EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [연세대학교 의과대학 소화기학 연수강좌]
[연세대학교 의과대학 소화기학 연수강좌]
2015년 10월 11일 일요일 연세대 소화기내과에서 주최한 소화기학 연수강좌에 환자안전 강의차 다녀왔습니다 (2015년 10월 11일 연세대학교 에비슨의생명연구센터 유일한 홀). 일본 JDDW에서 돌아와 바로 연세대에서 강의를 하려니 조금 벅차긴 했지만... 준비된 발표들이 알차서 좋은 시간이었습니다.

![]() 1. 비만과 대사성 질환의 내시경 치료 - 연세대학교 신성관
1. 비만과 대사성 질환의 내시경 치료 - 연세대학교 신성관
비만은 보기 싫은 상태가 아니라 질병입니다. 서양인에 비하여 동양인에서는 동일 BMI에서 체지방률이 높고 비만관련 질환도 많기 때문에 서양보다 다소 tight한 진단기준을 적용해야 합니다.
비만 관련하여 위를 수술하면 체중감소효과만 있지만 소장을 수술하면 체중이 빠질뿐만 아니라 당뇨관련 여러 지표가 개선됩니다. 아직까지 잘 알려지지 않은 기준이 있을 것입니다. 체중감소 시술 후 당뇨가 좋아지는 기전 중 하나로 incretin 이라는 호르몬의 역할이 주목받고 있습니다. 예상치 못한 다른 기전들도 연구되고 있습니다.
 대한임상소화기내과 2015;2(3)
대한임상소화기내과 2015;2(3)
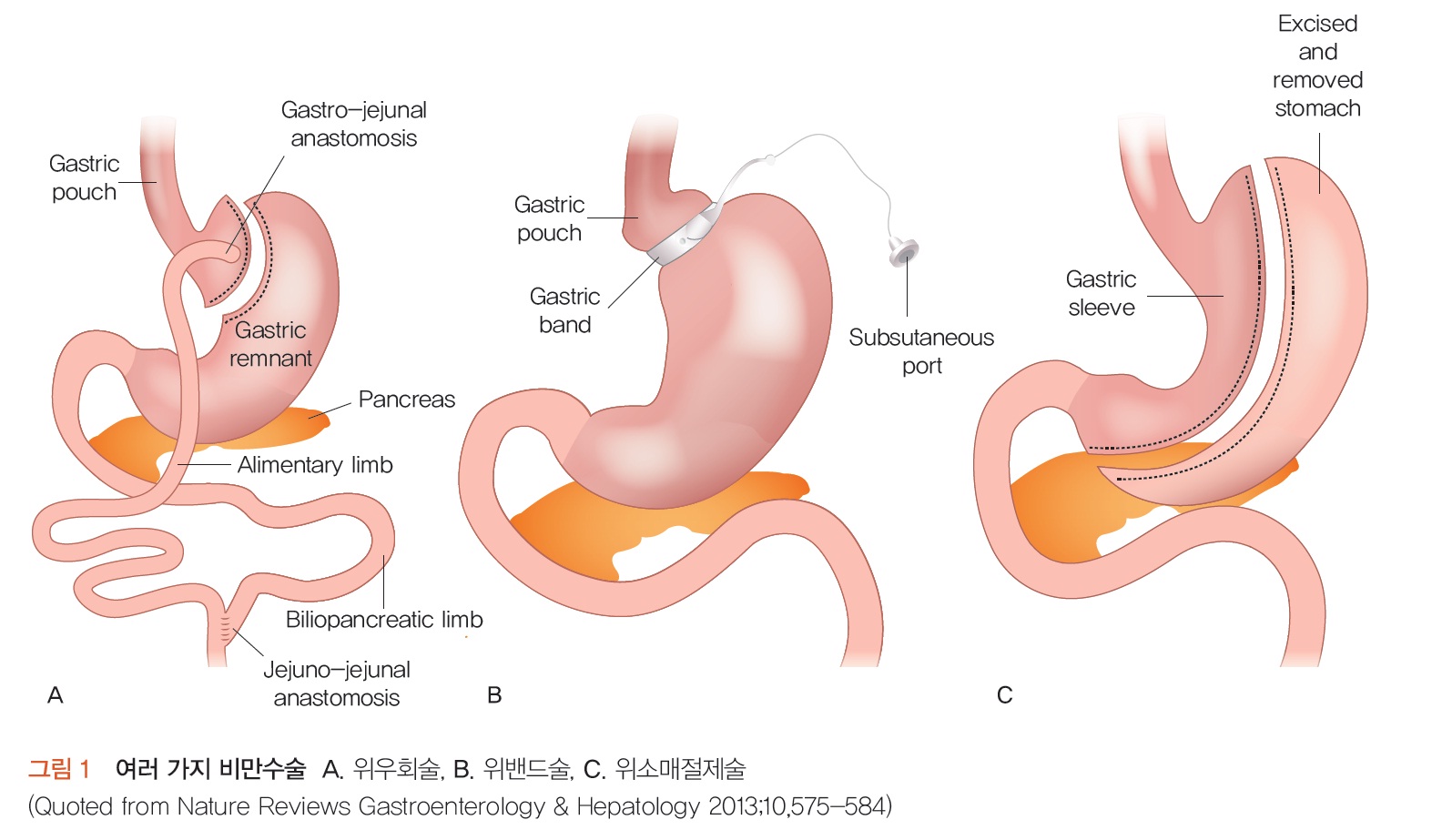
1) 위에 시술하는 방법
(1) Apollo overstich를 이용한 sleeve gastrectomy
(2) Incisionless operating plateform

(3) Aspiration therapy: PEG와 비슷한 원리로 음식을 먹고 PEG tube를 통해 음식을 뽑아내는 방법.
