EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Cowden syndrome. 카우덴 증후군, 코든 증후군, 코우덴 증후군] - 終
[Cowden syndrome. 카우덴 증후군, 코든 증후군, 코우덴 증후군] - 終

2. 유전자 변이
4. 내시경 소견
6. 코드와 산정특례
7. References
![]() 1. Cowden syndrome이란?
1. Cowden syndrome이란?
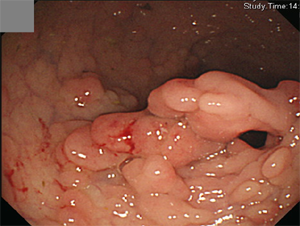
위내시경 소견입니다. 진단은 무엇이겠습니까?
.
.
힌트입니다. 위의 용종증인데 식도에는 glycogen acanthosis가 현저하였습니다. 40대 후반임에도 불구하고... 진단은 무엇이겠습니까?
.
.
두번째 힌트입니다. 대장에는 polyposis가 있었는데 대두분 inflammatory polyp었고 일부만 adenomatous polyp이었습니다.
.
.
세번째 힌트입니다. 유방 수술과, 자궁 수술과, 갑상선 수술의 병력도 있었습니다.
.
.
그렇습니다. Cowden 증후군입니다.
Cowden syndrome 카우덴 증후군은 EndoTODAY와 인연이 깊습니다. 2010년 EndoTODAY를 mobile version으로 개편할 때 첫 mobile format EndoTODAY 증례가 Cowden syndrome이었습니다.
Cowden syndrome은 환자 이름을 딴 질병명입니다. 처음 기술된 환자가 Cowden 씨였습니다 (Lloyd KM. Ann Intern Med 1963). Cowden syndrome은 피부, 구강 점막의 병변을 특징으로 하고 소화관에 polyposis를 일으킵니다. 여러 장기에 hamartoma를 동반합니다. 혈관질환이나 피부질환을 가진 분이 뒤늦게 Cowden syndrome으로 진단되고 놀라서 큰 병원을 찾는 경우가 있습니다.
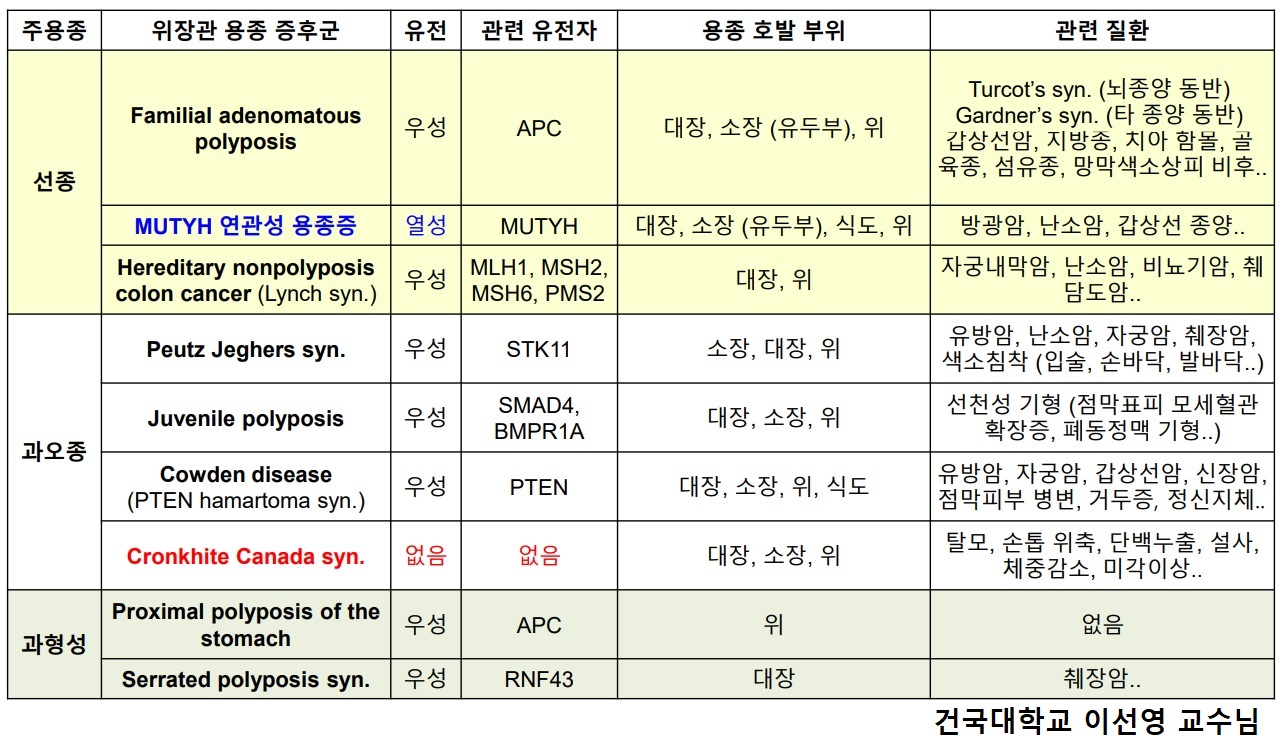
카우덴 증후군은 10q23에 위치하는 종양억제유전자 PTEN 돌연변이에 의해 발생하는 PTEN 과오종 증후군 중 하나입니다. 약 절반은 부모로부터 상염색체 우성으로 물려받고 약 절반은 가족력이 없습니다. 