EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Interval cancer. 중간암] - 終
[Interval cancer. 중간암] - 終
[바쁜 분을 위한 요약]
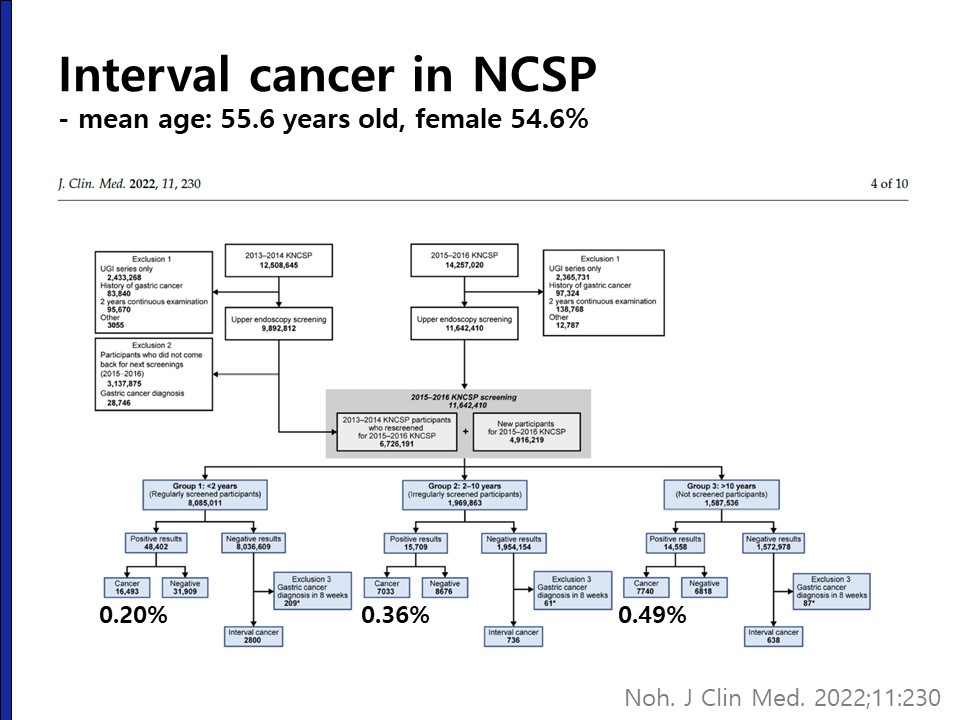
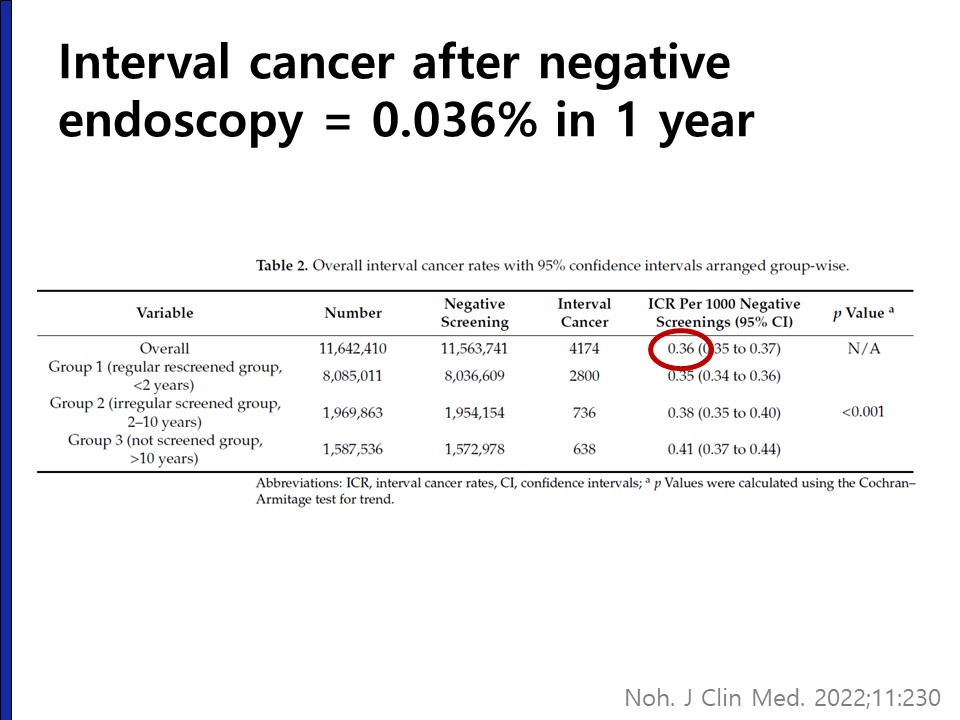
내시경에 대한 강의를 들으면 '이 수진자의 2년을 책임진다'라는 마음가짐으로 검사하라는 이야기를 듣게 된다. 환자들은 내시경 검사에서 특이 소견이 없으면 적어도 위암은 없다고 생각한다. 그러나 위내시경은 그만큼 완벽하지 않다. 위내시경도 검사의 하나일 뿐이며 나름대로의 민감도와 특이도가 있다. 민감도가 100%인 검사는 없다. 우리나라 국가암검진프로그램(National Cancer Screening Program)에서 시행한 위내시경의 위암 발견율과 negative endoscopy 후 interval cancer의 비율에 대한 자료가 발표되었다. 평균 55.6세, 여성 54.6%인 대상군에서 국가암검진 위내시경의 암 진단율은 0.26%였다. 400명 검사하면 한 명이 암으로 진단되는 셈이다. 2년 이내 위내시경 경험자에서는 0.22%, 2년초과 10년 이내 내시경 경험자에서는 0.36%, 10년 이상 무경험자에서는 0.49%였다. Negative endoscopy 후 1년 이내 암진단율은 0.036%였습니다. 1-2년 사이 위내시경을 받으셨던 500명 중 한명에서 다음 검진 내시경에서 위암이 발견된다는 자료이다. 작은 조기위암은 흔히 놓칠 수 있다. 간혹 맹점에 위치한 진행성 위암이나 보만 4형 진행성 위암이 발견되지 못하는 예가 있어 주의가 필요하다.
