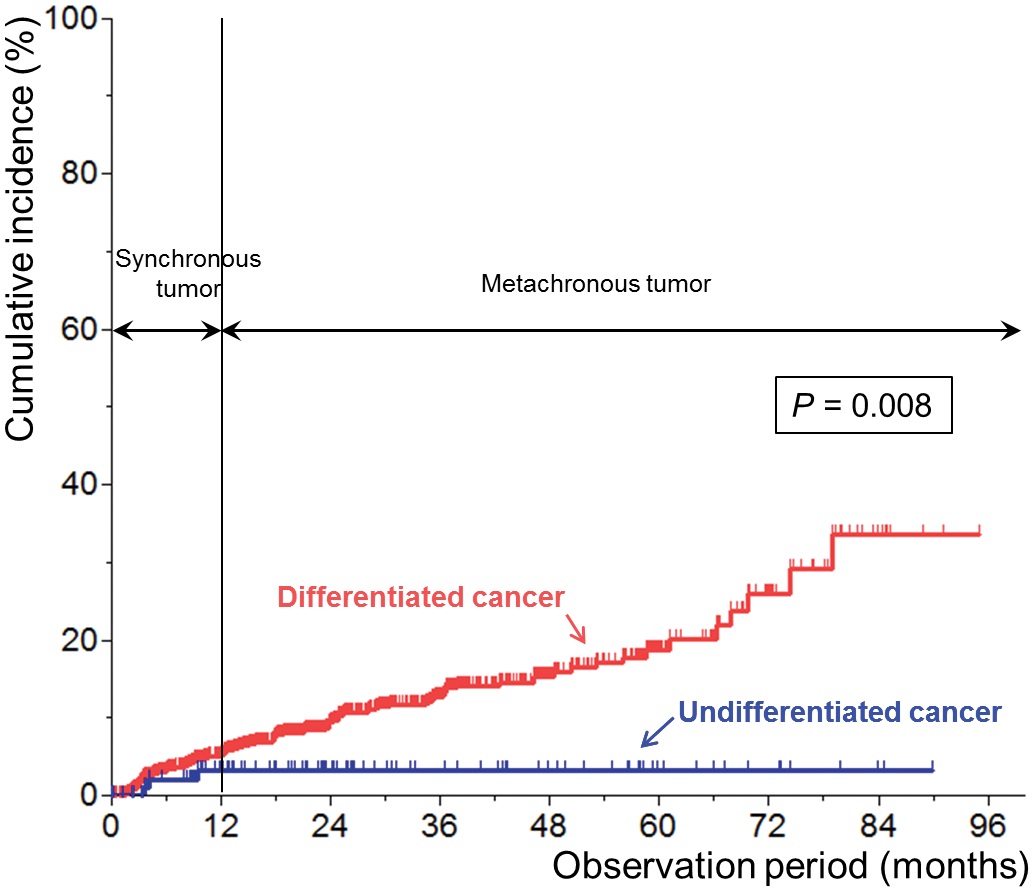
![]() 2016Гт ПЌММДыЧаБГ (Park CH. PLoS One 2016). Undifferentiated type EGCПЁ ДыЧб ГЛНУАц ФЁЗс ШФ РЬМвМК РчЙпРЬ РћОњНРДЯДй. НЩСіОюДТ ЕПНУМК РчЙпЕЕ РћОњДйАэ ЧеДЯДй. АсЗа("These findings suggest that ESD should be actively considered as a possible treatment for undifferentiated type EGCs")РК СЖБн РЬЛѓЧпНРДЯДй. РЬМвМК РчЙпРЬ РћДйДТ АЭРЬ ОюЖЛАд ГЛНУАц ФЁЗсРЧ РћРРСѕ ШЎДыЗЮ ПЌАсЕЧДТСі РЬЧиЧв Мі ОјНРДЯДй.