다발성 안면 털종(facial trichilemmona), 유두종성 구진(papillomatous papule), 말단 각화증(acral keratosis)과 같은 피부점막병소를 가지는 경우가 많다. 안면 털종은 모낭의 outer root sheath에 발생하는 양성 과오종 병변으로, 천천히 자라고 피부색과 비슷하며 직경은 1-5 mm이고 얼굴과 목의 헤어라인 근처에서 잘 발견됩니다.
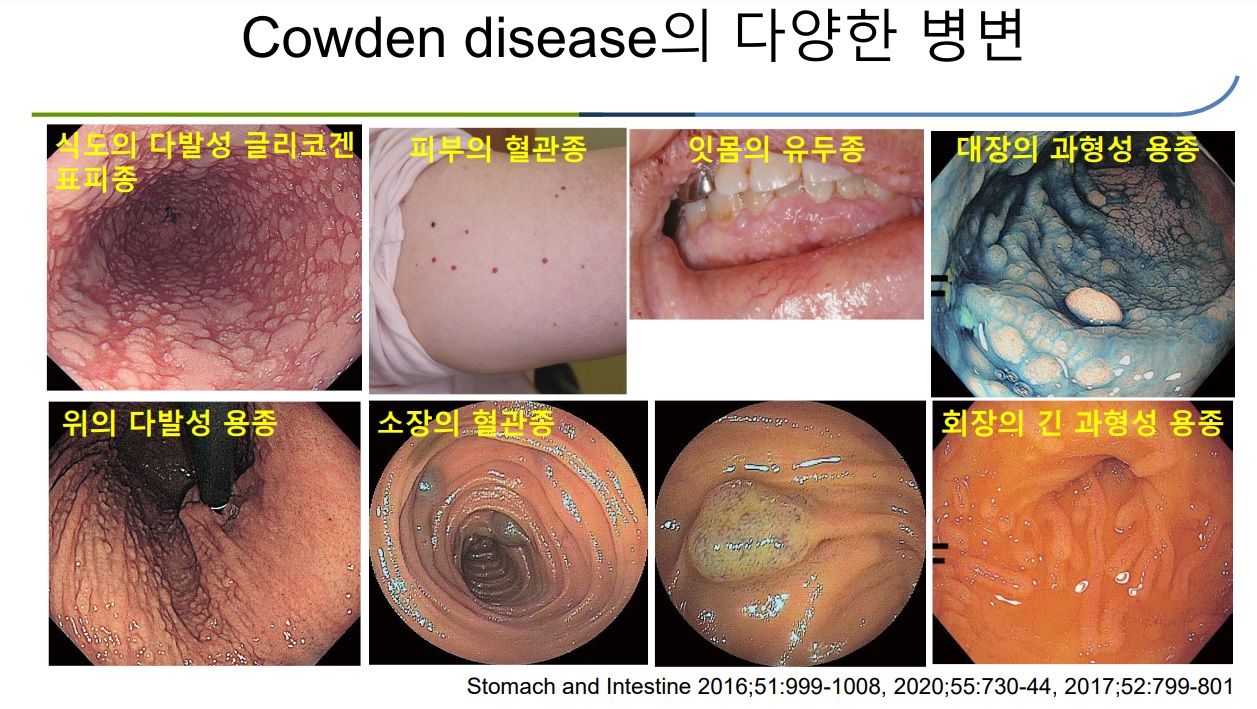
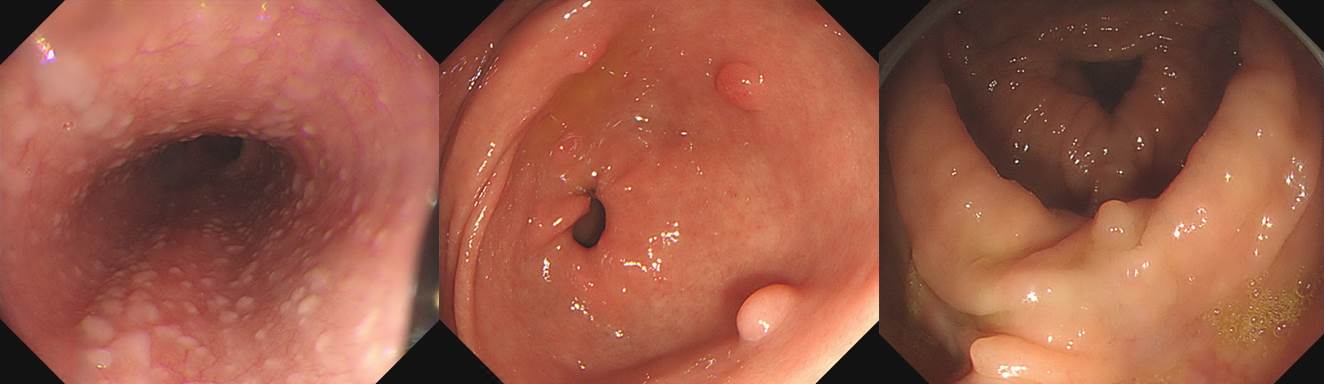
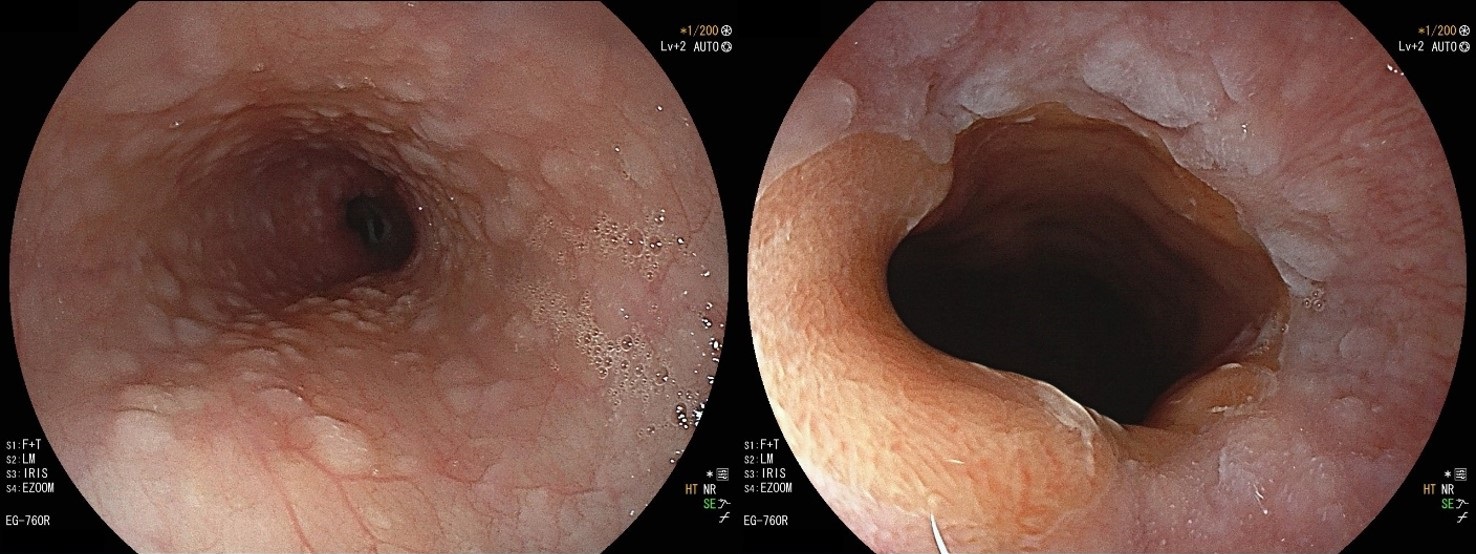
위장관 용종은 식도에서 대장까지 어디에나 가능하며 크기는 1 mm에서 수 cm까지 다양하나 대개 크지 않고 주위 점막과 동일한 색조를 보이며 밀집되어 나타나는 과용종입니다. 가족성 유전성 용종증 (familial adenomatous polyposis, FAP)에서 보이는 비교적 균일한 선종성 용종과는 확연히 구분됩니다. 식도 병소는 글리코젠 가시세포증입니다. 글리코젠 가시세포종은 고령에서 흔히 발견되는데, 비교적 젊은 환자에서 심한 클리코젠 가시세포종이 발견되면 카우덴 증후군을 고려해야 합니다.