2) 소장에 시술하는 방법
(1) Duodenal sleeve
(2) Duodenal mucosal resurfacing
* 참고: EndoTODAY 비만
![]() 2. 대장암 예방과 조기 진단 - 연세대학교 이현정
2. 대장암 예방과 조기 진단 - 연세대학교 이현정
우리나라에서 대장암은 남자의 경우 매년 6.1%, 여자의 경우 매년 4.5% 증가하고 있습니다.
전체 대장암 환자의 약 5-15%는 유전적 요인에 의해 발생하며, 비교적 잘 밝혀진 유전성 대장암은 전체 대장암의 약 5%를 차지합니다. 예를 들어 가족성선종성용종증 (FAP, 1%), 유전성 비용종증 대장암 (2-3 %), 포이츠-제거스 증후군, 연소기 용종증, MYH 용종증 등이 있습니다.
MUTYH-associated polyposis (MAP)는 익숙하지 않은 질환인지라 아래에 간단히 소개합니다.
MUTYH-associated colorectal cancer and adenomatous polyposis (Surg Today 2014)
MUTYH-associated polyposis (MAP) was first described in 2002. MUTYH is a component of a base excision repair system that protects the genomic information from oxidative damage. When the MUTYH gene product is impaired by bi-allelic germline mutation, it leads to the mutation of cancer-related genes, such as the APC and/or the KRAS genes, via G to T transversion. MAP is a hereditary colorectal cancer syndrome inherited in an autosomal-recessive fashion. The clinical features of MAP include the presence of 10-100 adenomatous polyps in the colon, and early onset of colorectal cancer. Ethnic and geographical differences in the pattern of the MUTYH gene mutations have been suggested. In Caucasian patients, c.536A>G (Y179C) and c.1187G>A (G396D) mutations are frequently detected. In the Asian population, Y179C and G396D are uncommon, whereas other variants are suggested to be the major causes of MAP.
ASCO recommends the following screening for people with MAP. It is important to discuss these options with your doctor, as each individual is different:
- Colonoscopy every one to two years, beginning at age 18 to 20.
- Yearly colonoscopy once a person develops polyps. Colectomy is the surgical removal of the entire colon. This may be considered if polyps cannot be managed with regular colonoscopies because there are too many.
- Upper endoscopy (EGD) at age 25 to 30 or once colorectal polyps are detected, whichever occurs first
- Yearly ultrasound of the thyroid may be considered starting at age 25 to 30
- Computed tomography (CT) scan or magnetic resonance imaging (MRI) if a person has a family history of desmoid tumors and a mutation on the APC gene that is linked with these tumors
2004년부터 2008년까지 우리나라에서 시행한 국가암검진 대변잠혈검사의 양성률은 7.28%였습니다. 저는 이런 질문을 했습니다.
우리나라에서는 이상하게도 대장내시경을 받은 사람도 걸러지지 않고 매년 stool occult blood로 건진을 받으라는 쪽지를 받고 있습니다. 정부의 무책임한 건진 정책으로 인하여 작년에 대장내시경을 받은 사람이 올해에도 stool occult blood 양성으로 대장내시경을 받으라는 권유를 받고 오시는 분이 제법 많습니다. 어떻게 하시는지요?