2016Гт ПЌММДыЧаБГ (Park CH. PLoS One 2016). Undifferentiated type EGCПЁ ДыЧб ГЛНУАц ФЁЗс ШФ РЬМвМК РчЙпРЬ РћОњНРДЯДй. НЩСіОюДТ ЕПНУМК РчЙпЕЕ РћОњДйАэ ЧеДЯДй. АсЗа("These findings suggest that ESD should be actively considered as a possible treatment for undifferentiated type EGCs")РК СЖБн РЬЛѓЧпНРДЯДй. РЬМвМК РчЙпРЬ РћДйДТ АЭРЬ ОюЖЛАд ГЛНУАц ФЁЗсРЧ РћРРСѕ ШЎДыЗЮ ПЌАсЕЧДТСі РЬЧиЧв Мі ОјНРДЯДй.
БзЗБЕЅ 2010Гт ААРК БтАќПЁМ ЙпЧЅЧб ГэЙЎ(Seo JH. Digestion 2010)Ањ АсЗаРЬ ЙнДыРЮ АЭ ААНРДЯДй. 2010ГтПЁДТ "undifferentiated histology and upper location of the primary lesion were correlated with the occurrence of metachronous gastric cancer"ПДБт ЖЇЙЎРдДЯДй.
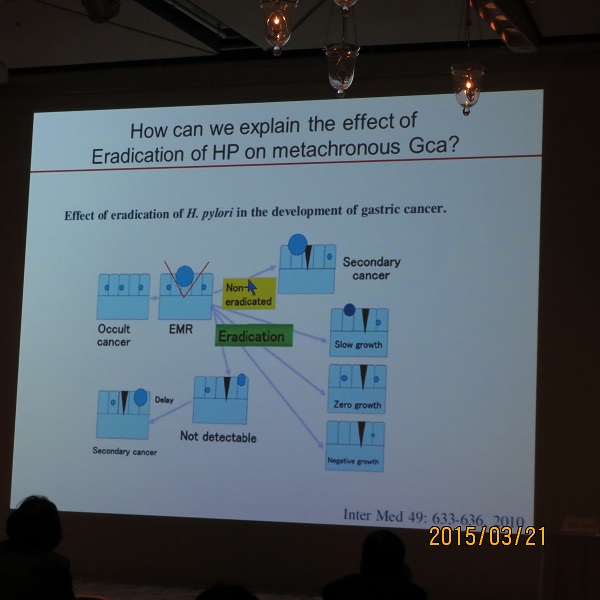
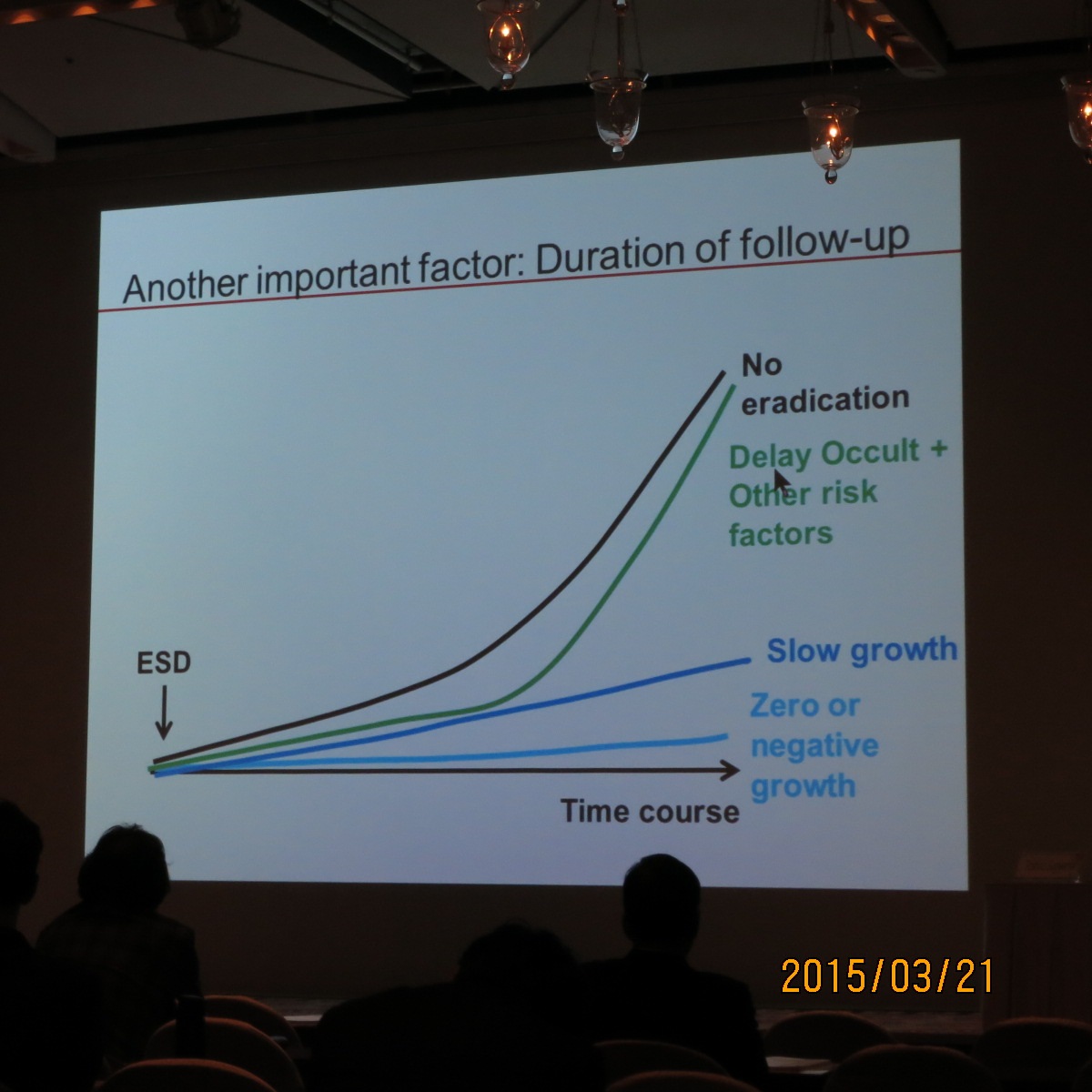
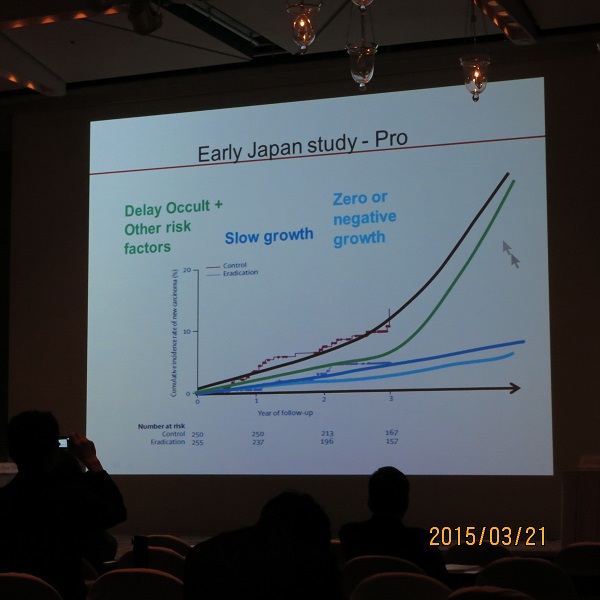
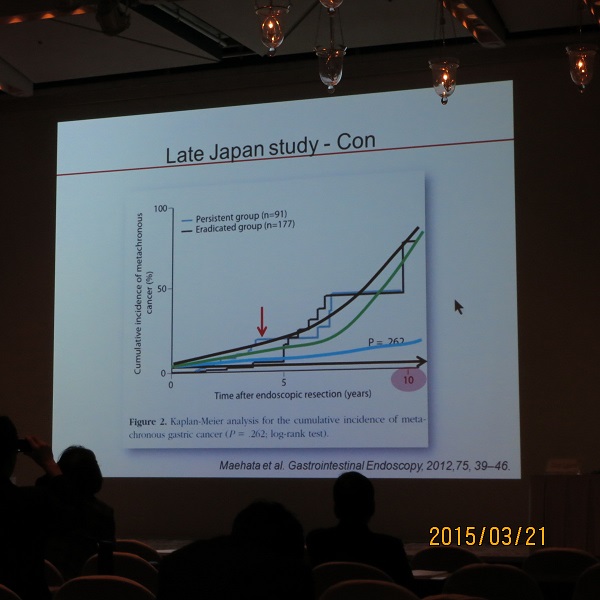
![]() 2015Гт 3Пљ 20РЯ ЧбРЯЧяИЎФкЙкХЭЧаШИ АцКЯДыЧаБГ РќМКПь БГМіДд АРЧ. Metachronous recurrence after ESD
2015Гт 3Пљ 20РЯ ЧбРЯЧяИЎФкЙкХЭЧаШИ АцКЯДыЧаБГ РќМКПь БГМіДд АРЧ. Metachronous recurrence after ESD
РќМКПь БГМіДдВВМ АцКЯДыРЧ ESD ШФ metachronous recurrenceПЁ ДыЧб РкНХРЧ ЕЅРЬХИИІ КИПЉСжНХ ШФ КёНСЧб ДйИЅ ПЌБИ АсАњЕщРЛ КИПЉСжИщМ ИХПь СпПфЧб АЁМГРЛ СІНУЧЯМЬНРДЯДй. ESD