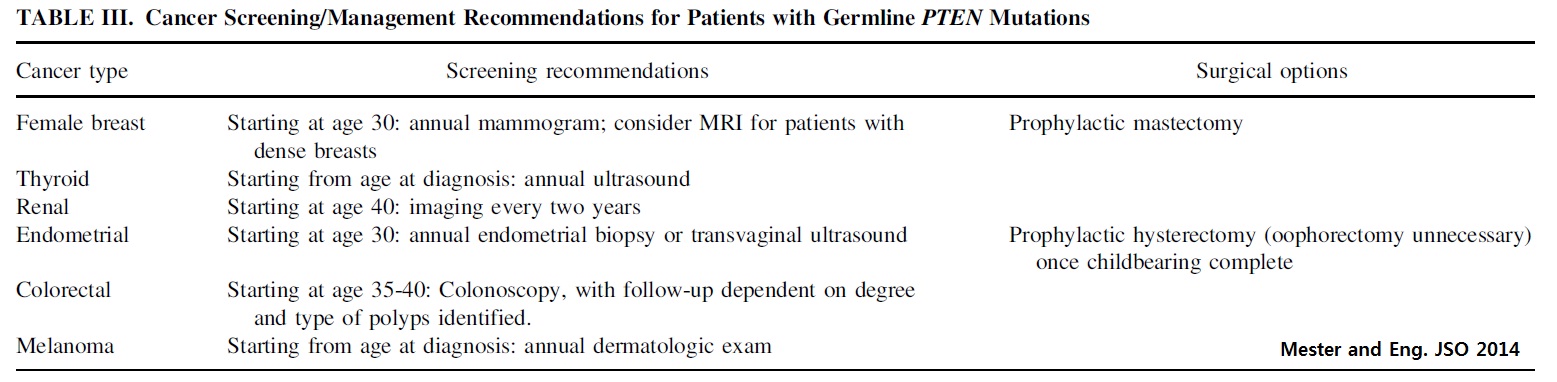
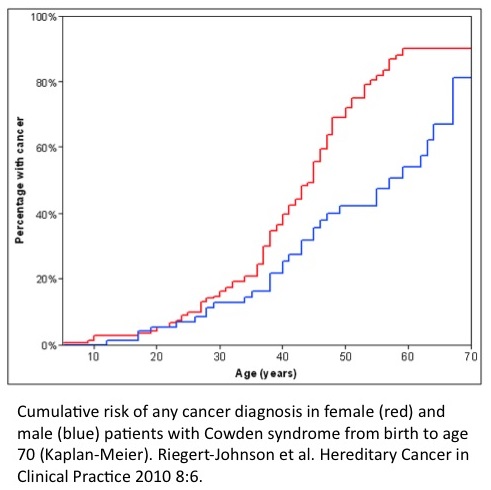
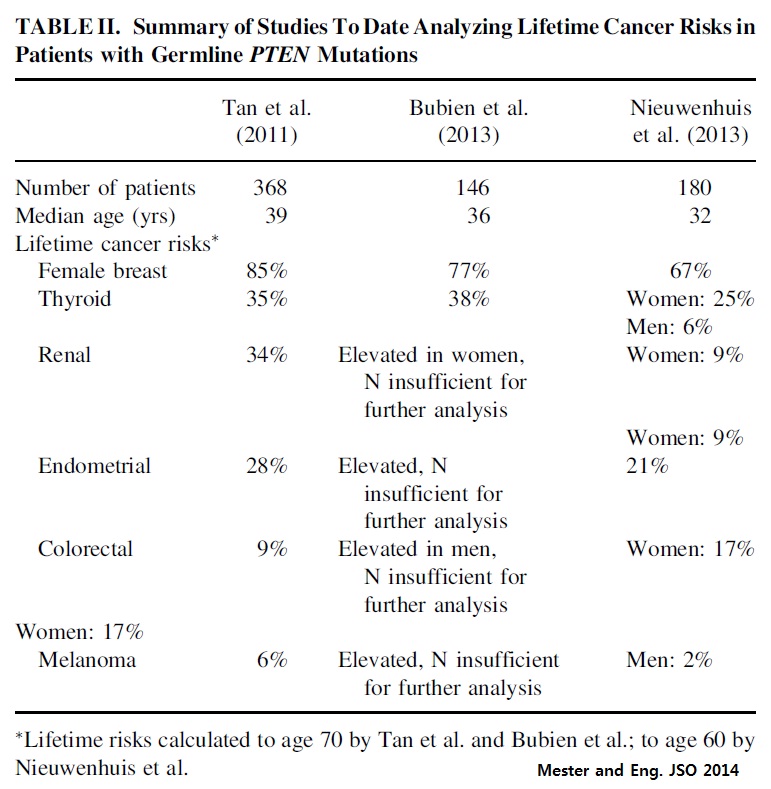
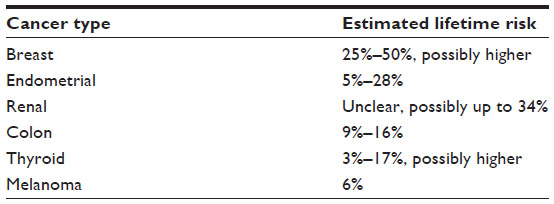
카우덴 증후군은 다발성 암 증후군의 하나이며 유방암, 갑상선암, 자궁내막암, 대장직장암, 신장암 및 위암의 위험이 높습니다. 일반적인 검진보다 훨씬 짧은 간격으로 많은 장기에 대한 검진이 필요합니다.
Cowden syndrome is a hereditary condition which causes multiple types of benign tissue overgrowth (called hamartomas) and a risk of breast, thyroid, and uterine cancers. The most consistent features of CS are small flesh-colored bumps on the skin involving a hair follicle (trichilemmomas) and small wart-like growths (papillomatous papules) on the face, hands and mouth. CS is also often associated with a large head size (macrocephaly) and hamartomatous polyps of the small and large intestine. Thyroid adenomas, goiter, and nodules are also seen at increased frequency. Women are at increased risk for benign