차재명 교수님께서 최근 Am J Gastroenterol에 이에 대한 답변이 있었다고 comment 해 주셨습니다 (아래 초록 참조). 대장내시경 후 stool occult blood 가 양성이라도 interval cancer는 거의 없다고 합니다. 제 걱정은 일단 대변에서 피가 나왔다고 오신 분에게 '위험이 낮으니 그녕 가세요'라고 말하며 되돌려보내기는 어려울 것 같다는 것입니다. 불필요한 검사는 안하는 것이 상책일 것 같습니다.
Results: The mean age (68.9±9.6 years), sex (95.2% male), and race (48.1% white, 32.1% black, 15.6% Hispanic, and 4.2% other) did not differ between the four groups. Overall, adenomas of any size were detected in 42.8% of patients, adenomas >= 10 mm in 14.7%, advanced neoplasms in 20.7%, and cancers in 7.3%. Advanced neoplasms were detected in 30.4% of patients who have never had a colonoscopy, 27% in those who have had one greater than 10 years prior, 10.0% in 5-10 years prior, and 1.1% in less than 5 years prior.
Conclusions: In asymptomatic average-risk patients with a negative colonoscopy within the last 5 years, the prevalence of adenomas is low, and no patient was diagnosed with cancer. These findings support the CDC recommendations to suspend annual FOBT for up to 5 years after a negative colonoscopy.
대장내시경 후 추적검사에 대해서는 다음 link를 참고하기 바랍니다. colon_cancer_004.html
[2017-2-4. 이준행 추가] 대장내시경 검사 후 stool occult blood test는 필요하지 않다는 것이 중론입니다. 그러나 미디어에서는 '5.5.1 법칙'이 소개되고 있습니다. 엉터리도 이런 엉터리가 없다는 생각입니다.
![]() 3. 간암 예방 및 조기 간암 발견 - 연세대학교 김도영
3. 간암 예방 및 조기 간암 발견 - 연세대학교 김도영
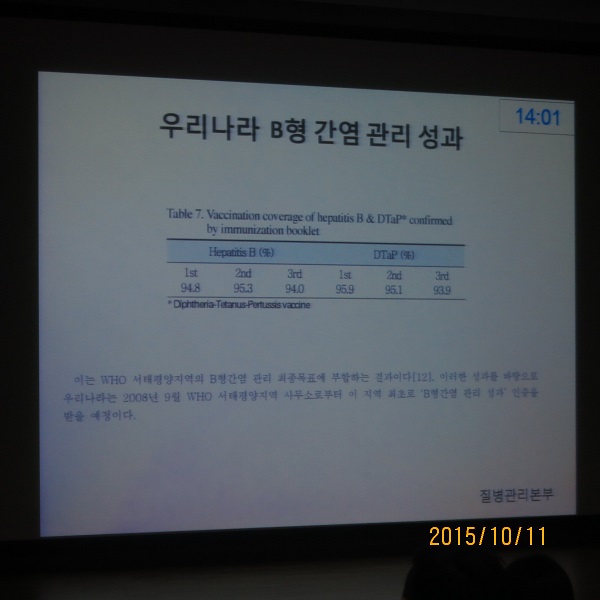
우리나라는 간염 관리를 잘 하고 있는 나라로 국제적으로 창찬을 받고 있다는 말씀을 하셨습니다.
Antiviral therapy clearly reduces HCC incidence. 항바이러스 초치료에 실패하면 약을 바꿔서 치료를 지속해야 한다고 합니다.
간암 조기진단을 위하여 ultrasonography alone은 부족하다고 합니다. Within Milan이 63%라고 합니다. 즉 간이식을 시도할 수 있는 단계를 넘는 사람이 1/3입니다. AFP를 더해도 민감도는 69% 정도입니다.
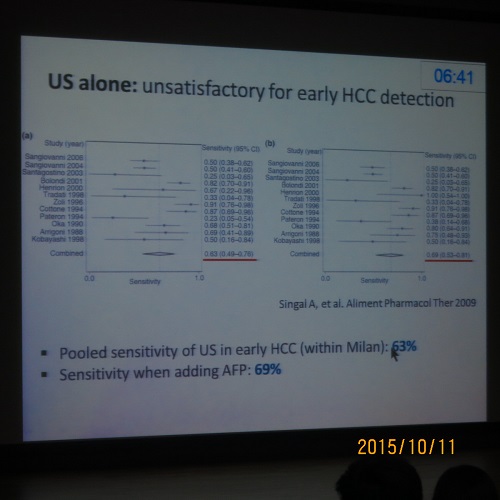
Alpha FP (AFP) 이외의 좋은 marker는 아직 없습니다. DCP, AFP-L3 등이 언급되었지만 세브란스 병원 연구에서는 negative data 였습니다 (Lim TS. Scand J Gastroenterol Epub).