1. Interval gastric cancer 중간 위암
2. Interval colon cancer 중간 대장암
3. Surveillance colonoscopy: moving toward precision surveillance
4. References
![]() 1. Interval gastric cancer. 중간 위암
1. Interval gastric cancer. 중간 위암
[연세대학교 논문 (2015)]
미국에서 interval colon cancer라는 개념이 활발하게 연구되고 있습니다. 최근 Gut and Liver에 연세대학교에서 interval gastric cancer라는 개념의 논문을 발표하였습니다 (Gut Liver 2015). 검진 간격이 명확히 확립되어 있지 않고, 왜 짧은 간격으로 검사를 받았는지 뚜렷하지 않았습니다. 따라서 interval cancer의 정의에 꼭 들어맞는 경우는 아닙니다만 몇 가지 흥미로운 포인트가 있어 소개합니다.
연구자들의 건진 내시경실에서 발견된 위암의 14.3%가 interval gastric cancer였습니다.
양 군간의 procedure time에 차이가 없다는 점이 흥미로웠습니다. 약 4분으로 차이가 없었습니다. 궁금한 것은 마지막 내시경 검사의 procedure time인데 이에 대한 자료는 없었습니다. 정말 가려운 곳은 아무도 긁어주지 않는군요.
제가 표를 제시하지는 않았지만 interval cancer 16예 중 11예가 undifferentiated type 암이었고 5예가 differentiated type 암이었다는 점도 주목하시기 바랍니다. 진행성 위암은 undifferentiated type 암이 1예, differentiated type 암이 1예였습니다.
[우리나라 국가암검진 프로그램 (National Cancer Screening Program, NCSP) 참여자의 중간암]
매우 중요한 자료가 발표되었습니다 (J Clin Med 2021). 국가암검진프로그램(National Cancer Screening Program)에서 시행한 내시경 검사에서 위암 발견율과 negative endoscopy 후 interval cancer의 비율입니다. 평균 55.6세, 여성 54.6%인 대상군에서 국가암검진 내시경 검사의 암 진단율은 0.26%였습니다. 400명 검사하면 한 명이 암으로 진단된다는 것입니다. 2년 이내 내시경 경험자에서는 0.22%, 2년초과 10년 이내 내시경 경험자에서는 0.36%, 10년 이상 무경험자에서는 0.49%였습니다. Negative endoscopy 후 1년 이내 암진단율 (= interval cancer)은 0.036%였습니다.
[Post-Endoscopy Upper Gastrointestinal Cancers (2022)]
Post-Endoscopy Upper Gastrointestinal Cancers에 대한 메타분석입니다 (Gastroenterology 2022). 초록의 abstract 부분을 옮깁니다.
"A total of 2696 citations were screened and 25 studies were included, comprising 81,184 UGI cancers, of which 7926 were considered PEUGIC. For PEUGIC assessed within 6 to 36 months of a "cancer-negative" EGD, the mean interval was approximately 17 months. Patients with PEUGIC were less likely to present with dysphagia (odds ratio [OR] 0.37) and weight loss (OR 0.58) and were more likely to present with gastroesophageal reflux (OR 2.64) than detected cancers. PEUGICs were more common in women in Western populations (OR 1.30). PEUGICs were typically smaller at diagnosis and associated with less advanced disease staging compared with detected cancers (OR 2.87 for stage 1 vs 2-4). Most EGDs (>75%) were abnormal preceding diagnosis of PEUGIC."
[Interval advanced gastric cancer after negative endoscopy (2023)]
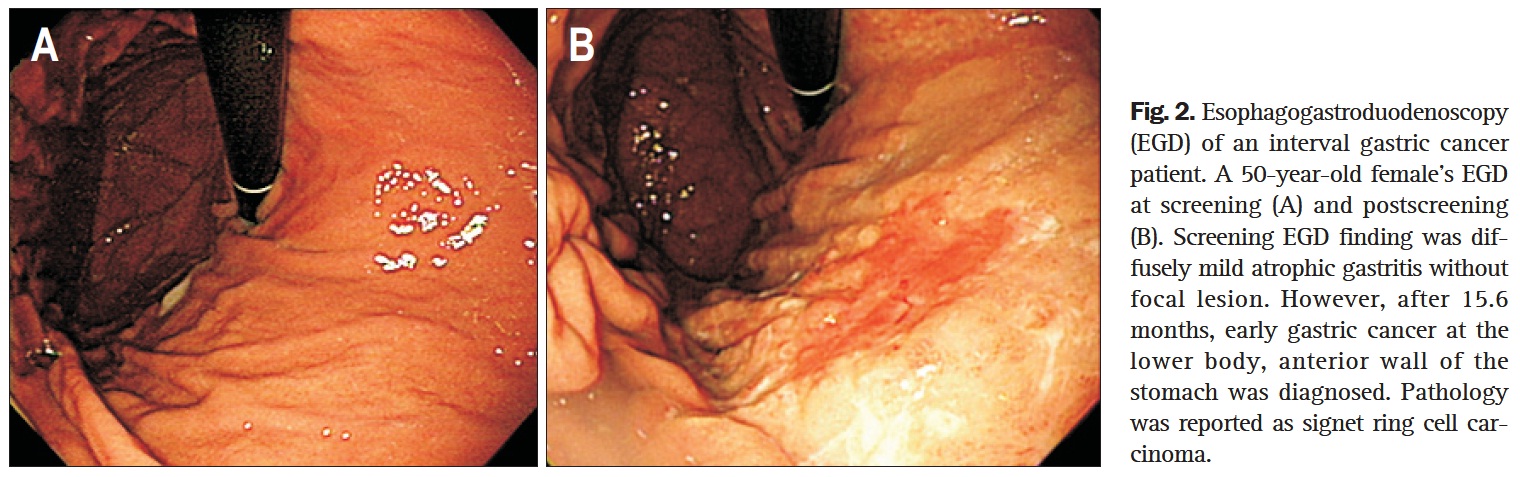
삼성서울병원 김태준 교수님께서 중간위암 중 진행성 위암을 중심으로 분석한 자료입니다 (Clin Gastroenterol Hepatol 2023). 내시경 검사 시간이 가장 중요한 인자였습니다. 빠른 내시경보다 바른 내시경이 필요합니다.
16년 연구 기간 동안 내시경 검사를 2번 이상 받은 19만여 명 중 위암으로 진단된 1,319명(0.68%) 중 제외기준에 속한 환자를 제외한 1,257명을 분석하였습니다. 102명(8.1%)은 진행성 위암, 1,155명(91.9%)은 조기위암이었습니다.
Interval AGC와 interval EGC의 분포에 뚜렷한 차이가 있었습니다.
현실적으로 조기위암은 miss하기 쉽기 때문에 진행성 위암을 중심으로 분석하였습니다. 중간 진행성 위암과 관련된 인자로는 관찰시간이 가장 중요했습니다.