breast conditions, such as ductal hyperplasia, papillomatosis, fibrocystic breast disease, or fibroadenomas. Less commonly seen are benign fatty tumors (lipomas), blood vessel growths (hemangiomas), and other changes. (University of Iowa)
Cowden syndrome과 비슷한 몇 개의 질병명이 있는데 모두 PTEN 유전자 이상과 관련되어 있어서 최근에는 한 질환의 다른 spectrum으로 보는 경향이 있습니다. PTEN harmatoma tumor syndrome으로 부릅니다. 그 임상적 특징은 아래와 같습니다.
서양 자료여서 그런지 위암에 대한 언급이 없습니다. 그러나 Cowden 증후군에서 위암 발생률이 다소 높습니다.
Non-malignant features of Cowden syndrome
Cowden syndrome에 대한 최근 리뷰를 소개합니다. 제목이 Cowden syndrome: Recognizing and managing a not-so-rare hereditary cancer syndrome입니다. 드물기는 한데 그렇다고 아주 드물지도 않은 질환입니다.
약 절반은 부모로부터 물려받고 약 절반은 sporadic입니다. Autosomal dominant로 유전되므로 자녀의 절반도 같은 질환을 가집니다. 따라서 유전학적 검사와 상담, 그리고 가족에 대한 screening이 필요합니다.
소화기내과 의사인 필자는 Cowden syndrome의 암발생 위험에 관심을 가지고 있지만 암 이외에도 아래와 같은 신경, 피부 질환 등이 Cowden syndrome의 중요 특징입니다.
