EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [2023-12. Random ideas] - 終
[2023-12. Random ideas] - 終
[2023-12-23] 이런 Facebook 광고를 보았습니다. 국정원도 광고를 하네요. [우리는 음지에서 일하고 양지를 지향한다]
[2023-12-22] 일전에 대전을지대에 EndoGEL을 하나 기증한 적이 있습니다. 유익하게 사용했다는 메일이 왔습니다.
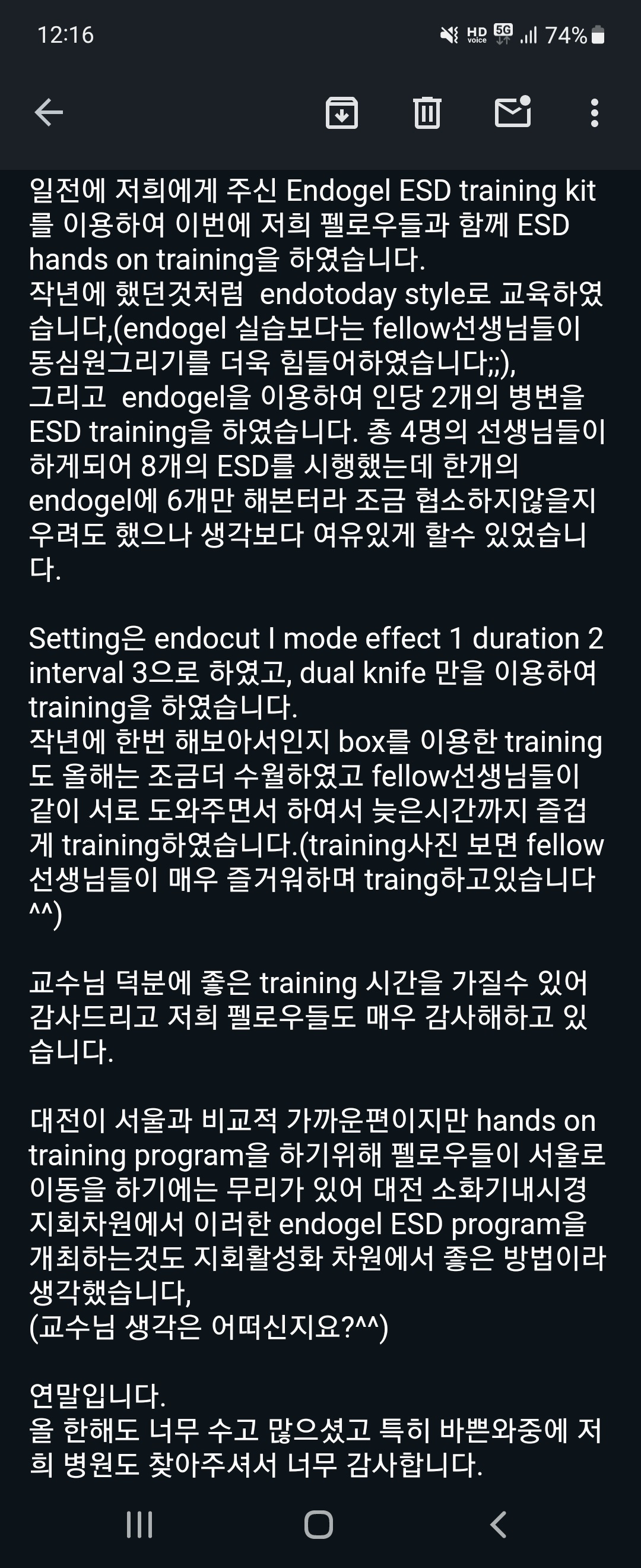
환자용 침대에서 EndoGEL 훈련을 하였으므로 고정이 불충분하여 잡아주느라 고생을 했을 것 같습니다. 내년에는 Koken simulator와 docking station을 준비해 좀 더 우아하게 연습토록 해 주고 싶습니다.