ШФ Hp СІБеРЬ metachronous cancer ЙпЛ§ПЁ ЙЬФЁДТ ПЕЧтРК follow-up БтАЃПЁ ЕћЖѓ ДоЖѓСјДйАэ МГИэЧЯМЬНРДЯДй.
Hp СІБе УЪБтПЁДТ ОЯРЧ СјЧрРЛ ОяСІЧеДЯДй. ЕћЖѓМ Hp СІБеРЬ metachronous cancer ЙпЛ§РЛ СйРЬДТ АЭРИЗЮ ГЊПЩДЯДй. БзЗЏГЊ РЇОЯРК HpРЬПмРЧ ДйИЅ ИЙРК ПфРЮПЁ РЧЧи ЙпЛ§ЧеДЯДй. ЕћЖѓМ РхБтАЃ УпРћАќТћРЛ ЧЯИщ Hp РЬПмРЧ ДйИЅ РЮРк(diet, atrophic anc metaplastic gastritis, epigenetic change)РЧ ПЕЧтРЬ ЛѓДыРћРИЗЮ СпПфЧиСіЙЧЗЮ Hp СІБеПЁ РЧЧб ШПАњАЁ ЛѓДыРћРИЗЮ РлОЦСіАэ АсБЙ ТїРЬАЁ ОјДТ АЭРИЗЮ ГЊПЩДЯДй. РЬ КаОпПЁ ДыЧб МГИэ Сп РЬУГЗГ АЃАсЧЯАэ ИэЗсЧб АЁМГРК УГРНРЬОњНРДЯДй. РќМКПь МБЛ§Дд. ИкС§ДЯДй.