- Macrocephaly (larger-than-average head size)
- Trichilemmomas (benign skin lesions, skin tags) and papillomatous papules (raised areas on the skin)
- Learning disabilities and/or autism
- Development of lipomas (benign tumors of fatty tissue), intestinal polyps, and uterine fibroids (benign tumors of the uterus)
trichilemmomas

2021년 10월 이선영 교수님 교육자료
Cowden 환자 관리의 핵심은 암검진입니다. 상세한 내용은 아래를 참고하시기 바랍니다. 위암이 빠졌는데요, Cowden 증후군에서 위암도 약간 많이 발생한다고 알려져 있습니다. 위내시경을 1년에 한번 하도록 권하고 있습니다.
일본 책에 나온 사진입니다.
![]() 2. 유전자 변이
2. 유전자 변이
PTEN is a tumor suppressor gene located on chromosome 10q23.3. It encodes a phosphatase that influences the cell cycle, causing G1 arrest and apoptosis.
[Cowden syndrome이 의심되는데 유전자 변이가 확인되지 않으면?]
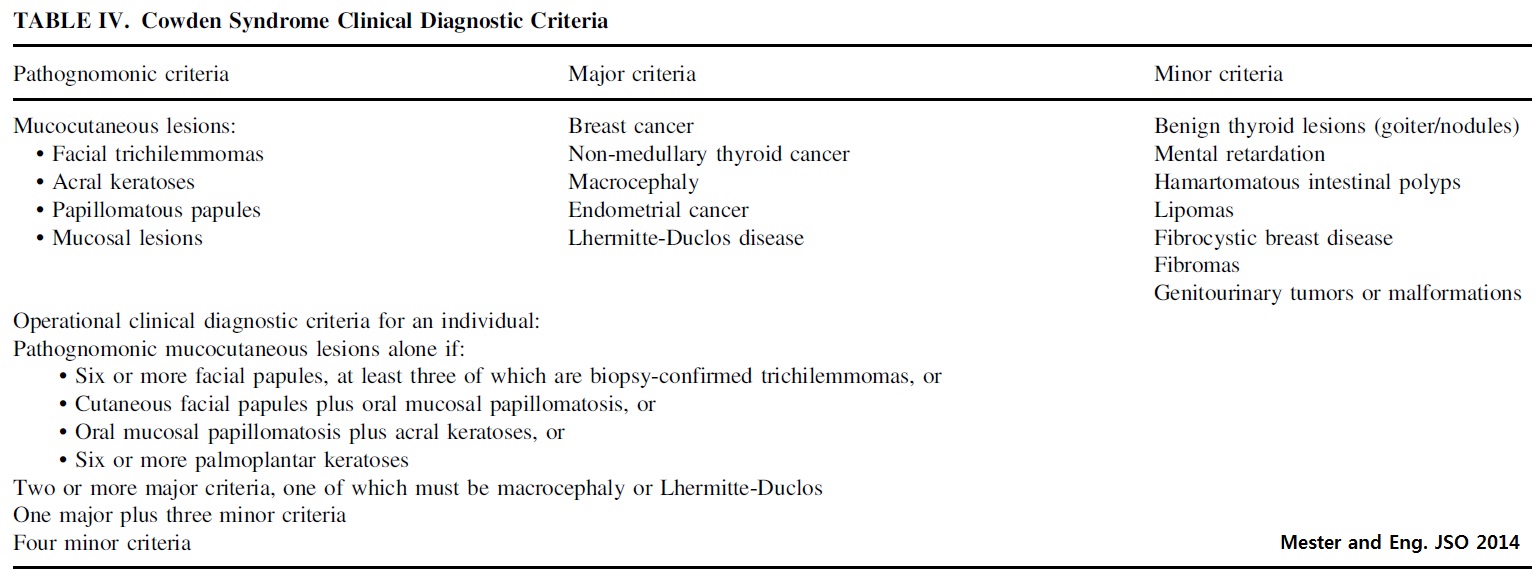
PTEN 유전자 검사를 하면 대부분 이상이 확인됩니다. 간혹 PTEN 유전자 변이가 확인되지 않더라도 아래와 같은 임상적 특성이 있으면 Cowden syndrome에 준하여 관리하면 됩니다.