보만 4형의 경우 예후가 훨씬 나빴습니다.
Discussion의 마지막 문장을 소개합니다.
"In conclusion, interval cancer is an inevitable part of gastric cancer screening programs. However, a better understanding of the predictors of advanced IGCs can identify areas for enhancing the possibilities of earlier detection. The implications of this study suggest that gastric observation time affects the diagnostic accuracy of EGD. We suggest measurement of observation time as a surrogate marker for examination quality. Further prospective studies could validate the quality threshold and confirm the concept that a minimum amount of time may be required for quality EGD examination."
[영국 NHS의 상부위장관 중간암 (2023)]
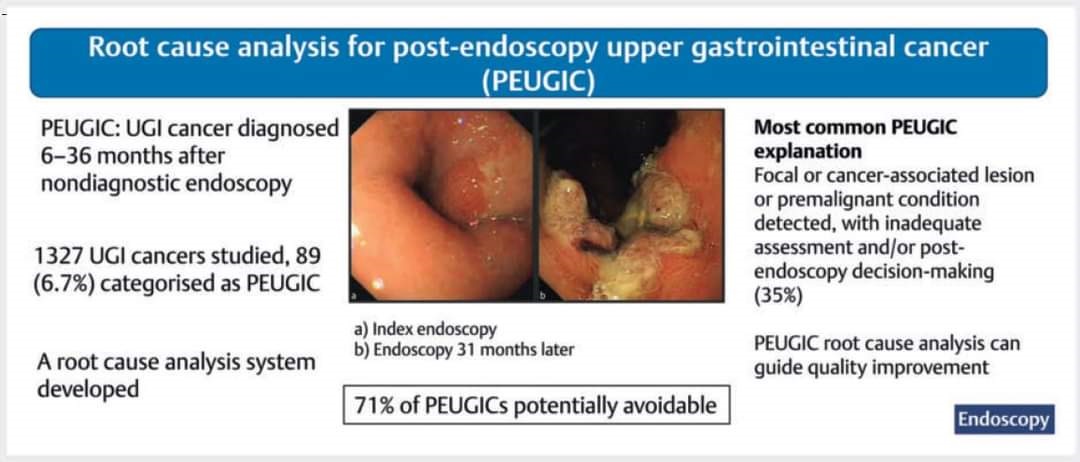
2023년 1월호 Endoscopy 지에 영국 Birmingham에서 interval gastric cancer에 대한 근본원인분석 논문을 발표하였습니다 (Endoscopy 2023). Index endoscopy 6-36개월 후 발견된 암으로 정의되었고 빈도는 6.7%였으며 71%는 potentially avoidable, 45%는 outcome이 달라질 수 있었다고 해석되었습니다. 영국에서 진행된 연구로 위암보다 식도암이 많았고 70% 이상에서 palliative treatment를 받을 정도로 advanced stage에서 진단되었기 때문에 우리나라에 그대로 적용하기는 어려운 자료입니다. 상부위장관 암 환자의 70%가 손쓸 수 없는 단계에서 발견된다니... 영국 NHS의 수준을 알 수 있습니다. 한 마디로 엉터리입니다. 배울 점이 있을까요? 논문은 그럴싸하지만 의사로서의 실력은 형편없다고 하겠습니다. 제가 가장 싫어하는 상황입니다. 환자는 실력있는 의사를 좋아합니다.
PEUGICs (post-endoscopy upper GI cancers)를 interval cancer와 non-interval cancer로 나누고 있습니다.
Editorial에는 quality factor에 대한 언급이 있습니다. Adequate training이 첫번째로 나열되어 있습니다.
"Identified operator factors include: adequate training and currency of practice; adequate mucosal visualization and inspection times; the use of established classification systems to describe endoscopic findings; and identification and photodocumentation of relevant anatomical landmarks and detected lesions. Nonoperator factors include: the use of high resolution endoscopes; adequate allocation of procedure times; and dedicated lists for patients at higher risk of cancer, such as those undergoing surveillance procedures for BE or gastric intestinal metaplasia and atrophy. Importantly, these statements provide a set of auditable performance indicators that both the individual and institution can use for quality assurance and benchmarking."
Quality indicator를 적용함에 있어 서구에서도 법적인 문제를 걱정하고 있습니다.
"One of the barriers to the implementation of such systems are concerns that the findings may be used to define individual accountability or in the medicolegal setting. It is critical that the system should not be used for such purposes, but only for its intended purposes of improving the quality of UGI endoscopy and thereby reducing the rate of PEUGIC."
![]() 2. Interval colon cancer 중간 대장암 (2020년. 삼성서울병원 김태준 교수님 강의)
2. Interval colon cancer 중간 대장암 (2020년. 삼성서울병원 김태준 교수님 강의)
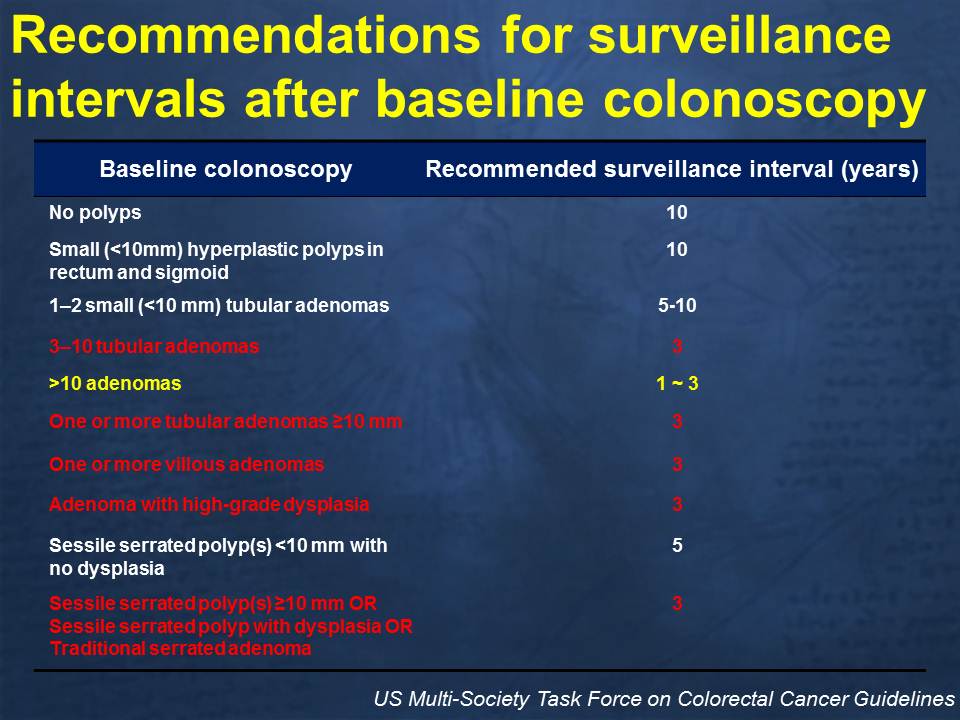
국내 가이드라인입니다. 대장내시경이 정상이거나 1-2개의 작은 tubular adenoma를 제거한 경우는 5년 후 추적내시경이 권고되고 있습니다. 3-4개의 선종을 제거한 경우, 혹은 다른 고위험인자가 있으면 보통 3년 후 재검하면 됩니다. Piecemeal로 제거되어 완벽하게 제거되었는지 자신이 없다면 3개월 후입니다. 대장내시경 1년 혹은 2년 후 추적 대장내시경이 권유되는 항목은 하나도 없습니다. 현실 의료와 가이드라인은 이만큼 차이가 있습니다.