[2023-12-22] 2023-11-23 다학제 집담회 다시보기
[2023-12-22] NCC gastric cancer forum
[2023-12-22] 오래된 기사를 우연히 다시 만났습니다. [병원에 간 태블릿피시, 의사도 환자도 ‘OK’]
[2023-12-21] Dr. Batbileg (Babi) from Mongolia visited my endoscopy training room.
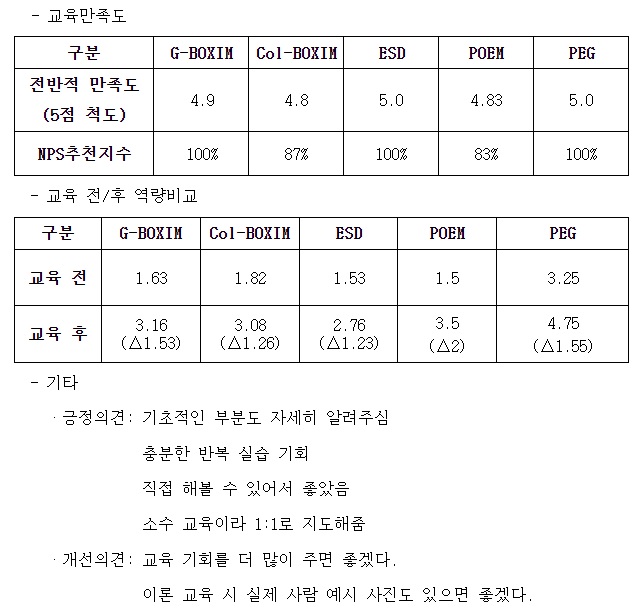
[2023-12-20] 1년간의 내시경 핸즈온 교육 공개강좌의 결과 보고서를 받았습니다. 만족스럽습니다. 더 많이 더 자주 하지 못해서 아쉬울 따름입니다.
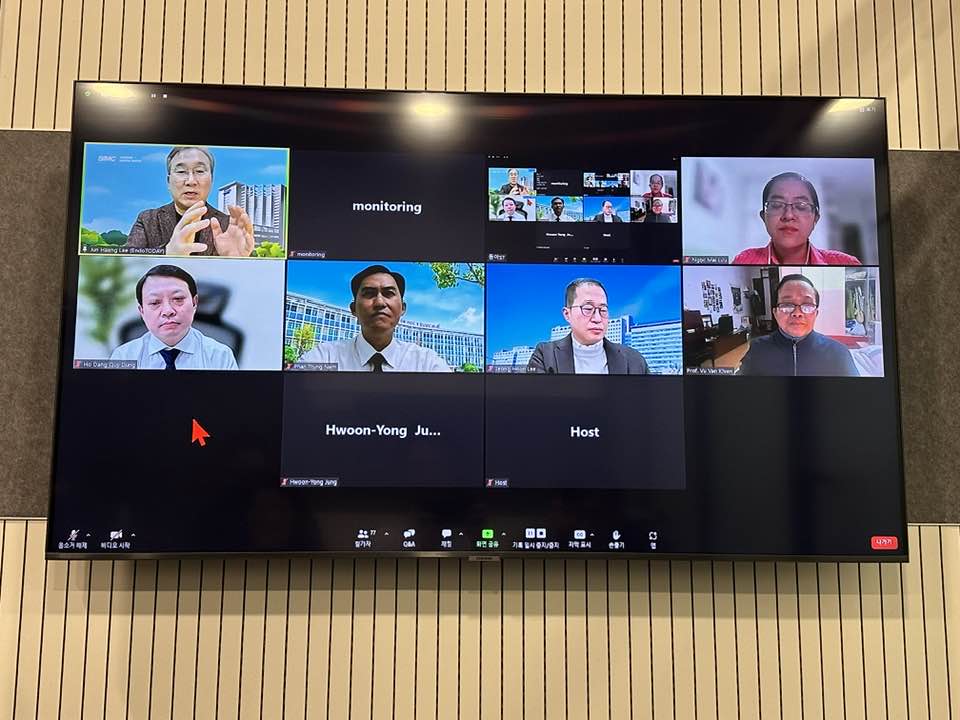
[2023-12-19] Helicobacter 학회에서 베트남과 webinar를 하였고 제가 첫 발표를 하였습니다. 50대 중반에 발표가 벅차기는 합니다.