АќЗУГэЙЎ: Failure of Helicobacter pylori eradication and age are independent risk factors for recurrent neoplasia after endoscopic resection of early gastric cancer in 283 patients. Kwon YH. Aliment Pharmacol Ther 2014;39:609-18
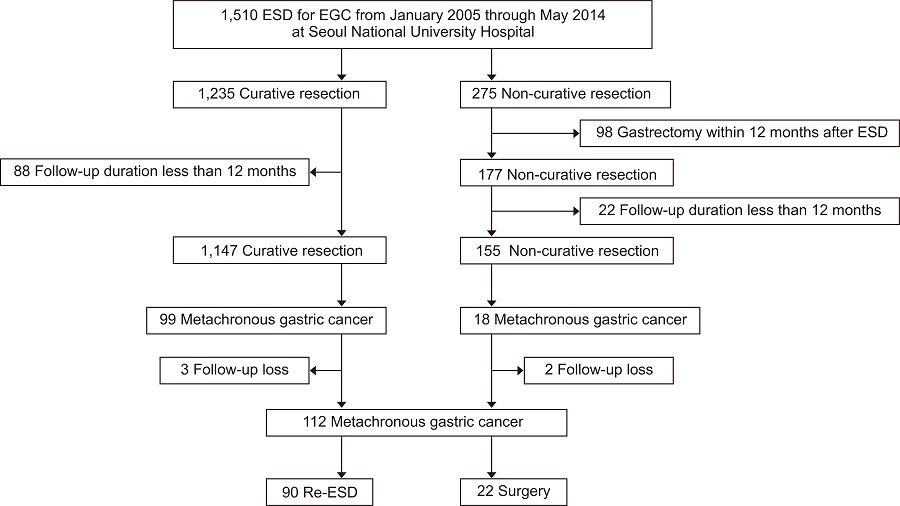
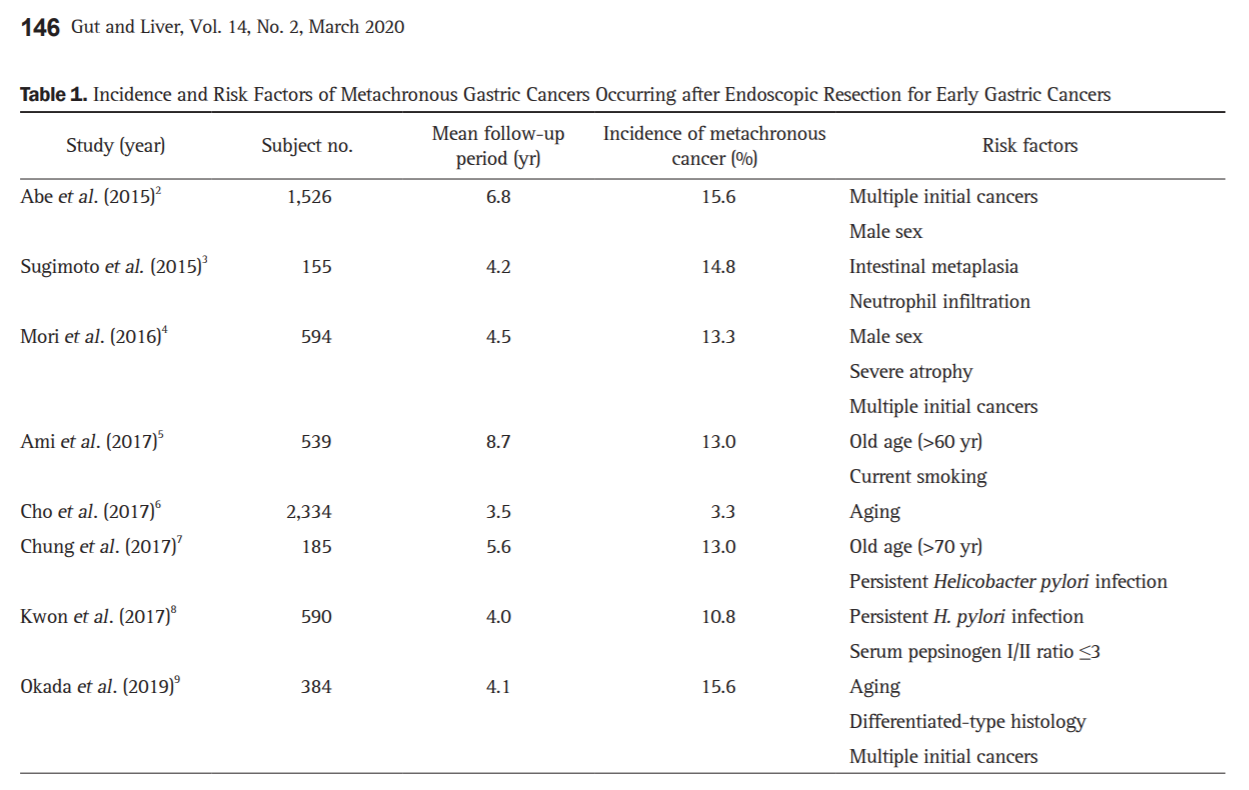
![]() 2020Гт МПяДы (Gut and Liver 2020)
2020Гт МПяДы (Gut and Liver 2020)
МПяДы ЦРПЁМДТ 112Иэ Сп 90Иэ (80.3%)РЛ ESDЗЮ ФЁЗсЧпДйДТ ГюЖѓПю МКРћРЛ КИАэЧЯПДНРДЯДй.