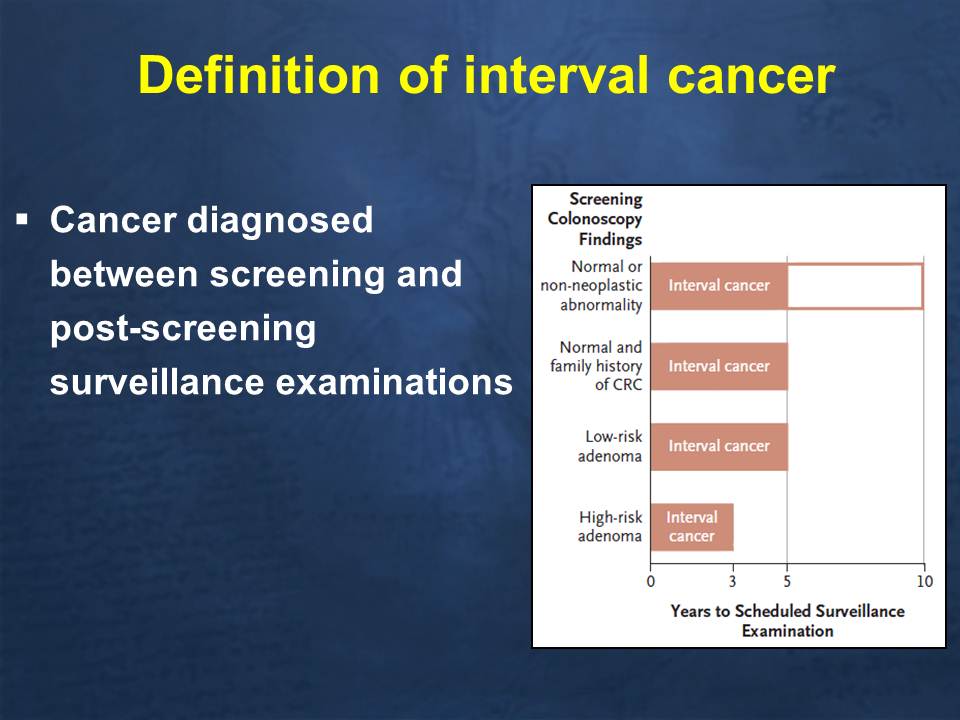
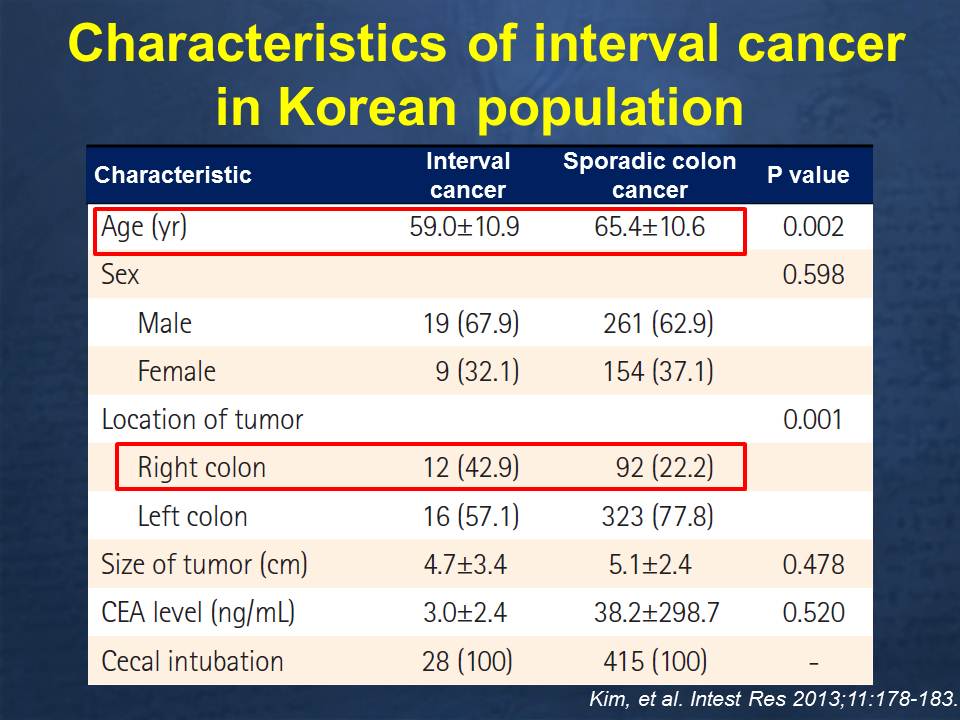
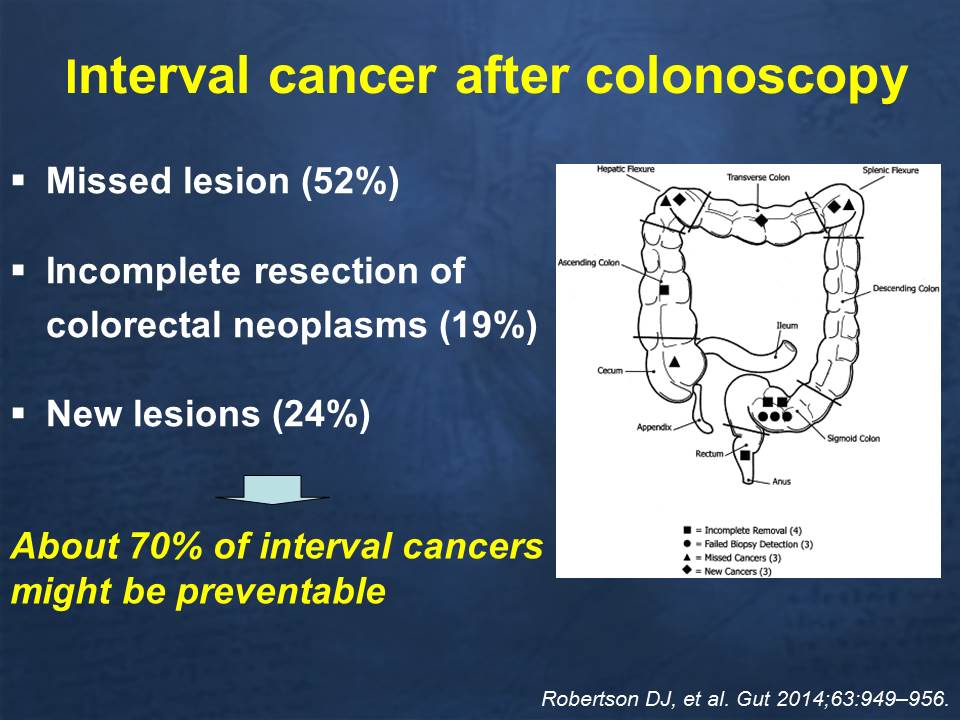
중간암은 전체 대장암의 6%입니다.
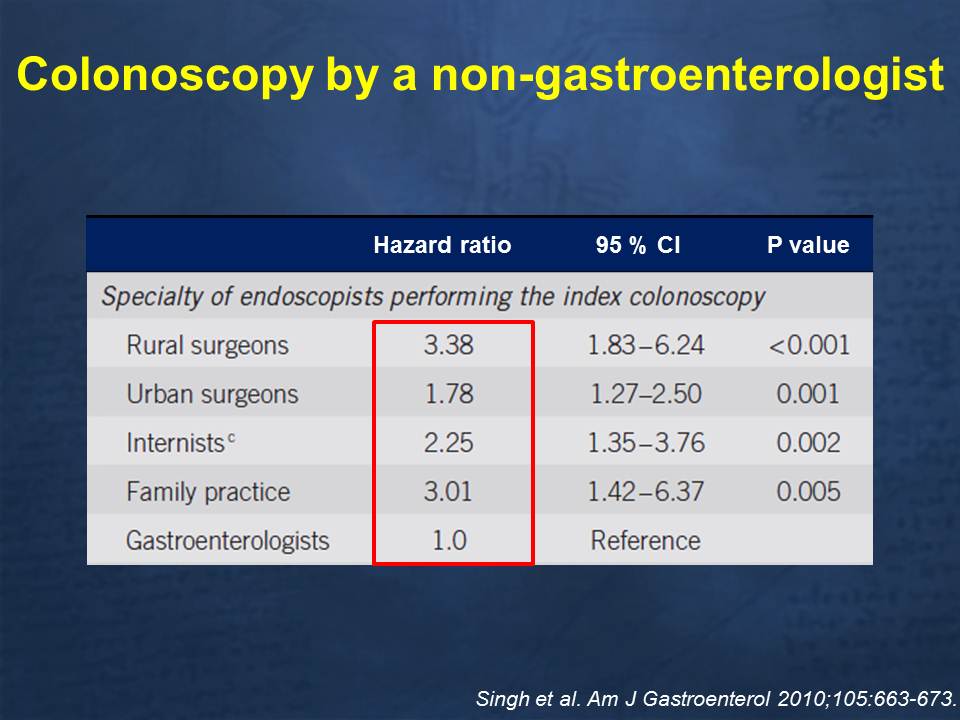
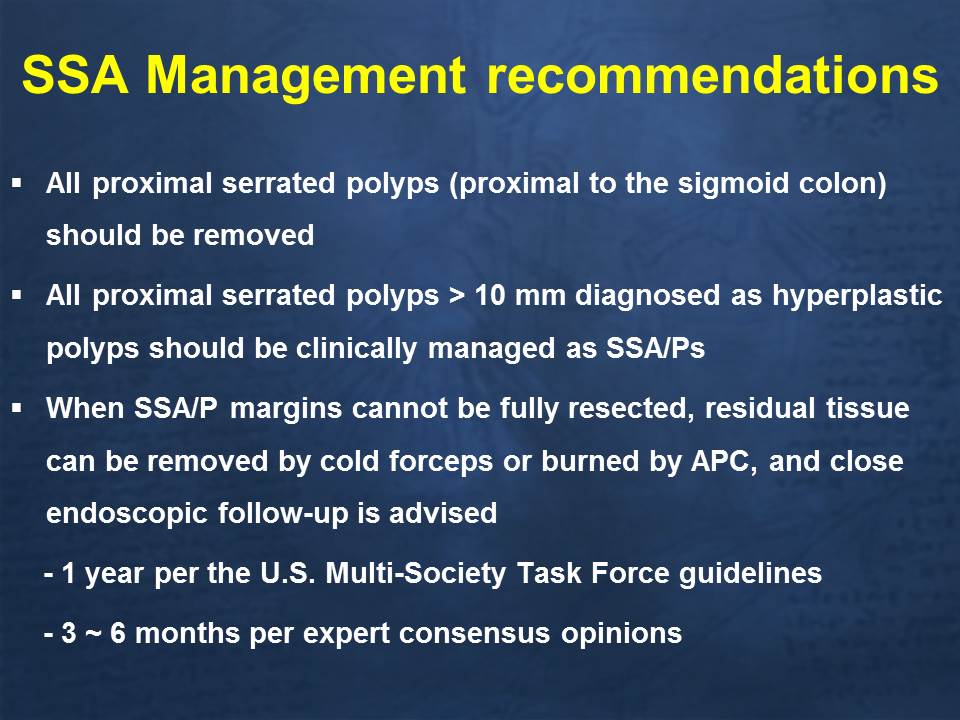
중간암은 여자에 많고, 우측 대장에 많고, 완벽하게 제거하지 못한 경우에서 많습니다.