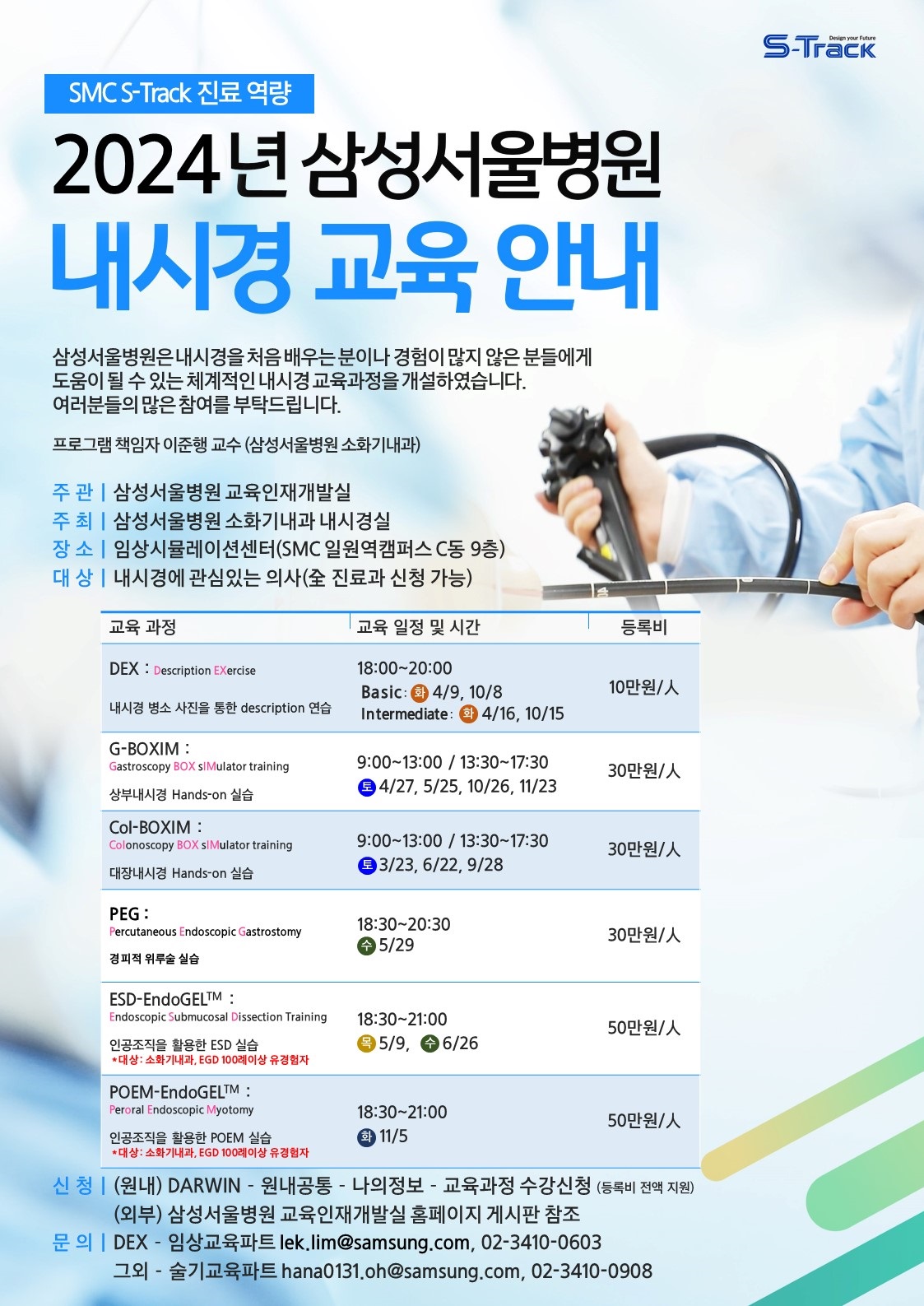
[2023-12-19] 2024년 SMC 내시경 hands-on training 일정이 나왔습니다.