РЬ ГэЙЎПЁ ДыЧб editorialПЁДТ БзАЃ ЙпЧЅЕШ ГэЙЎЕщРЧ ГЛПыРЬ Рп СЄИЎЕЧОю РжОњНРДЯДй.
![]() [Cases]
[Cases]
ГЏЙЎ РЇОЯ ESD ЧЯПДДТЕЅ ЖЧ ДйИЅ ЙцЧтПЁМ ГЏЙЎ РЇОЯРЬ ГЊПШ
РЬМвМК РЇОЯ Сп МіМњРЬ ЧЪПфЧб АцПьАЁ СОСО ЙпАпЕЫДЯДй.
РЬМвМК РЇОЯ Сп ESD ШФ МіМњРЬ ЧЪПфЧб АцПьЕЕ РжНРДЯДй.
Stomach, endoscopic submucosal dissection:
Early gastric carcinoma
1. Location : mid antrum
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 13 mm (2) vertical diameter, 12 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion : 1000 Ї) (pT1b)
7. Resection margin : involved deep resection margin by carcinoma with cauterized artifacts safety margin : distal 15 mm, proximal 13 mm, anterior 16 mm, posterior 14 mm, deep 0 mm (sm only)
8. Lymphatic invasion : present (+++)
9. Venous invasion : suspicious
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
2008Гт synchronous EGCsЗЮ ESD (x2) ШФ УЙ РЬМвМК РЇОЯ(2011)РК ESDЗЮ ЧиАсЧв Мі РжОњРИГЊ ЕЮЙјТА РЬМвМК РЇОЯ(2015)РК ESD ШФ ОЦЗЁПЭ ААРЬ МіМњРЬ ЧЪПфЧб АсАњАЁ ГЊПдНРДЯДй.
Stomach: LC of mid body, ESD:
Early gastric carcinoma
1. Location : body, lesser curvature
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 11 mm (2) vertical diameter, 8 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion : 400 Ї) (pT1b)
7. Resection margin : involved deep resection margin by carcinoma with cauterized artifacts safety margin : distal 6 mm, proximal 9 mm, anterior 8 mm, posterior 10 mm, deep 0 Ї
8. Lymphatic invasion : present
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
АэЕЕМБСО ГЛНУАцФЁЗс ШФ РЬМвМКРИЗЮ РЇОЯРЬ ЙпАпЕЧДТ АцПьЕЕ РжНРДЯДй.
Stomach, ESD : Early gastric carcinoma
1. Location : antrum, anterior wall
2. Gross type : EGC type IIb
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 12 mm (2) vertical diameter, 8 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 7 mm, proximal 4 mm, anterior 4 mm, posterior 8 mm, deep 600 Ї
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
Metachronous cancer develops in 1-2%/year after ESD for EGC. Six years after ESD for EGC, a metachronous cancer was found in the lesser curvature aspect of the high body. ESD was done again.
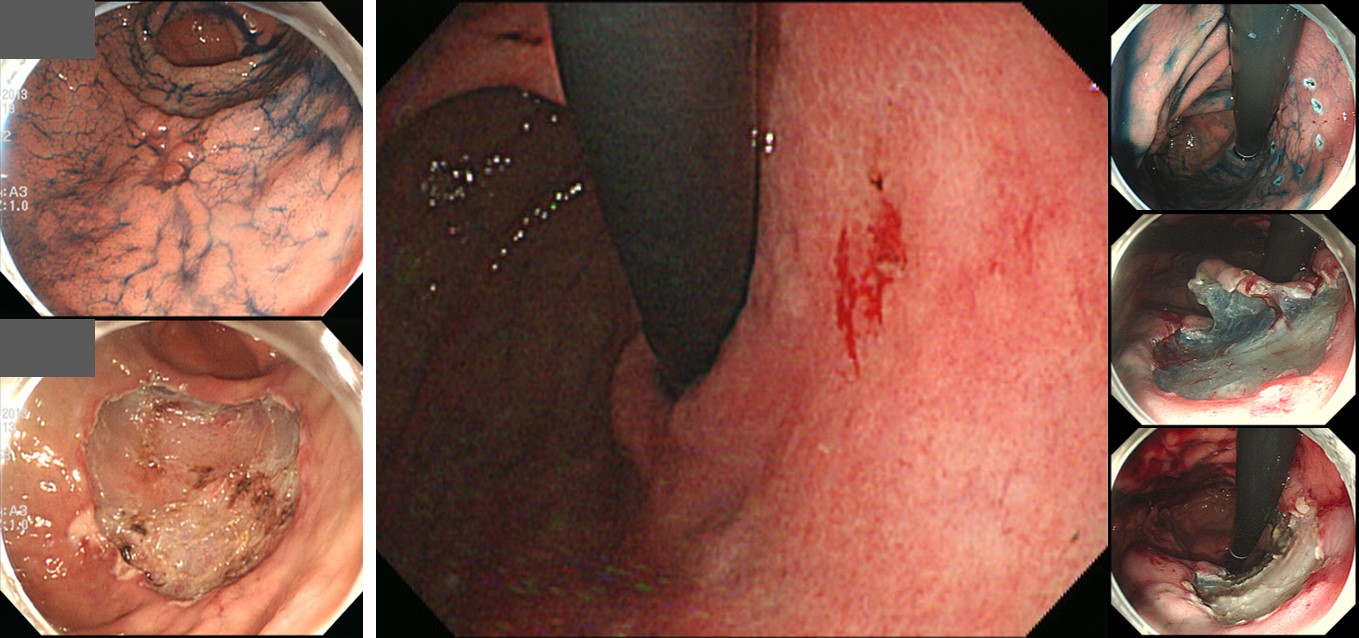
[1st ESD (left)]
ESD: Early gastric carcinoma
1. Location : proximal antrum, greater curvature
2. Gross type : EGC type IIb+IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 14 mm (2) vertical diameter, 13 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 11 mm, proximal 12 mm, anterior 18 mm, posterior 12 mm
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent[2nd ESD (right)]
ESD: Early gastric carcinoma
1. Location : high body, lesser curvature
2. Gross type : EGC type IIa+IIc
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 18 mm (2) vertical diameter, 14 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N) safety margin : distal 7 mm, proximal 6 mm, anterior 12 mm, posterior 10 mm, deep 200 Ї
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
Borrmann type 4 gastric cancer may develop after ESD.
2021Гт (F/64)
Biopsy at peritoneal seeding nodule
![]() [FAQ]
[FAQ]
[2021-3-31. ЧаЛ§ СњЙЎ]
ЙнКЙРћРИЗЮ РчЙпЧЯДТ EGCПЁ ДыЧиМ ОеРИЗЮ ОюЖЛАд ЧиОпЧвСі БУБнЧеДЯДй. ПјЗЁ БзГЩ ESDЧб ШЏРкЖѓИщ АцАњАќТћРЛ ЧЯАкСіИИ, РЬЗИАд РчЙпЧЯДТ ШЏРкРЧ АцПьПЁДТ ДйРН ЙјПЁ ЖЧ РчЙпЧв АцПь ЯЧѲ̳̜РЛ АэЗСЧиОп ЧЯГЊПф?
[2021-4-1. РЬСиЧр ДфКЏ]
ССРК СњЙЎ АЈЛчЧеДЯДй. Чб ИЖЕ№ЗЮ ДфЧЯИщ РчЙпРЧ СОЗљПЁ ЕћЖѓ ДйИЈДЯДй.
СЖБтРЇОЯ ГЛНУАцФЁЗс ШФ КДИЎЧаРћРИЗЮ ПЯНЧѲЗЮ ЦЧДмЕШ ШЏРкРЧ ЕПРЯ КДМв(index cancer)РЧ БЙМв, ИВЧСР§ РќРЬ ШЄРК ПјАн РчЙпРК ЛѓДчШї РћНРДЯДй (EndoTODAY Longterm outcome of endoscopic curative resection of EGC). БЙМв РчЙпРК ЛѓШВПЁ ЕћЖѓМ МвРлМњ, second ESD, ШЄРК МіМњРЛ РћПыЧеДЯДй. ИВЧСР§ РќРЬДТ ДчПЌШї МіМњРЛ ЧеДЯДй. ПјАн РчЙпРК ОШХИБюПю АцПьРЬСіИИ ЧзОЯФЁЗсИІ ЧеДЯДй (EndoTODAY Extragastric recurrence after ESD for EGC).
Index cancerРЧ РчЙпКИДйДТ РЬМвМК (ьЖсЖрѕ) РчЙпРЬ ШчЧеДЯДй (EndoTODAY РЬМвМК РчЙп). РЇ ГЛРЧ ДйИЅ МгПЁМ РЇОЯРЬ ЛѕЗЮ ЙпЛ§ЧЯДТ АцПьРЮЕЅ Бз КѓЕЕДТ 1ГтПЁ 1-2%РдДЯДй. 5ГтРЬИщ 5-10%ЖѓДТ РЧЙЬРЬДЯ ЛѓДчШї ШчЧеДЯДй.
РЬМвМК РчЙпРЧ ФЁЗсПјФЂРК РЇОЯРЬ УГРН СјДмЕЧОњРЛ ЖЇПЭ КёНСЧеДЯДй. ГЛНУАц ЧѲ̜ РћРРСѕРЬИщ ГЛНУАц ЧѲ̜РЛ ЧЯАэ МіМњ РћРРСѕРЬИщ МіМњРЛ ЧеДЯДй. 2ЙјТА, 3ЙјТА, 4ЙјТА.... ОЯРЬОњДйДТ РЬРЏЗЮ ГЛНУАц ЧѲ̜РЛ АэЗСЧЯСі ОЪАэ МіМњЧЯДТ АцПьДТ АХРЧ ОјНРДЯДй. РЇДТ МвСпЧб РхБтРЬАэ АЁДЩЧЯИщ ГЁБюСі АЁСіАэ ЛчДТ АЭРЬ РЏИЎЧЯБт ЖЇЙЎРдДЯДй. Subtotal gastrectomyГЊ total gastrectomy ШФ ЛюРЧ СњРК ЛѓДчШї ЖГОюС§ДЯДй.
[2021-3-31. ЧаЛ§ СњЙЎ]
НУМњРЛ ЧЯБт Рќ СЖСїАЫЛчПЁМДТ well differentiatedПДДТЕЅ, ESD ШФ СЖСїАЫЛч АсАњАЁ moderately differentiatedЗЮ ГЊПдДйИщ, РЬ АцПьПЁДТ МіМњРЛ АэЗСЧиОпЧЯГЊПф?
[2021-4-1. РЬСиЧр ДфКЏ]
ESD РќШФ ММЦїЧќРЧ ТїРЬДТ ЛѓДчЧеДЯДй (EndoTODAY Pathologic discrepancy). СЖСїАЫЛчДТ КЮКа АЫЛчРЬАэ ESD АЫУМПЁ ДыЧб АЫЛчДТ РќУМ АЫЛчРЬБт ЖЇЙЎРдДЯДй. КЮКаРЛ КИАэ РќУМИІ ПЙУјЧЯДТ АЭРК ЧзЛѓ СЄШЎЧЯСі ОЪНРДЯДй.
ESD РќШФ ММЦїЧќРЬ ДйИЃАд ГЊПУ ЖЇРЧ ПјФЂРК АЃДмЧеДЯДй. ESD АЫУМПЁ ДыЧб КДИЎАсАњПЁ ЕћЖѓ additional surgery ПЉКЮИІ АсСЄЧеДЯДй.
![]() [References]
[References]
1) ъж ESD ШФ ГЛНУАц МвАп (РЬСиЧр). ЛяМКМПяКДПј Winter school 2018

© РЯПјГЛНУАцБГНЧ ЙйИЅГЛНУАцПЌБИМв РЬСиЧр. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.