Q and A에서 나온 김도영 교수님 답변: C형 간염에 대한 좋은 약들이 많이 나왔습니다. 비록 AST/ALT가 정상이더라도 hepatitis C virus를 가지고 있는 것이 확인된 모든 사람이 항바이러스제 치료 대상이라고 합니다.
![]() 4. 정확한 진정제 사용과 모니터링 - 연세대학교 마취과 유영철
4. 정확한 진정제 사용과 모니터링 - 연세대학교 마취과 유영철
Malampati score가 3 혹은 4 인 경우는 마취과 의사에게 진정을 의뢰하라고 권고됩니다. 3인 환자가 10%, 4인 환자가 1-2%입니다.
유교수님은 진정내시경에서 routine 하게 산소를 주는 것이 필요하다고 주장하셨습니다. 비만, 평소 코를 고는 환자, airway가 안 좋은 환자에서는 특히 산소를 주도록 권했습니다. 진정 전에 5분 정도 산소를 주거나 산소를 이용한 큰 호흡을 몇번 하는 것도 좋다고 제안하였습니다. 고민입니다. 현실적인 어려움이 적지 않기 때문입니다. 번거롭기도 하고, 매번 nasal prong을 바꾸는 것도 불편하고, 검사 진행 속도도 늦어질 것 같고, 의료진이 방심할까 걱정되기도 하고...
![]() 5. 대장내시경 질관리 - 경희대학교 차재명
5. 대장내시경 질관리 - 경희대학교 차재명
차재명 교수님은 씨애틀의 Virginia Mason Medical Center가 적자를 타개하기 위하여 비용절감에 몰두하지 않고 질행상 노력을 해서 흑자전환된 사례를 소개했습니다.
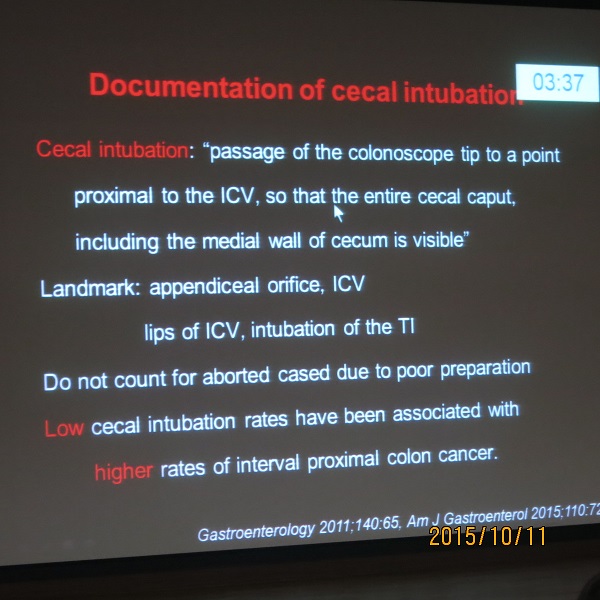
Cecum을 멀리서 잠깐 보았다고 cecal intubation이 된 것으로 간주하면 안됩니다. 기준이 상당히 엄격했습니다 (아래 사진 참조).
대장 정결은 남아있는 물을 모두 제거한 후 평가하는 Boston scale을 권합니다.
![]() 6. 내시경실의 환자안전과 의료진 안전 - 성균관대학교 이준행 (좌장은 연세대학교 박효진 교수님께서 수고해 주셨습니다)
6. 내시경실의 환자안전과 의료진 안전 - 성균관대학교 이준행 (좌장은 연세대학교 박효진 교수님께서 수고해 주셨습니다)
저는 "메르스 때 느끼셨겠지만 안전은 개개인의 노력만으로 이룰 수 있는 그런 일이 아닙니다. 큰 투자와 시스템 개발 및 지속적인 반복 훈련이 전제되어야 합니다. 오늘은 소화기내과 행사라는 점을 고려하여 지금부터 나부터 할 수 있는 일 두 가지를 중심으로 말씀드리겠습니다."로 시작하여 critical value report (CVR)과 ergonomics에 대하여 강의하였습니다.
![]() [References]
[References]
1) 2015년 연세대학교 의과대학 소화기학 연수강좌 - 비만, 대장암 예방과 조기 진단, 간암 예방, 대장내시경 질관리
2) 2016년 연세대학교 의과대학 소화기학 연수강좌 - belching/bloating, hepatitis C
© EndoTODAY Endoscopy Learning Center. Jun Haeng Lee. 일원내시경교실 바른내시경연구소 이준행