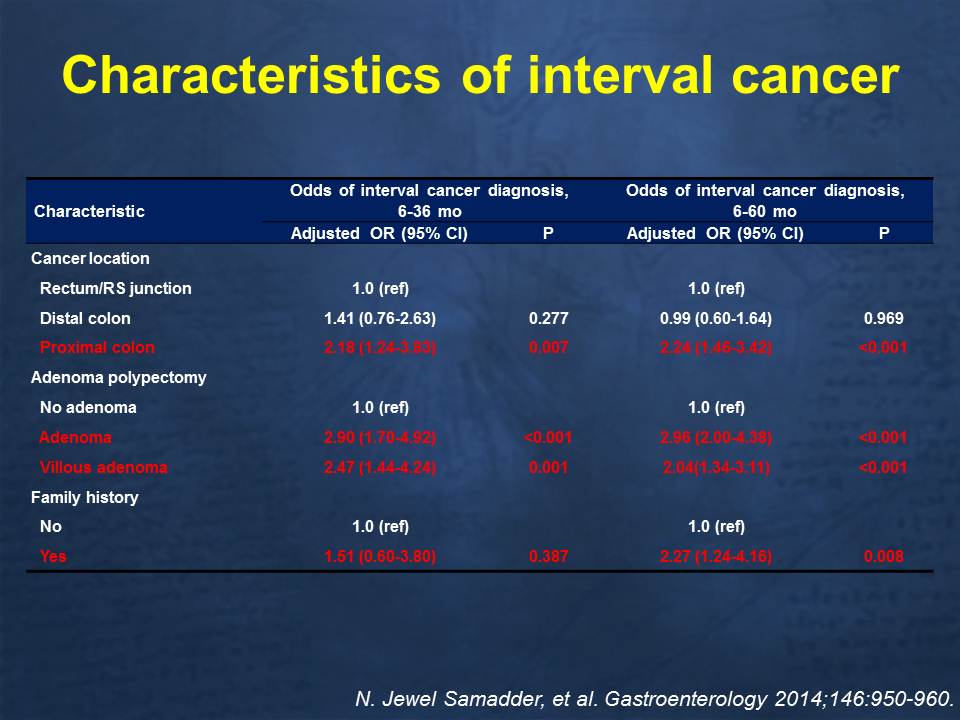
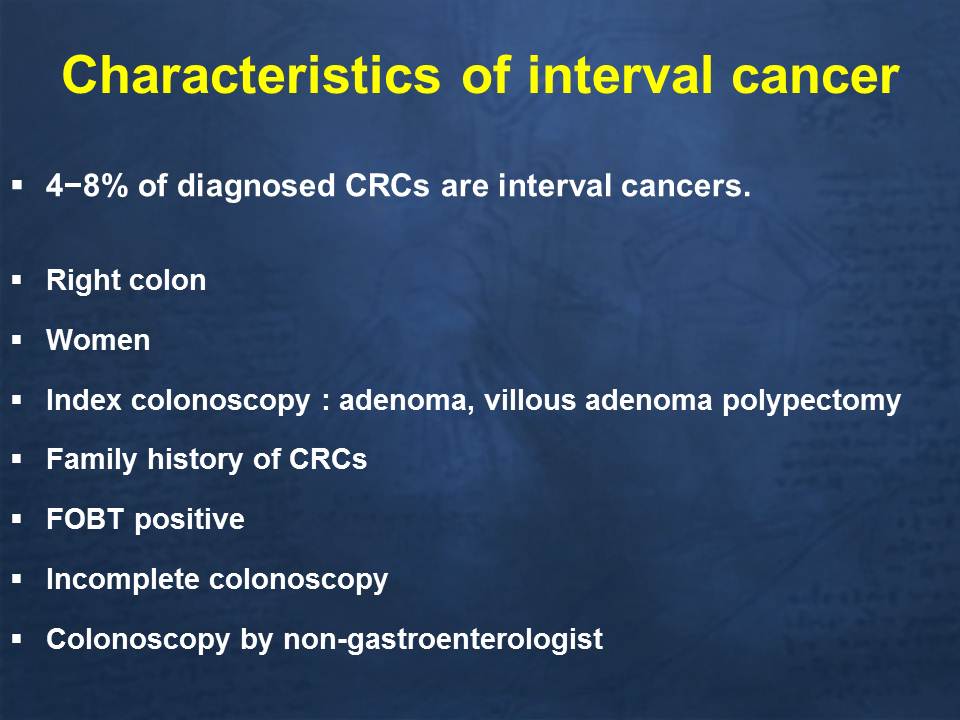
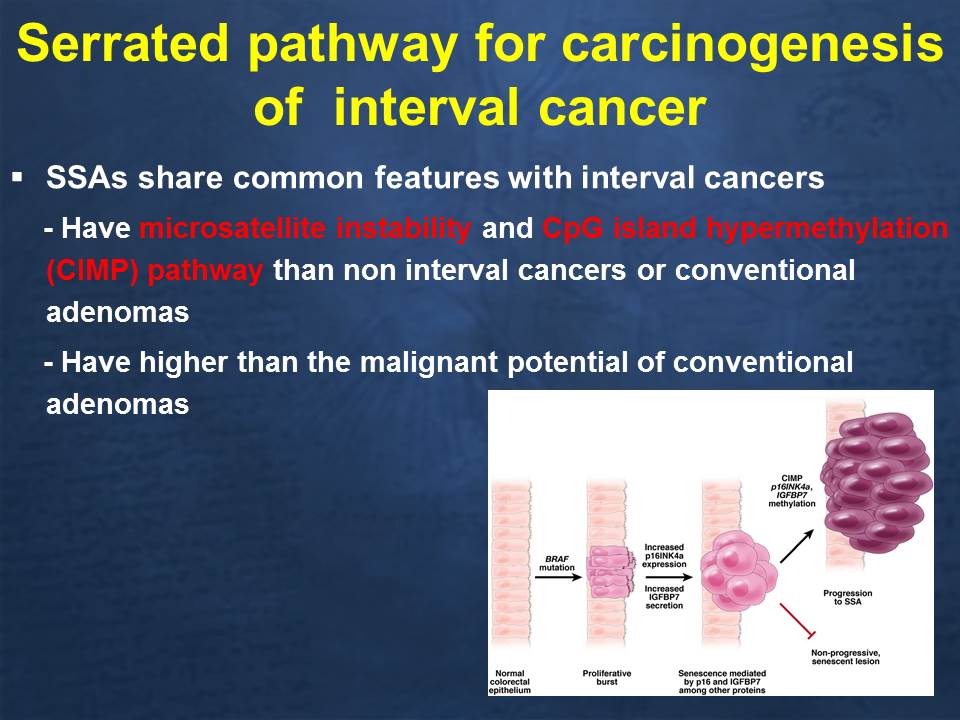
Sessile serrated adenoma는 중간암의 중요 원인입니다.
Withdrawal time을 8-9분까지 늘리자고 주장하는 분들의 데이타입니다. 제가 해보면 6분도 짧지 않은 시간인에 9분이라니...... 너무하군요.
우리나라에서 FUSE를 사용하는 분이 계신다는 이야기를 듣고 놀랐습니다. 말하자면 3 화면을 동시에 봐야 하니 어지러울 수 밖에 없을 것 같습니다. 저는 시도하지 않을까 합니다.
![]() 3. Surveillance colonoscopy: moving toward "precision surveillance" (2019-3-22 Expert meeting 김태준 교수님 강의)
3. Surveillance colonoscopy: moving toward "precision surveillance" (2019-3-22 Expert meeting 김태준 교수님 강의)
Low risk adenoma란 1 또는 2개의 작은 선종을 의미하는데 이런 경우 우리나라 가이드라인에서는 5년 후 미국 가이드라인에서는 5년에서 10년 후 f/u 할 것을 권유하고 있습니다. Low risk adenoma 에 대한 surveillance interval은 adenoma 가 없는 정상 그룹과 비슷하게 제시됩니다. 그 이유는 low risk adenoma 군의 (1) metachronous advanced adenoma 발생률, (2) 대장암 발생률, (3) 대장암 사망률이 general population이나 no adenoma 군과 비슷하기 때문입니다.
우리나라 연구입니다. High risk group은 metachronous advanced adenoma 발생률이 높았지만 low risk group은 정상 그룹과 차이가 없었습니다.
Low-risk adenoma 와는 다르게 high risk adenoma는 대장암 사망 위험도가 더 높았습니다.
Index colonoscopy 후 대장암 발생률입니다. Advanced adenoma가 있었던 사람이 대장암에 잘 걸립니다. 그러나 non-advanced adenoma였던 사람은 선종이 없었던 사람과 차이가 없었습니다.
같은 자료를 그래프로 보여주는 것입니다.
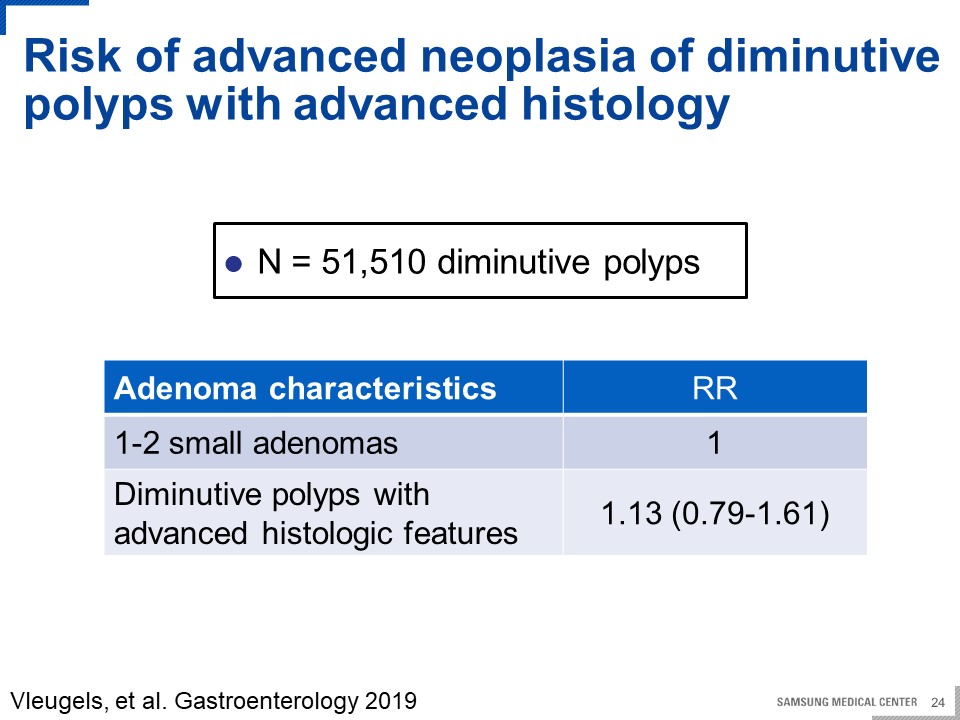
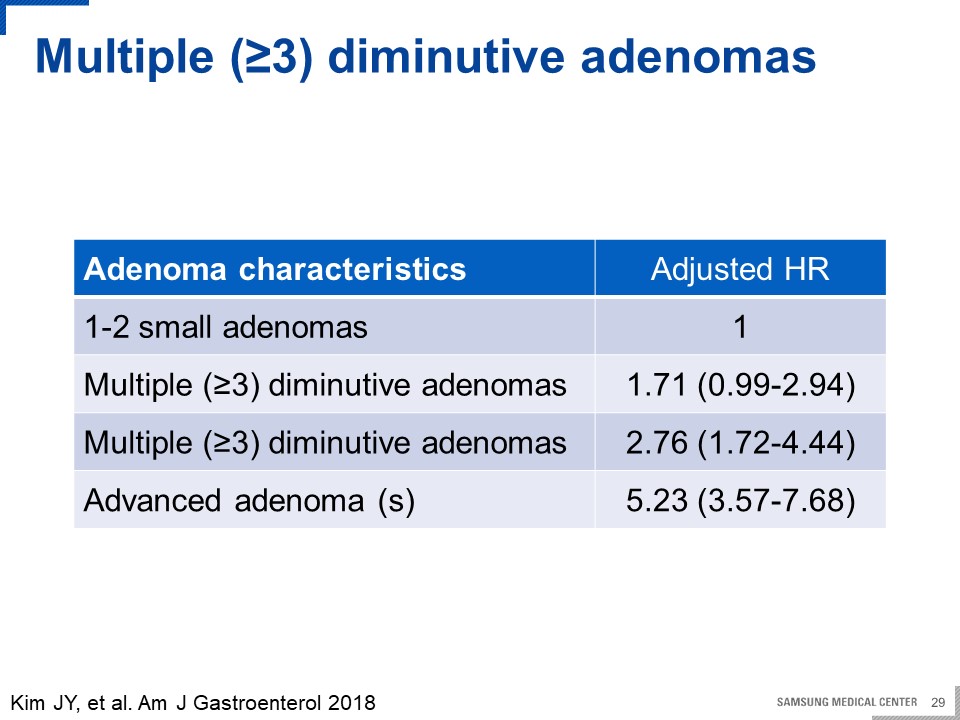
High risk group의 대해서도 몇 가지 풀리지 않은 이슈가 있습니다. 내시경 화질이 좋아지면서 5mm 이하의 매우 작은 용종 발견율이 증가하였고 이로 인해 선종발견율이 높아졌습니다. 따라서 다수의 5mm 이하 작은 선종들"도 정말 high risk에 해당하는지 의문입니다.