![]() 3. 악성질환 screening
3. 악성질환 screening
Cowden syndrome에서는 다양한 악성질환이 발생할 수 있습니다.
Cowden syndrome 환자에서 발생한 신장암
Cowden syndrome 환자 관리의 핵심은 다양한 암에 대한 검진과 적절한
Cowden syndrome 환자의 악성질환 조기진단을 위한 검진 지침입니다.
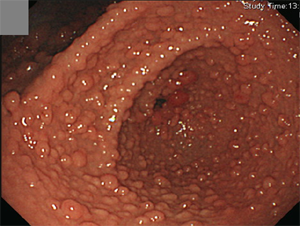
![]() 4. 내시경 소견
4. 내시경 소견
[증례 1]
2010년 9월 9일 EndoTODAY를 모바일로 개편한 후 첫 자료가 Cowden's disease (EndoTODAY 20100909)였습니다. 아래에 옮깁니다.
용종증(polyposis)는 선종성 용종증과 비선종성 용종증으로 나누어집니다. 비선종성 용종증의 대표는 그 유명한 Peutz-Jeghers syndrome이지요. Cowden’s disease, Bannayan-Ruvalcabe-Riley syndrome, hereditary mixed polyposis syndrome, intestinal ganglioneuromatosis and neurofibromatosis, Devon family syndrome, Basal cell nevus syndrome등도 모두 비선종성 용종증입니다.
40대 여성이 최근 발견된 위와 장의 nonadenomatous polyposis로 의뢰되었습니다. 환자는 갑상선암, 유방암, 자궁암으로 수술받은 과거력이 있었습니다. 얼굴과 목에 태어날 때부터 쥐젖이 있었다고 하며, 손발에 물집양 병변이 있었습니다. 이 모든 소견은 PTEN 유전자의 돌연변이에 의한 autosomal dominant 질환인 Cowden's disease에 합당한 소견입니다. 위에는 매우 많은 sessile polyp이 있었으며 조직검사는 hyperplastic polyp으로 보고되었습니다.
PTEN 유전자의 돌연변이가 발견되었습니다. PTEN 유전자 5번째 exon에서 395번째 염기서열이 G에서 A로 치환됨에 따라 129번째 아미노산이 Gly에서 Arg으로 바뀌는 missense variation이 발견된 것입니다.
이 환자의 대장내시경에서 매우 많은 용종이 발견되었습니다. 조직검사는 inflammatory fibrinoid polyp으로 보고되었습니다. 위와 달리 대장 용종들은 크기 차이가 심했는데 이 점이 일반적인 소견인지 아니면 이 환자의 특별한 소견인지 저도 잘 모릅니다.
[증례 2]
Gastric hamartomatoous polyps
Colonic inflammatory polyps
[증례 3] 유전학적 confirm은 되지 않음.
Gastroduodenal hamartomatous polyposis
Cowden syndrome을 의심할 수 있는 좋은 hint 중 하나는 유난히 심한 식도 glycogen acanthosis입니다.
위장관의 다양한 hamartomatous polyp에 대해서는 Gastric Hamartomatous Polyps - Review and Update (Clin Med Insights Gastroenterol 2016)를 참고하시기 바랍니다. 문헌 중 Cowden syndrome 부분을 옮깁니다.
The incidence of CS (Cowden syndrome) in the general population is 1 in 200,000 and more than 90% patients present in the adult life by the late third decade. Mucocutaneous hamartomas (trichilemmomas, acral keratosis, and papillomatous lesions) are pathognomonic features of CS. Macrocephaly and Lhermitte?Duclos disease or dysplastic cerebellar gangliocytoma are two other features considered specific for CS and are included in the major criteria.
These patients have an increased risk of breast, thyroid, and endometrial carcinoma, which are the other major criteria. Patients with CS also have a predisposition to benign hamartomatous outgrowths such as lipomas, arteriovenous malformations, fibrocystic breast disease, benign thyroid nodules, multiple uterine leiomyomas (fibroids) and/or bicornuate uterus, and gastrointestinal polyps. Diffuse esophageal glycogenic acanthosis is present in more than 80% of CS patients and may be diagnostic for CS in the presence of other benign gastrointestinal polyposis.