2024년 잠정 계획. 변경 가능
[2023-12-19] HUG Vietnam webinar (동아 ST)
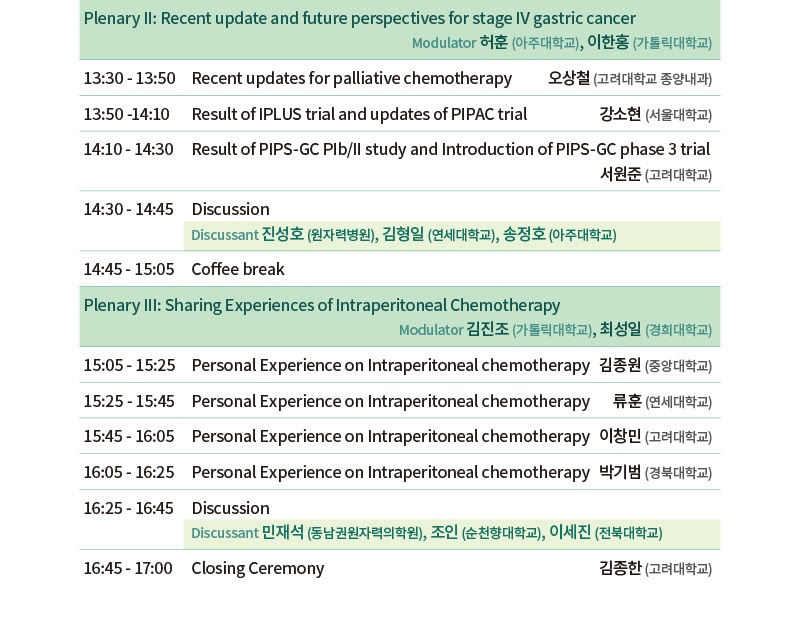
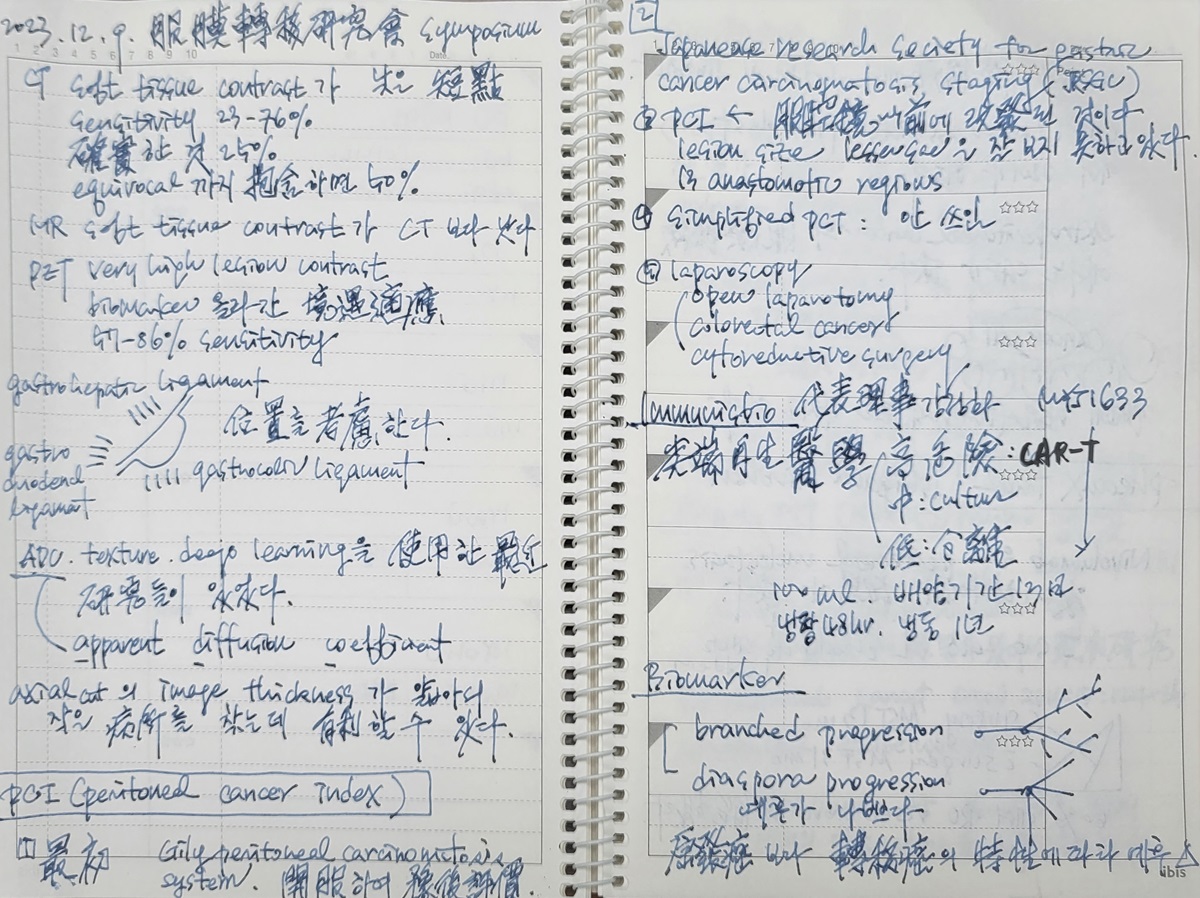
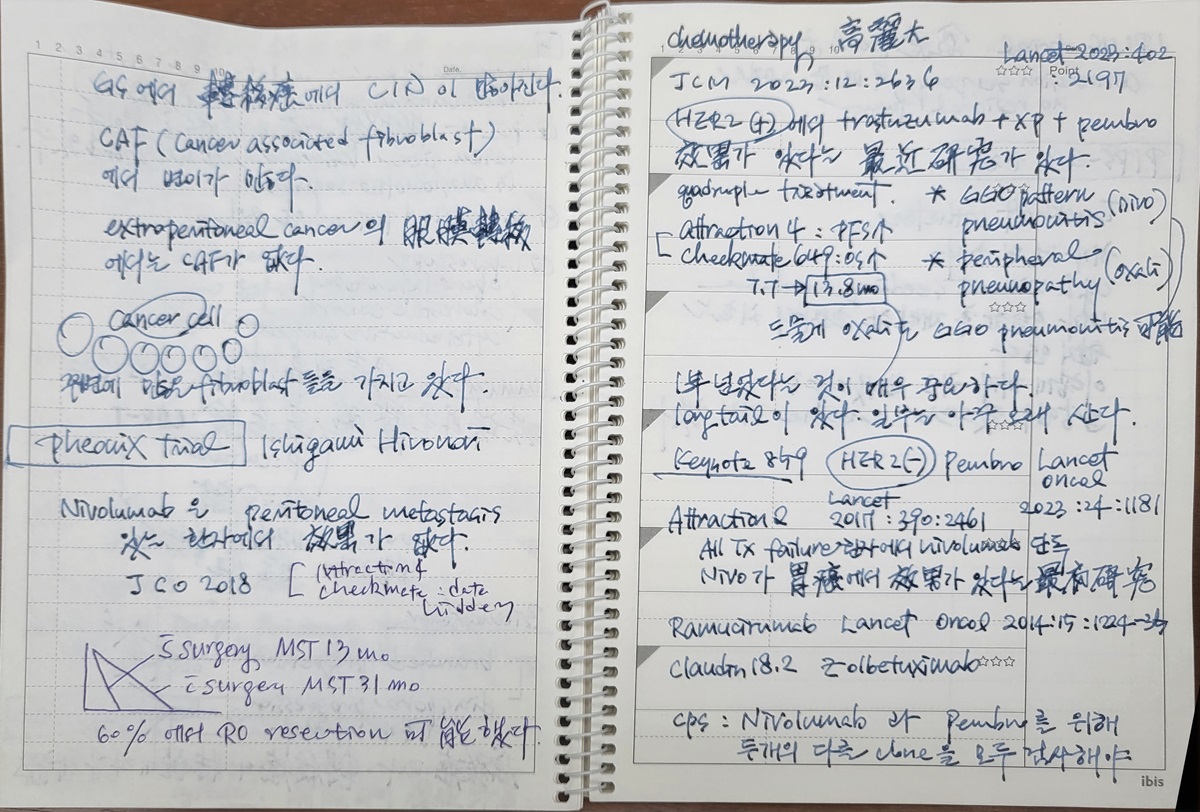
[2023-12-9] 위암복막전이연구회 (고려대학교 구로병원 새롬교육관 1F 대강당)
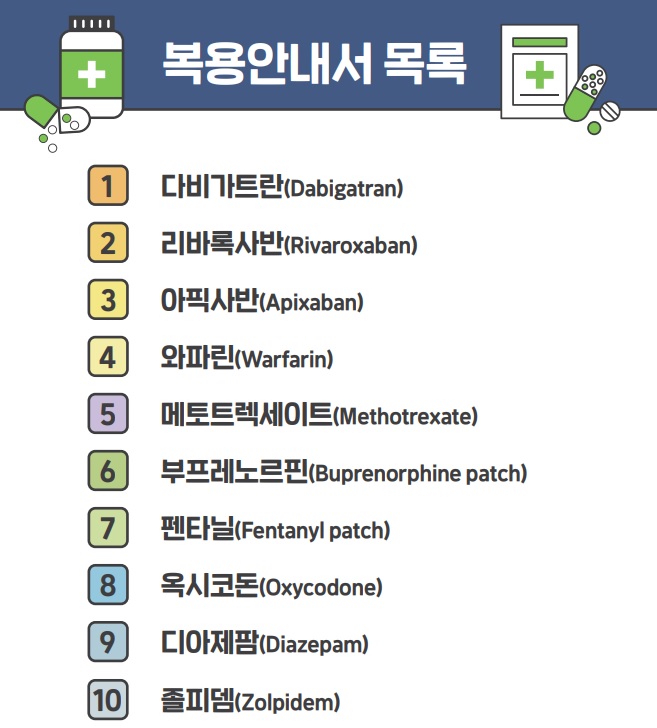
[2023-12-8] 2022년 말 인증원에서 KOPS를 통하여 정확하고 안전한 복용안내서를 게시하였습니다.
PDF 10.0M
제가 관심있게 본 것은 복용안내서 목록입니다. 맨 앞 4개가 NOAC과 warfarin이었기 때문입니다. 내시경 검사와 관련하여 중단 여부를 고민하는 약제가 가장 위험한 약으로 언급되고 있으니 그 중요성을 알 수 있습니다.
[2024-12-7] 여수 질향상학회. 3개병원 식사.
[2024-12-5] BOXIM training for a Mongolian doctor
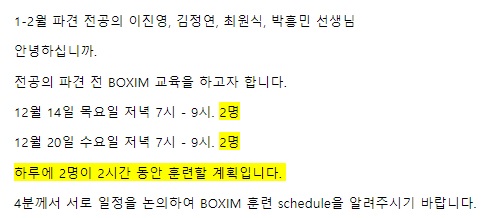
[2024-12-4] 내과 전공의 파견 전 BOXIM을 시작하였습니다.
[2023-12-19] HUG 베트남 webinar 증례 발표
Today, I’d like to present two cases of closely related gastric lesions which can be found in Helicobacter pylori negative patients.
Gastric cancers usually develop in the stomach with Helicobacter pylori infection. With widespread eradication therapy, we can see gastric adenomas/cancers in patients without Helicobacter pylori infection.
The first case is adenocarcinoma of fundic gland type.
A forty-six years old lady was referred for the evaluation of a flat pale elevated mucosal lesion. Biopsies at the local clinic were mild glandular hyperplasia and focal regenerative change.
Repeated biopsy at my hospital showed atypical proliferation of fundic glands, suggestive of tubular adenocarcinoma, well differentiated, fundic gland type.
Background gastric mucosa was very clean, and serology for Helicobacter pylori was negative.
Although the location was a little bit difficult, ESD was done as usual.
Final pathology was 18 mm sized EGC 2a. It was a tubular adenocarcinoma, well differentiated, fundic gland type. The depth was 300 micrometer SM invasion. There was no lymphatic, and venous invasion.
The upper mucosal layer looked normal. In the lower mucosal layer, the structural atypia of the oxyntic glands was clear. The atypical glands were variable in size and shape with branching and anastomosing pattern. The tumor cells had centrally placed round and mildly atypical small nuclei. The cytoplasm of the tumor cells was basophilic like chief cells.
In this section, you can see the submucosal invasive lesions. Glands in the submucosal layer were mostly dilated, and the tumor cells were columnar or cuboidal with almost normal looking nuclei. Vertical resection margin was negative.
After a multidisciplinary discussion, follow up without additional surgery was recommended.
In the first follow up endoscopy, there was no evidence of recurrence. Histology for Helicobacter pylori was once again negative.
Recently, we did a follow up endoscopy again, and everything was OK.
This is a similar case. There was a small flat elevated lesion in the fundus.
Because of the difficult location, snare resection was done after circumferential cutting.
The pathology was tubular adenocarcinoma of fundic gland type. SM invasion was 200 micrometer.
This is another case of fundic gland type adenocarcinoma. It was limited in the mucosal layer.
From now on, I’d like to present oxyntic gland adenoma, which is considered as a pre-cancerous lesion of the fundic gland type adenocarcinoma.
On the posterior wall aspect of the mid to high body, a flat elevated lesion was found. Outside pathology was a few atypical oxyntic glands, suspicious for oxyntic gland adenoma. Helicobacter serology was negative.
The biopsy result was focal fundic gland dysplasia.
After a careful discussion with the patient, ESD was done.
On the posterior wall aspect of the mid-body, a 1cm sized oval flat pale elevated lesion was found. There was a focal hyperemic mucosal change probably due to previous biopsy at a local clinic. Small ESD was done as usual.
Final pathologic outcome of the ESD specimen was reported as oxyntic gland adenoma with high grade dysplasia. The long diameter was 6mm and the resection margins were negative.
In the low power view, there were clusters of irregular glands separated by radiating fibers of smooth muscle. The oxyntic glands were dilated, branched, fused and anastomosed with each other. Mucosal surface is spared and covered by gastric foveola and nonneoplastic oxyntic glands.
In the higher power view, the glands were mostly composed of columnar epithelial cells with chief cell differentiation characterized by basophilic cytoplasm and relatively uniform round nuclei. You can find some parietal cells with eosinophilic cytoplasm. The cytological atypia is not prominent.
Gastric polyps can be classified into two types by the mucosal compartment of origin. Hyperplastic polyps and tubular adenomas are surface epithelium-derived lesions. On the other hand, fundic gland polyps and oxyntic gland adenomas are gastric gland-derived lesions.
Mean age of patients with oxyntic gland adenoma is 66 years, with a male predominance. It is usually elevated lesion from 3 to 40 mm. OGAs can display a chief cell-predominant pattern, an admixture of chief and parietal cells resembling normal fundic glands, and a predominant mucous neck cell and foveolar differentiation pattern.
OGAs are composed of tightly packed tubules and trabeculae. Nuclear atypia is usually mild to moderate. Mitotic figures are rare. In contrast, high grade OGAs are characterized by complex anastomosing glands and more pronounced cytonuclear atypia. If submucosal invasion is present, should be classified as gastric adenocarcinoma of fundic gland type.
Fundic gland type EGC is a recently recognized, rare pathologic subtype of gastric adenocarcinoma. Histologically, fundic gland type adenocarcinoma is a well-differentiated adenocarcinoma mainly composed of cells resembling chief cells and is classified into chief cell predominant type, parietal cell predominant type, and mixed type.
Fundic gland type adenocarcinomas can develop from oxyntic gland adenomas.
Foor types of non-cardia Helicobacter pylori-negative gastric cancer were proposed, and adenocarcinoma of the fundic gland type is one of them.
Thank you for your attention.
여수 - 향일암. 청정게장. 명동게장. 넘너리바닷가 (하모샤브샤브). 모이핀 카페.
모이핀 카페에서 바라본 한려수도
![]() © 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (since 1999-8-23)
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (since 1999-8-23)