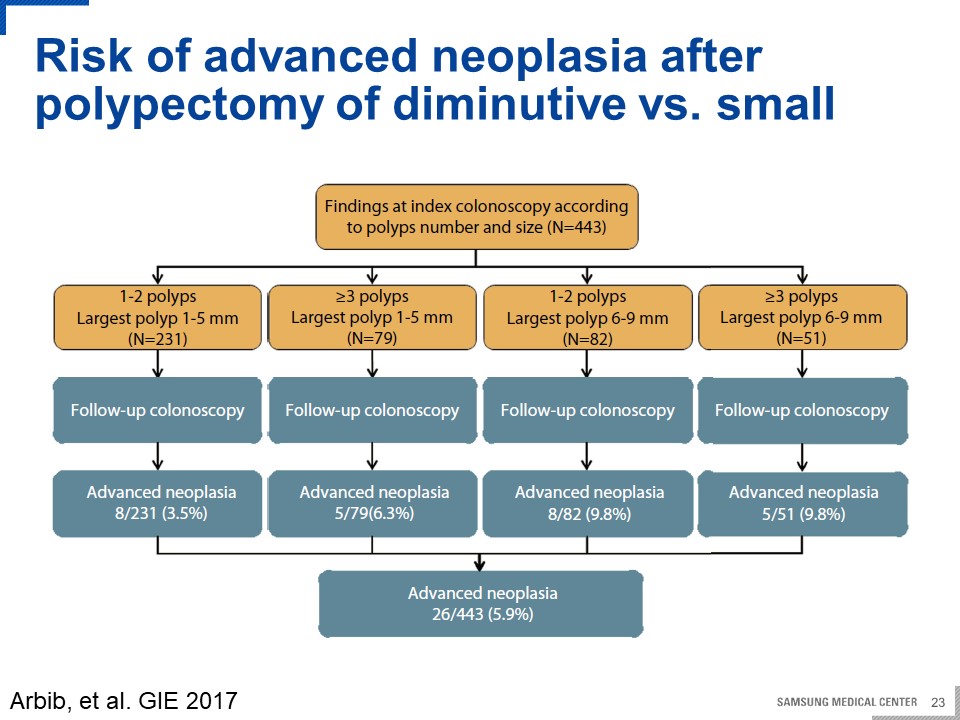
Multiple diminutive adenoma에 대한 연구를 시행하였는데 screening colonoscopy에서 한 개 이상의 선종을 제거한 사람들을 대상으로 분석을 하였습니다. 가이드라인대로 1-2 작은 선종을 가진 환자들을 low risk group으로 구분하고 high risk group은 다음과 같이 3개의 그룹을 세분화 하였습니다. 크기가 3개 이상이지만 diminutive non-advanced adenoma인 경우, 크기가 6-9mm의 small non-advanced adenoma경우, advanced adenoma인 경우로 나누어 surveillance colonoscopy에서의 advanced neoplasia의 발생을 비교하였습니다. 당연히 1-2개의 작은 선종을 가진 low risk group에서 발생이 가장 작았고 diminutive, small, advanced adenoma순으로 발생이 증가하였습니다.
고령이 위험인자입니다.
남성이 위험인자입니다.
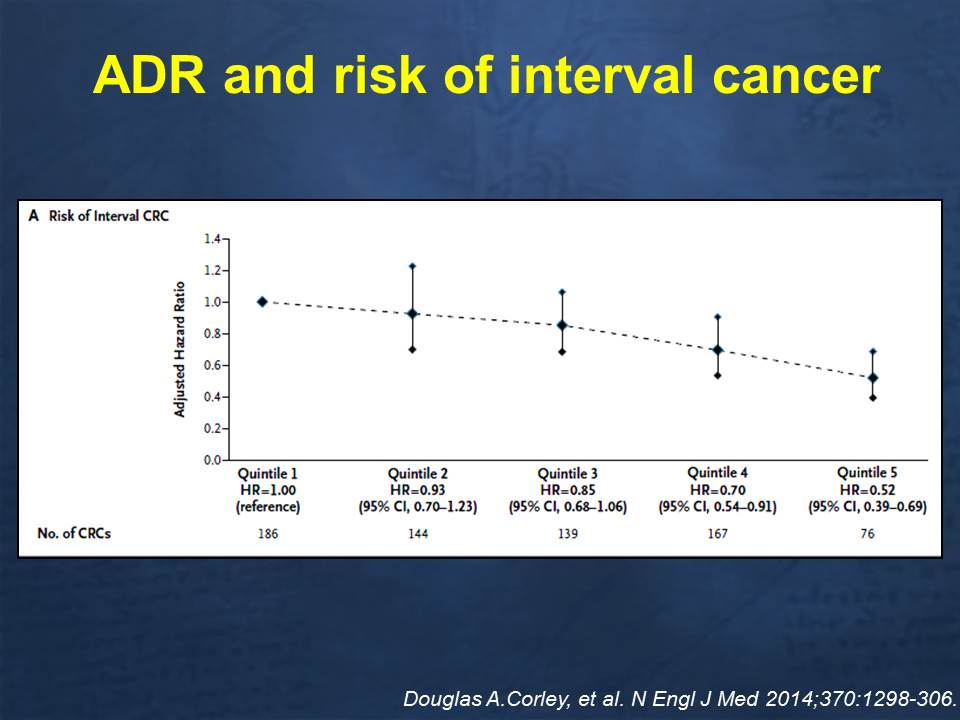
검사를 시행한 의사의 adenoma detection rate도 중요합니다. 낮은 ADR을 가진 내시경의사에게 screening을 받게 되면 높은 ADR을 가진 내시경 의사에게 받는 것보다 metachronous advanced neoplasia의 위험도가 높습니다. 따라서 low-risk adenoma를 가진 사람이 양질의 대장내시경을 시행받았다면 interval cancer의 위험은 높지 않습니다.
한 검진센터의 adenoma detection rate입니다.
김태준 교수님의 멋진 강의의 멋진 summary입니다.
![]() [References]
[References]
3) EndoTODAY 대장용종절제술 후 추적검사 Postpolypectomy surveillance
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.