Gastrointestinal polyps occur in up to 50% of patients with CS with a wide variety of endoscopic and histologic features, including adenomatous, inflammatory, hyperplastic, lymphoid, ganglioneuromatous, and leiomyomatous polyps. The majority of CS patients (>50%) have two or more different polyp histologies. Though most studies describe polyps in CS being colonic, gastric polyps are present in almost all patients with CS and are usually numerous with a variable appearance. Depending on the major histologic component, they can be smooth contoured or have a hyperplastic/papillary configuration endoscopically. The polyps in the stomach are commonly misdiagnosed as hyperplastic hamartomatous polyps. Though dysplasia has not been reported in gastric polyps in CS, patients with CS and gastric cancer have been reported. The risk of colorectal carcinoma in CS is 7%?15%, and 1 in 100 patients with CS may develop gastric malignancy.
Individuals with multiple gastrointestinal hamartomas or ganglioneuromas should be evaluated for PTEN gene mutation. The recommended gastrointestinal surveillance for patients with PTEN gene mutation is colonoscopy and esophagogastroduodenoscopy examination beginning at the age of 15 years and repeated every two years or two to three years, though different suggestions has been suggested.
![]() 5. Vascular abnormality
5. Vascular abnormality
AVMs and haemangiomas are not widely recognised features of Cowden syndrome.
Imaging of the gluteal arteriovenous malformation (AVM) in case 1. All views are in anterior-posterior orientation. (A) Angiogram of the distal aorta and iliac vessels showing the dilated left common iliac and left internal iliac arteries. (B) Computed tomographic angiogram showing a large AVM arising from the left superior gluteal artery and extending through the sciatic notch into the left buttock. (C) A reconstructed rendered surface angiogram showing the AVM arising from the left superior gluteal artery. (J Med Genetics 42(8))
Vascular anomalies in patients with a PTEN mutation are typically multifocal intramuscular combinations of fast-flow channels and ectopic fat. Cerebral DVAs (developmental venous anolamies) are very common. PTEN mutational analysis should be considered for all macrocephalic patients with fast-flow vascular anomalies or multiple intracranial DVAs. (Tan WH. J Med Genet 2007)
(A) Dural arteriovenous (AV) fistula (patient 23); (B, C) gadolinium-enhanced T1-weighted MRI of the brain showing developmental venous anomalies (arrows). (D, E) Aangiography of (D) patient 11 with paraspinal and (E) patient 15 with right lower limb arteriolovenous malformations, showing disproportionate venous ectasia, typical of PTEN lesions. (Tan WH. J Med Genet 2007)
Monitoring for vascular anomalies is not currently part of the “standard of care” for these patients.
![]() 6. 코드와 산정특례
6. 코드와 산정특례
2016년 7월 1일 희귀질환 산정특례 고시
Cowden syndrome은 Q85.84 코드로 산정특례 대상입니다.
![]() [FAQ]
[FAQ]
[2022-7-22. 애독자 질문]
Cowden 환자와 Cronkhite-Canada syndrome 환자, juvenile polyposis, FAP 등의 polyposis 환자들은 pathology로만으로도 진단이 가능한 것인지, 임상증상을 종합해서 보는 것인지 헷갈리는 것 같습니다. FAP 환자는 100개이상의 선종이 나오는 것으로 진단하고, Cowden 환자는 식도 achanthosis 가 있고 조직검사 상 과오종 등으로 나오고 Cronkhite canada syndrome 환자는 낭포상 선관확장으로 진단하는데 juvenile polyposis하고는 내시경적 소견을 구분하는 것이 맞는지 궁금합니다.
[2022-7-22. 이준행 답변]
좋은 질문입니다. 내시경 소견에 약간의 차이가 없는 것은 아니지만 진단에 사용할 정도로 specific한 것은 아닙니다. FAP는 adenomatous polyposis이므로 병리로 구분되겠으나 다른 종류는 조직학적 차이도 specific하지 않습니다. 임상상의 차이와 유전학적인 검사를 모두 고려한다고 보는 것이 좋겠습니다.
![]() [References]
[References]
2) PTEN 유전자 정보
3) 영문 환자 정보
- MD Anderson Cancer Research Center (PDF)
- cancer.net
- University of Iowa4) 용종증 폴립증후군 polyposis syndrome - 내시경세미나 강의록. 임종필. PDF 0.7M
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng