 EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
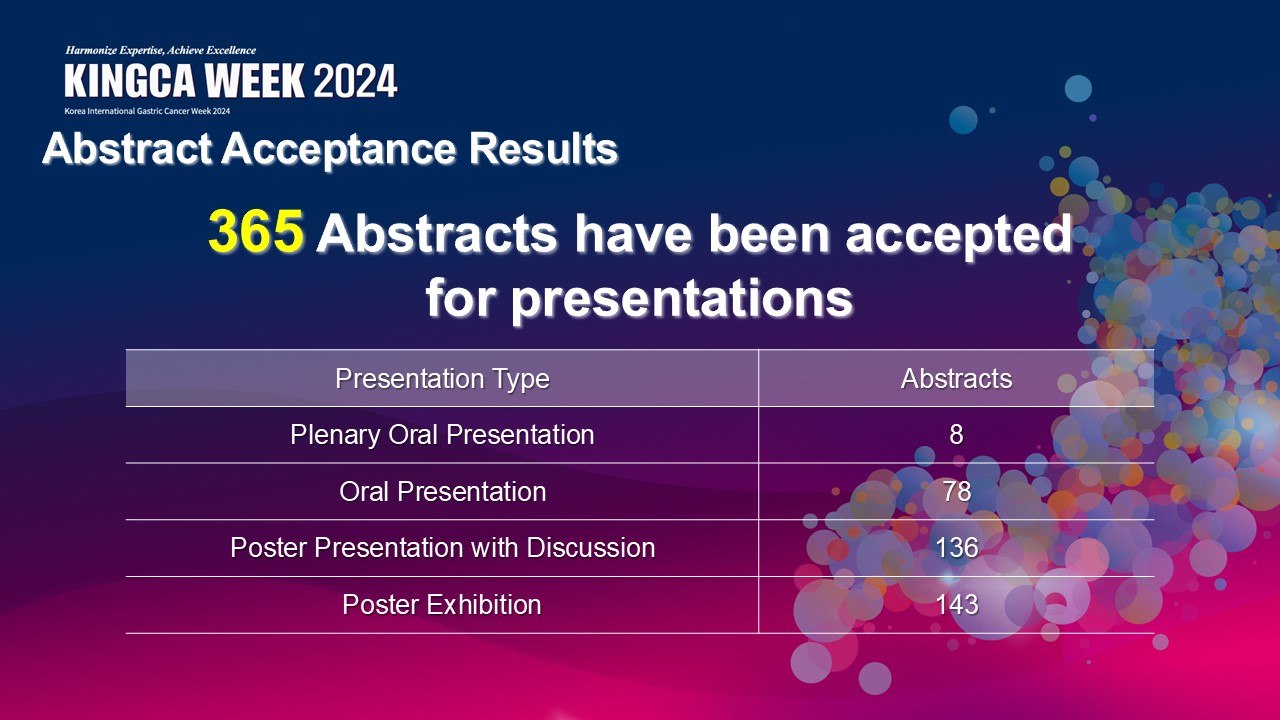
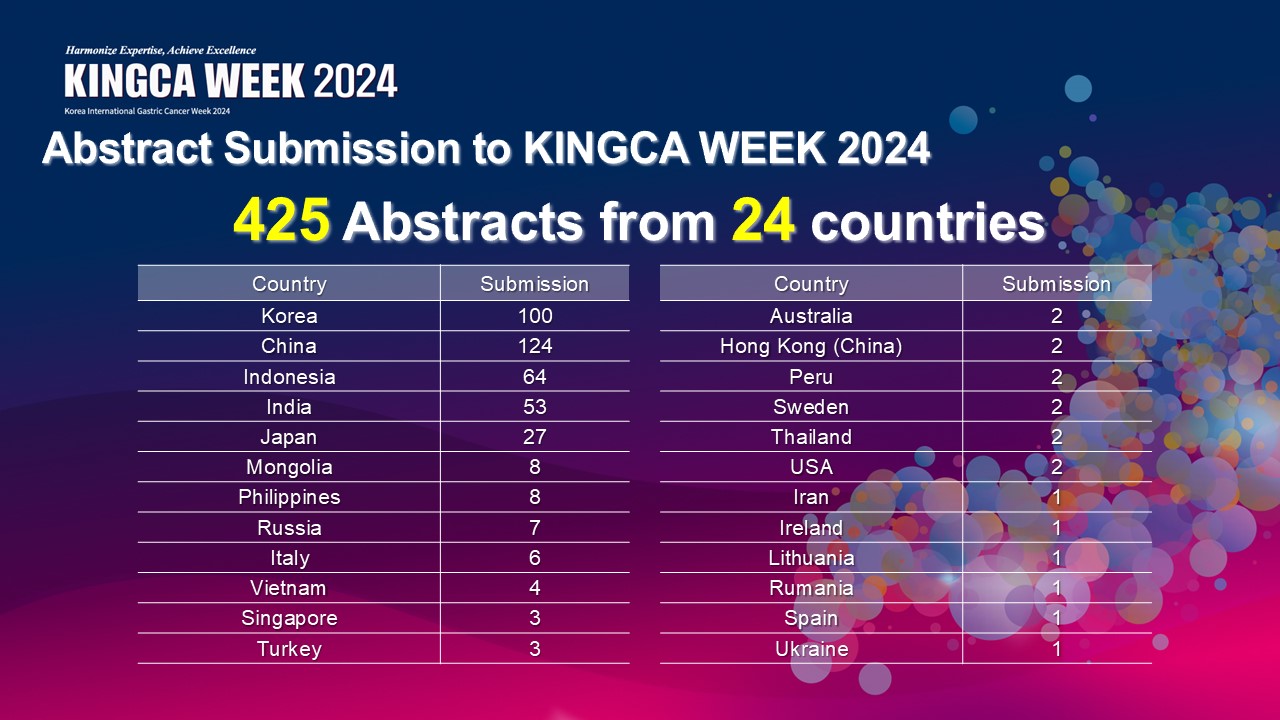
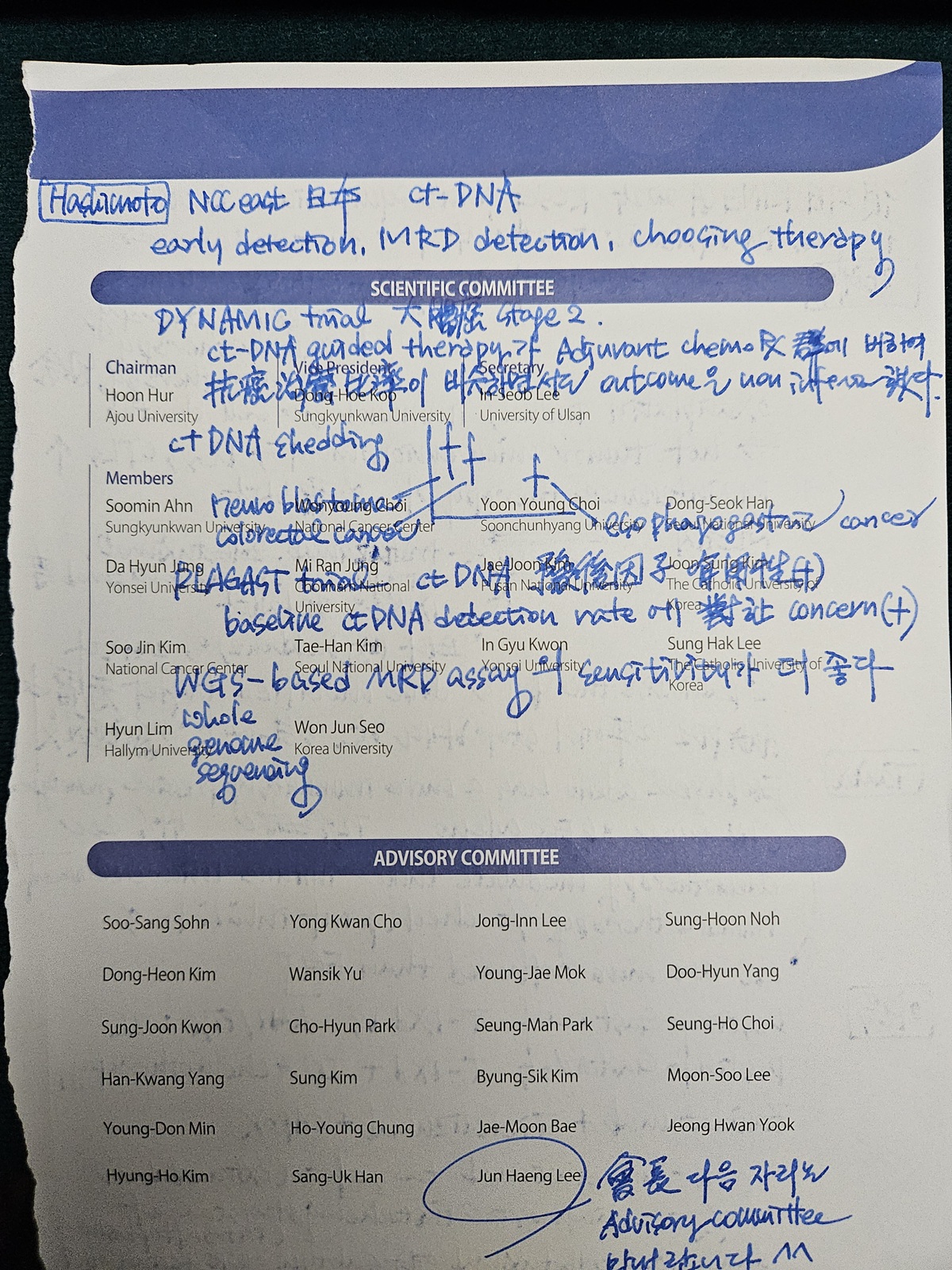
![]() [ДыЧбРЇОЯЧаШИ ЧаМњЧрЛч. KINGCA and KGCA] - №ћ
[ДыЧбРЇОЯЧаШИ ЧаМњЧрЛч. KINGCA and KGCA] - №ћ
[2026-6-17] РЇОЯЧаШИ ЧаМњСі Q1 СјРд. УрЧЯЧеДЯДй.
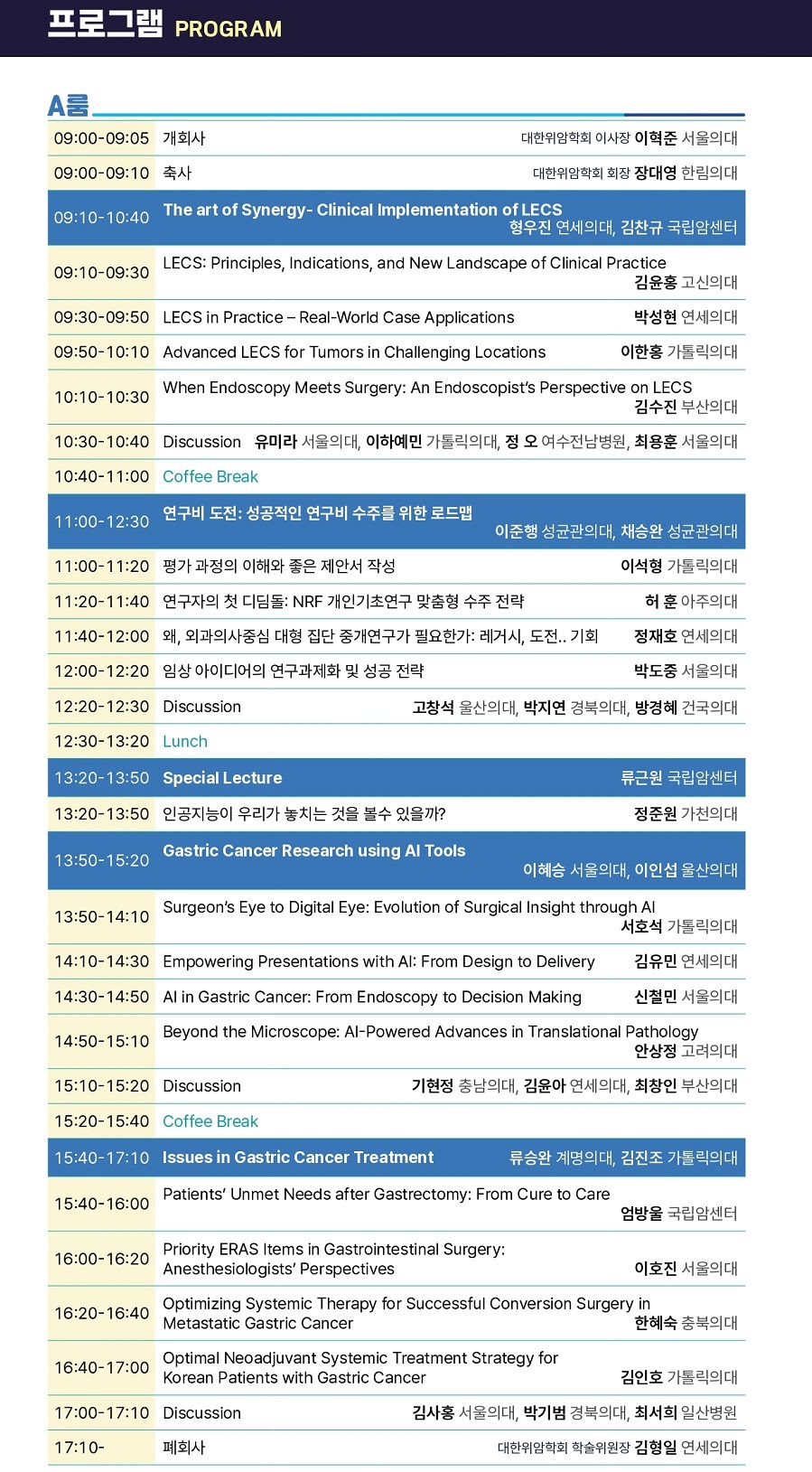
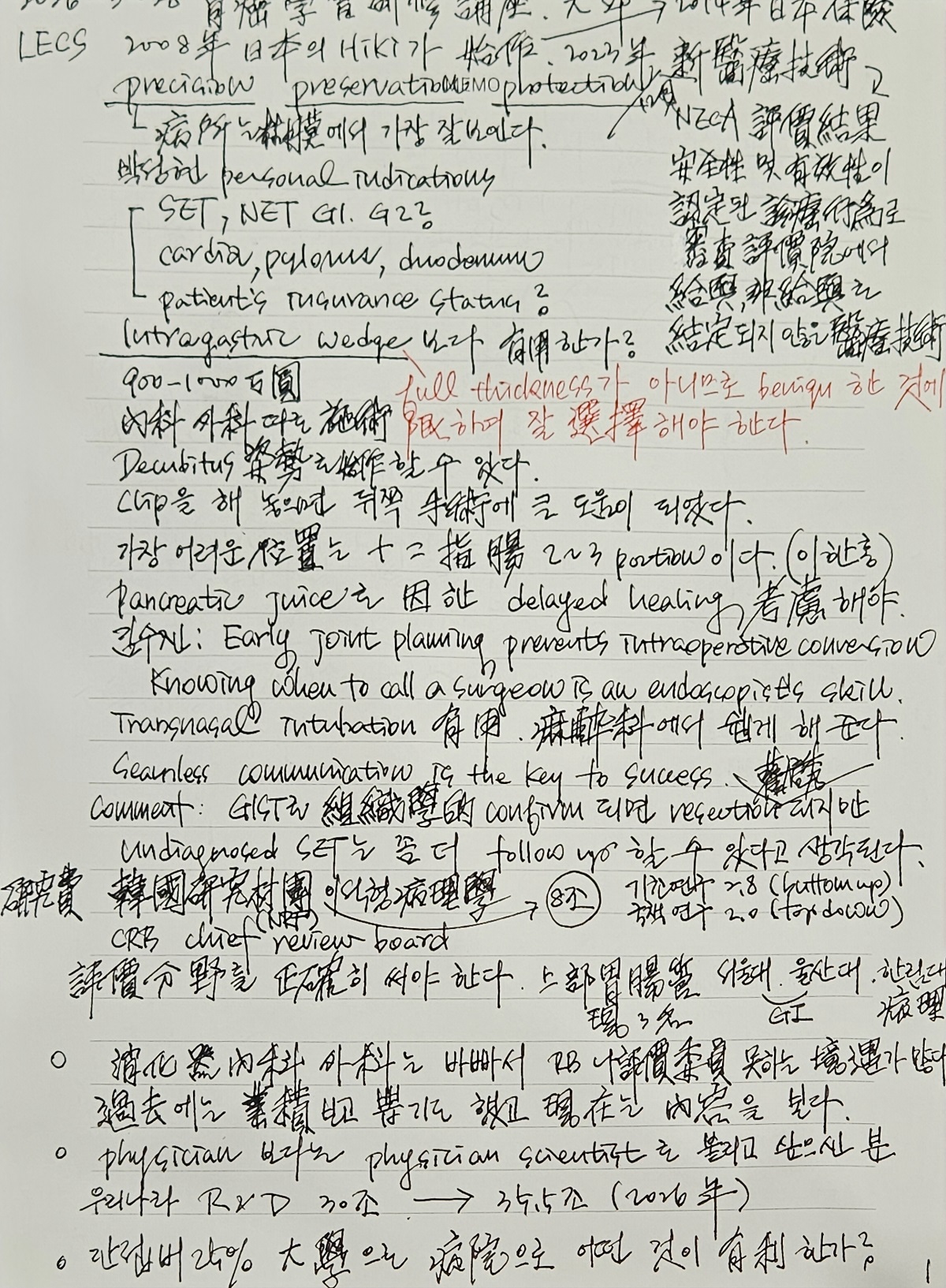
[2026-5-28] РЇОЯЧаШИ ДйЧаСІ С§ДуШИ. (1) АЃРЬНФ ШЏРкРЧ РЇОЯ ESD, (2) LECS


РЇ NETПЁ ДыЧб ИоХИКаМЎ(Dig Endosc 2025)ПЁМ ИВЧСР§ РќРЬДТ type 1ПЁМ 6.0%, type 2ПЁМ 38.5%, type 3ПЁМ 23.2% ПДРИИч, РЇЧшРЮРкДТ tumor size >10 mm (4.18), tumor invasion into the muscularis propria or deeper (11.21), grade 2/3 (5.96), and lymphovascular invasion (34.50) ПДНРДЯДй. 1.5cm КИДй РлРК СїРх NET 652ПЙПЁ ДыЧб ПьИЎГЊЖѓ ДйБтАќ ШФЧтРћ ПЌБИ (Gut Liver 2021)ПЁМ 75ПЙ (11.5%)ПЁМ lymphovascular invasionРЬ РжОњАэ, МіМњРЛ НУЧрЧб 41ПЙРЧ 48.8% (20/41)ПЁМ ИВЧСР§ РќРЬАЁ РжОњНРДЯДй.
[2026-3-28] РЇОЯЧаШИ НЩЦїСіОі. ДыБИ EXCO
![]() [2026-3-21] ПмАњ ЧеЕП НЩЦїСіОі
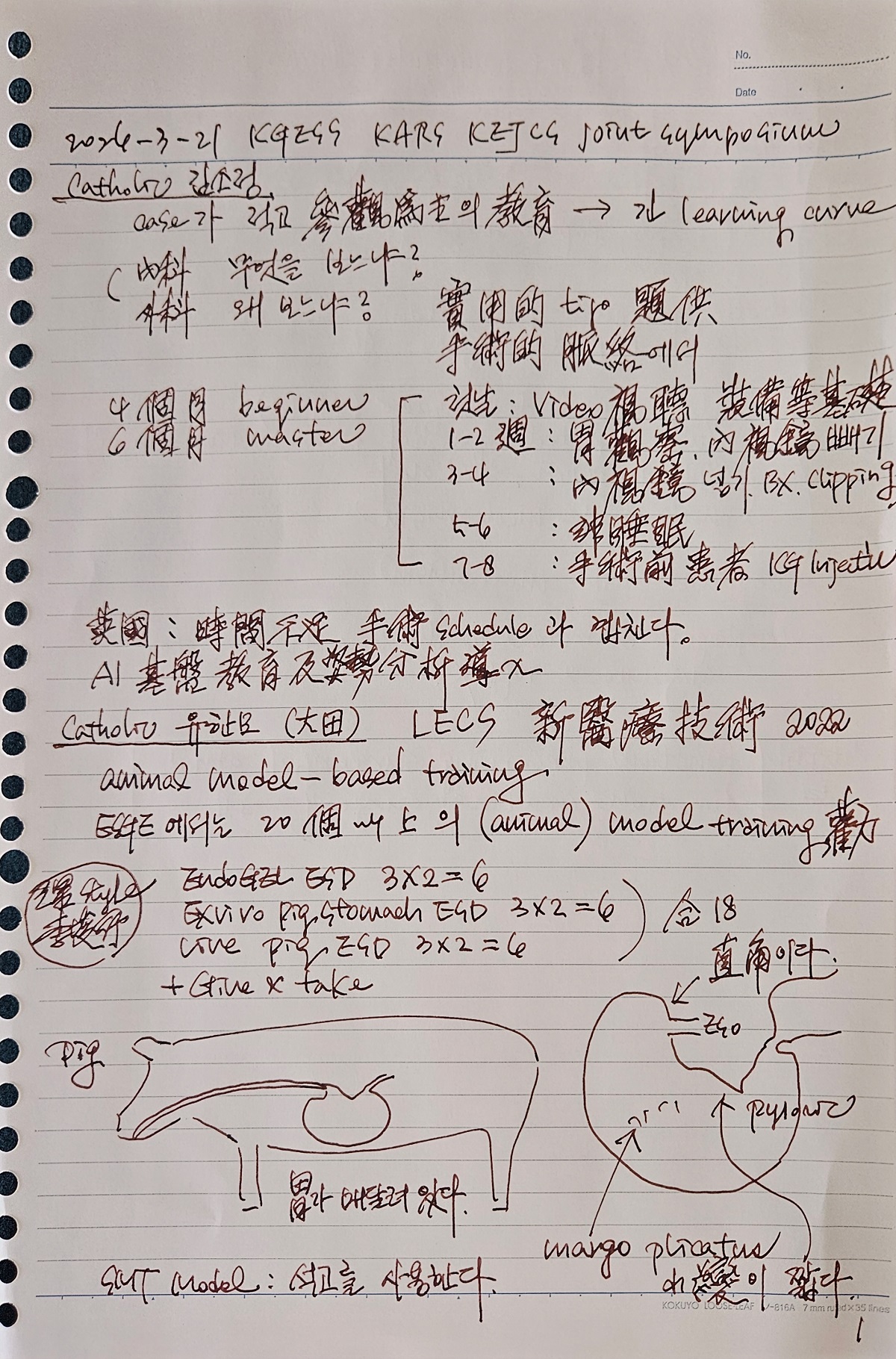
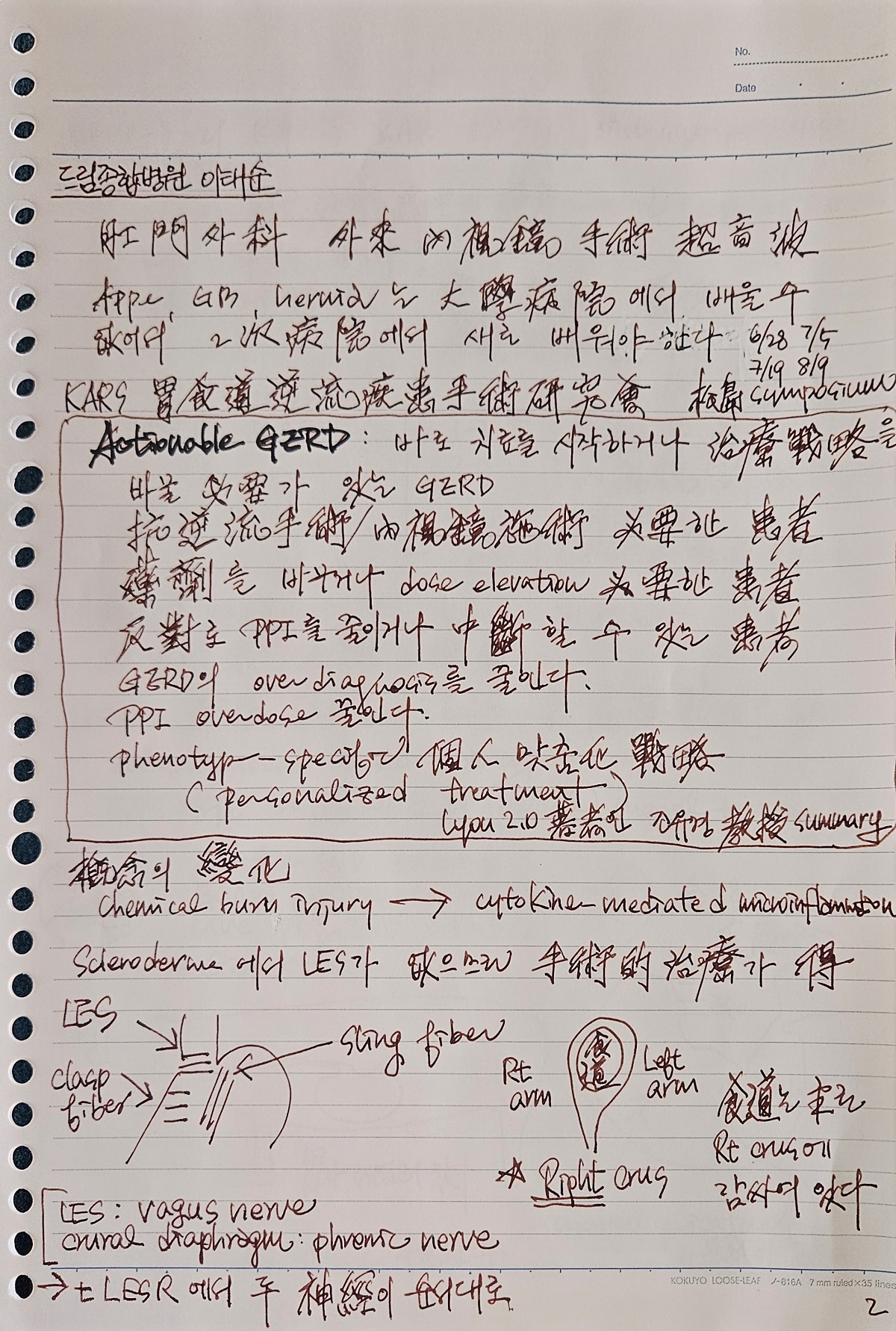
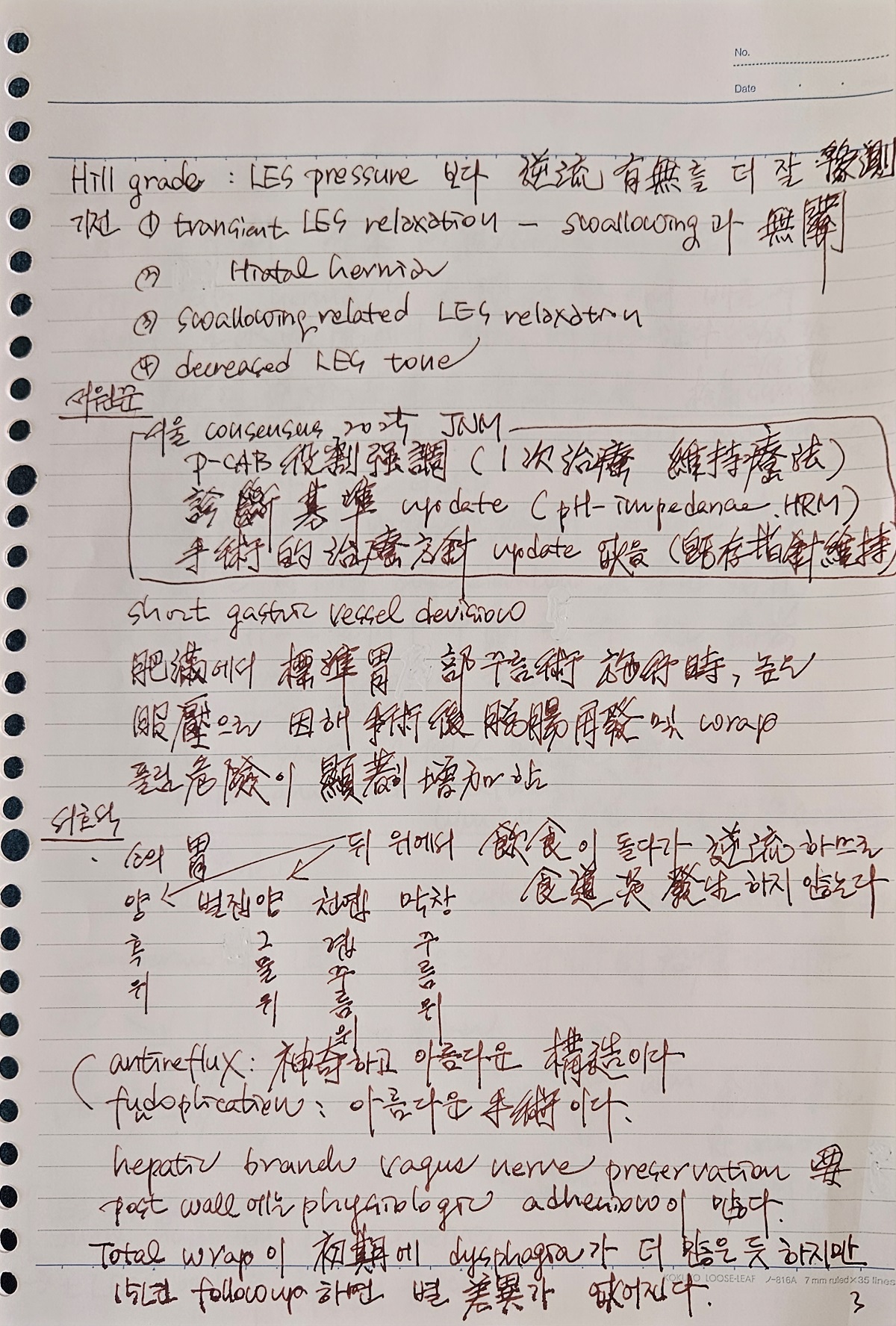
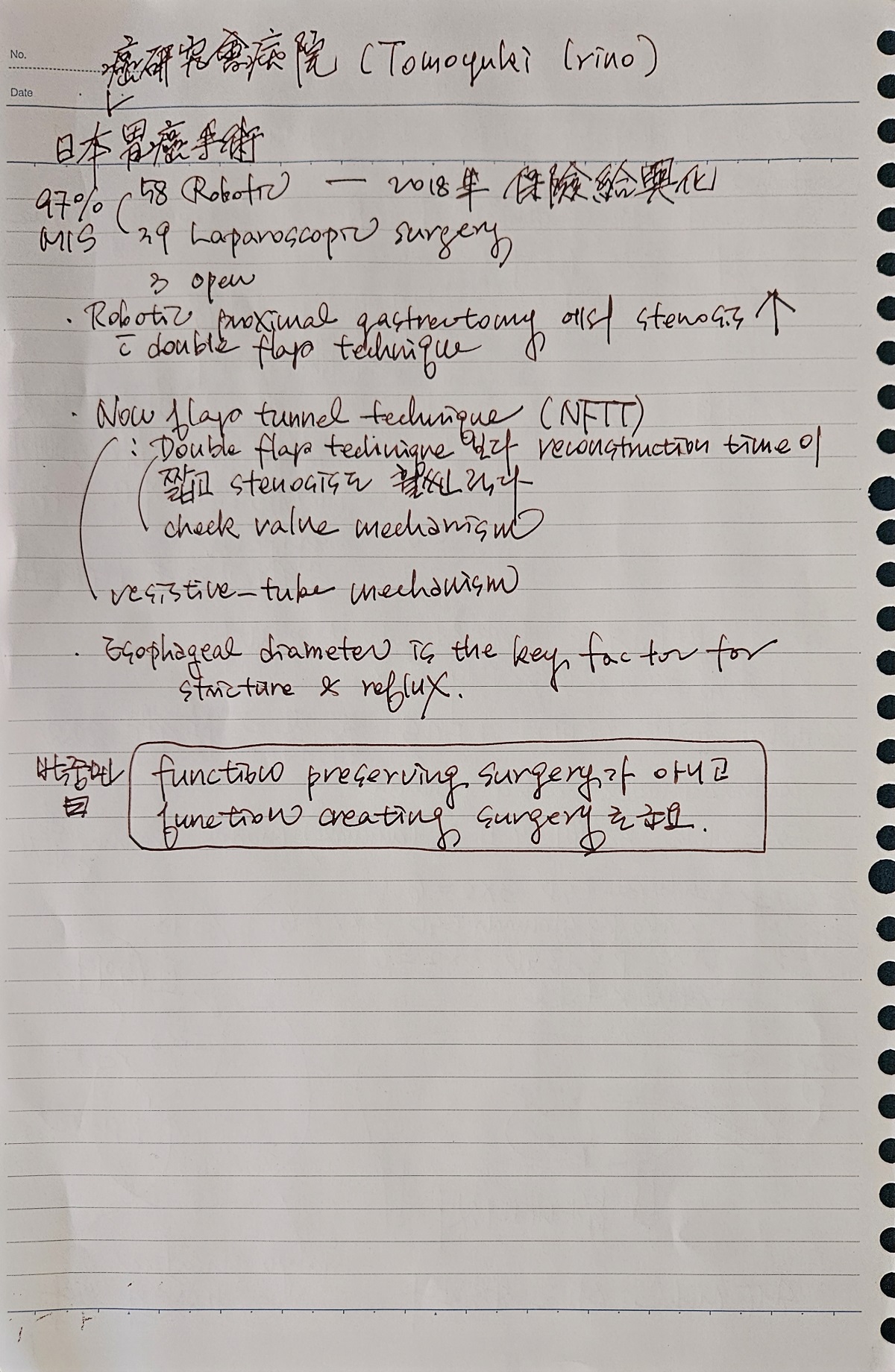
[2026-3-21] ПмАњ ЧеЕП НЩЦїСіОі
[2025-9-25] KINGCA 2025
[2025-5-22] ДйЧаСІ С§ДуШИ
[2025-5-8] IGCC 2025

Ladies and Gentlemen, itЁЏs a great honor for me to talk here today. This is our baseline. Pretreatment staging of gastric cancer is integral in selecting patients for appropriate, evidence-based treatment. Recently, KGCA released a revised version of the previous 5th evidence-based gastric cancer guideline in JGC. The first three statements are about staging. The accuracy of EUS in a recent Cochrane review, the differentiation between T1a vs. T1b, the sensitivity was 87%, and the specificity was 75%. In the evaluation of lymph node, the sensitivity is 83% which is acceptable, but the specificity was less than expectation, 67 percent. This case shows our typical approach for initially metastatic cancer. After endoscopy and detailed pathologic evaluation, CT and PET was done. The initial regimen was XELOX with Opdivo. This is the overall treatment algorithm in the recent Korean guideline. Regarding the staging, EUS and PET/CT are mentioned as optional modalities. When do we need EUS for initial staging of gastric cancer? IЁЏd like to split my discussion into two parts. Role of EUS before ESD In a recent audit for gastric cancer treatment in Korea, surgical resection was done in 60%, and endoscopic resection was done in 40%. More than 10 thousands cases of EGC were annually treated by ESD not only in tertiary hospitals but also in general hospitals. At my institution at Samsung Medical Center, gastric ESD is done about 1,000 cases a year. In the recent 5 years, the rate of gastric cancer among ESD cases was 73%. The rate of additional surgery after ESD for gastric cancer was 15%. The accuracy of EUS in the Yonsei University Severance hospital study, EUS T staging was correct in 63%. The rate of over-staging was quite high, 36%. The good news is that the major factors for incorrect EUS diagnosis were undifferentiated type histology and larger tumor size, which are usually out of the indications of endoscopic treatment. Cases A forty-five years old man was referred for a small elevated type lesion with slightly unclear margin. The histology was tubular adenocarcinoma, moderately differentiated. The third hyperechoic layer looked interrupted, which suggested submucosal invasion. Surgery was recommended at the local hospital. What would you recommend? I suggested diagnostic ESD but the patient wanted surgical treatment. [Click] Final pathology was EGC with SM2 submucosal invasion without lymph node metastasis. In the review process of this case, I found some areas of submucosal invasion in the initial endoscopic forceps biopsy specimen. The existence of submucosal invasion is not formally reported in the forceps biopsy pathology. In my opinion, definite submucosal invasion in forceps biopsy can be considered as strong indicator for surgery rather than ESD. I hope pathologists report these findings in their formal report. The second case. A fifty-nine years old man was referred. In EUS, the third hyperechoic layer was interrupted, so surgery was previously recommended. However, I recommended a diagnostic ESD. The ESD procedure was done as usual. And the final pathology was EGC with mixed histology, 28mm and the depth of invasion was muscularis mucosa. There was no recurrence. IЁЏd like to introduce an interesting real-world experience of EUS before ESD. Professor Lee at Korean National Cancer Center evaluated the effectiveness of an EUS-based plan compared to an endoscopy-based plan. Overall, the appropriate treatment selection were 75% in the endoscopy-based plan and 71% in the EUS-based plan. [Click] For endoscopic mucosal cancers, the appropriate treatment selection rates in the endoscopy-based plan were 88%, while the use of an EUS-based plan decreased this rate to 81%. The authors concluded that EUS may not be necessary before treating differentiated-type EGC, especially in endoscopically presumed mucosal cancers. European guideline also said that precise endoscopic evaluation is sufficient with EUS reserved only for selected cases. Based on previous discussion, I can say that endoscopic evaluation without EUS is sufficient for mucosal cancer with differentiated type histology. However, indications of ESD is expanding in terms of depth of invasion and histological types. For EGCs with differentiated type histology, ESD is frequently performed for small submucosal cancers when the depth of invasion is less than 500 um. Recently, diagnostic value of EUS for suspected submucosal cancers was evaluated in Japan. The overall accuracy for SM1 invasion was 58% for conventional endoscopy and 75% for EUS. However, the rate of over-staging among indicated cancers were quite high, 26%. This is the treatment outcome or the previous study. Based on EUS findings of SM2 or more, surgery was done in 72 patients. Among them, 16 cases were actually mucosal or SM1 cancers. They suggested that mucosal or SM1 lesion is suspected in conventional endoscopy, EUS does not change the final diagnosis. If SM2 or deeper lesion is suspected in conventional endoscopy, additional information from EUS can influence their final diagnosis. Staging T1a and T1b with EUS is quite tricky and an operator-dependent procedure. In this interesting study from China, saline injection before EUS improved the diagnostic accuracy for T1b staging in superficial esophageal cancer. Diagnostic accuracy was 93% in saline injection EUS and 65% in conventional EUS. Professor Park at ЛѓАшЙщ hospital examined the efficacy of saline-injection EUS in EGC. The diagnostic accuracy in this small single center study was like this. Although it is less than esophageal cancer, saline injection helps. Randomized multicenter clinical trial is on-going by professor Kim of Samsung Medical Center. This is a typical example. In conventional EUS, it looks like SM cancer, but after saline injection there was no evidence of submucosal invasion. In the final pathology, it was a poorly differentiated tubular adenocarcinoma limited in the mucosa. Are there more factors influencing the treatment option other than depth of invasion by conventional endoscopy and EUS? In order to predict the risk of non-curative ESD, we developed a risk scoring system. We found six independent variables such as pathology, size, axial location, circumferential location, macroscopic morphology, and ulcer. Based on the relative risk we made a score for each variables. This is the correlation between the total risk score and the predicted risk of non-curative ESD requiring gastrectomy. These factors can be considered when choosing the initial treatment options for early gastric cancers. IЁЏd like to briefly comment on the clinical importance of submucosal invasion found in the forceps biopsy. A 51 years old male patients was referred for an 1.5cm-sized EGC 2c with shallow central erosion. ESD was initially considered. However, submucosal invasion was clearly seen in the forceps biopsy. What would you do? I recommended surgery and the final surgical pathology was SM2 invasion without lymph node metastasis. SM2 invasion. Until now, it is not clear whether evidence of submucosal invasion in forceps biopsy is a contraindication of ESD. Further data is required, but I usually send the patient to surgeons especially for borderline cases with SM invasion in forceps biopsy. EUS in AGC In western countries, preoperative therapy is generally recommended for tumors that are staged on EUS as T3-4 or as lymph node-positive disease (N+), whereas immediate surgery is generally recommended for T1-2N0 tumors. In eastern countries, upfront surgery followed by adjuvant chemotherapy is more commonly used for most advanced gastric cancers without definite distant metastasis. So, the role of EUS is different in East and West. This is a famous neoadjuvant chemotherapy trial for advanced gastric cancer in Korea. Even in this trial, clinical staging was mostly based on CT findings without EUS. Non-interventional EUS is mostly reserved for borderline early gastric cancers in Korea. Ladies and gentlemen, IЁЏd like to conclude my talk by saying that gastric cancer staging is mostly based on conventional endoscopy, CT and PET/CT. EUS has some role in selecting patients for ESD, especially when SM cancer is suspected. The role of diagnostic ESD in increasing. Thank you very much for your attention.
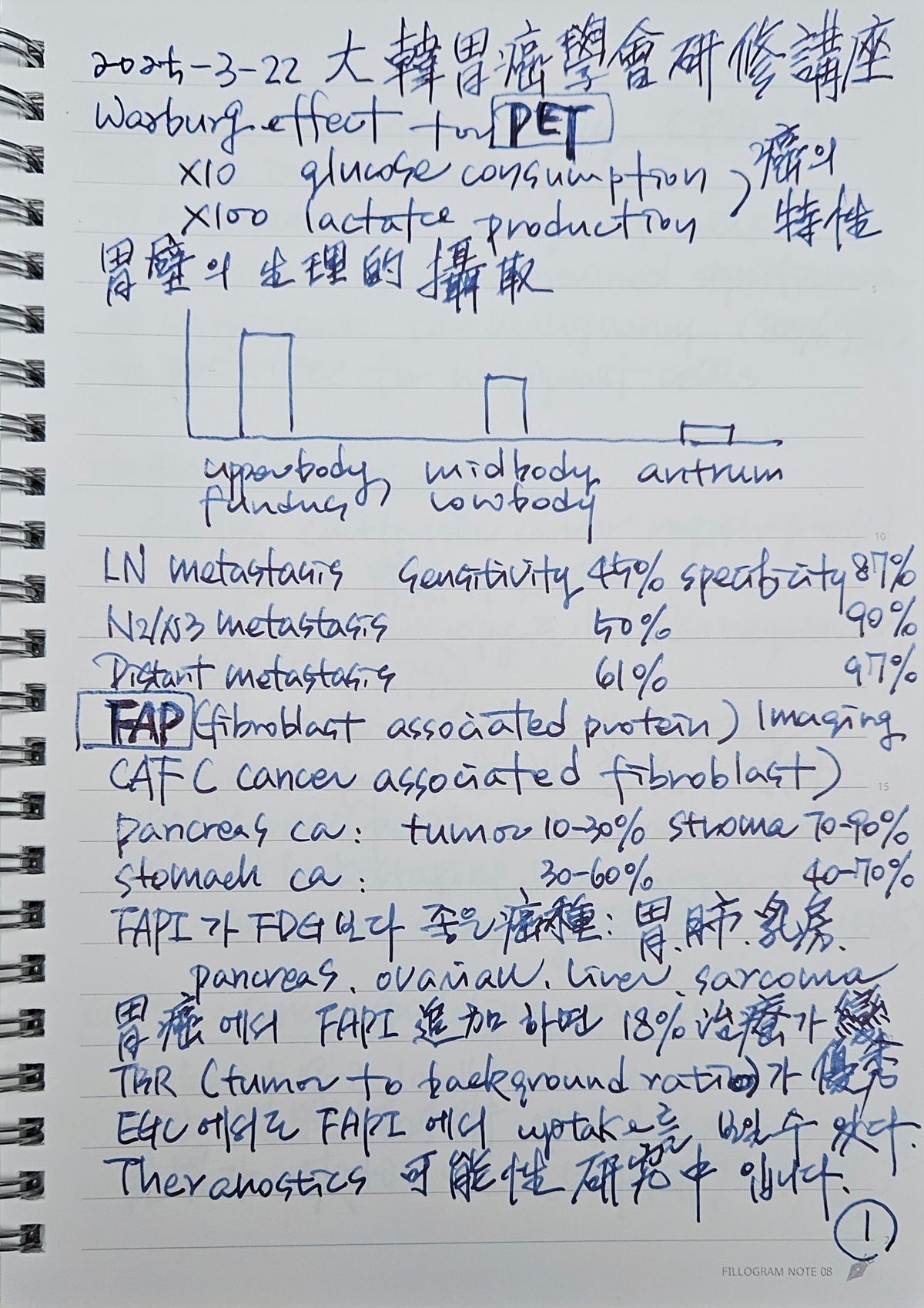
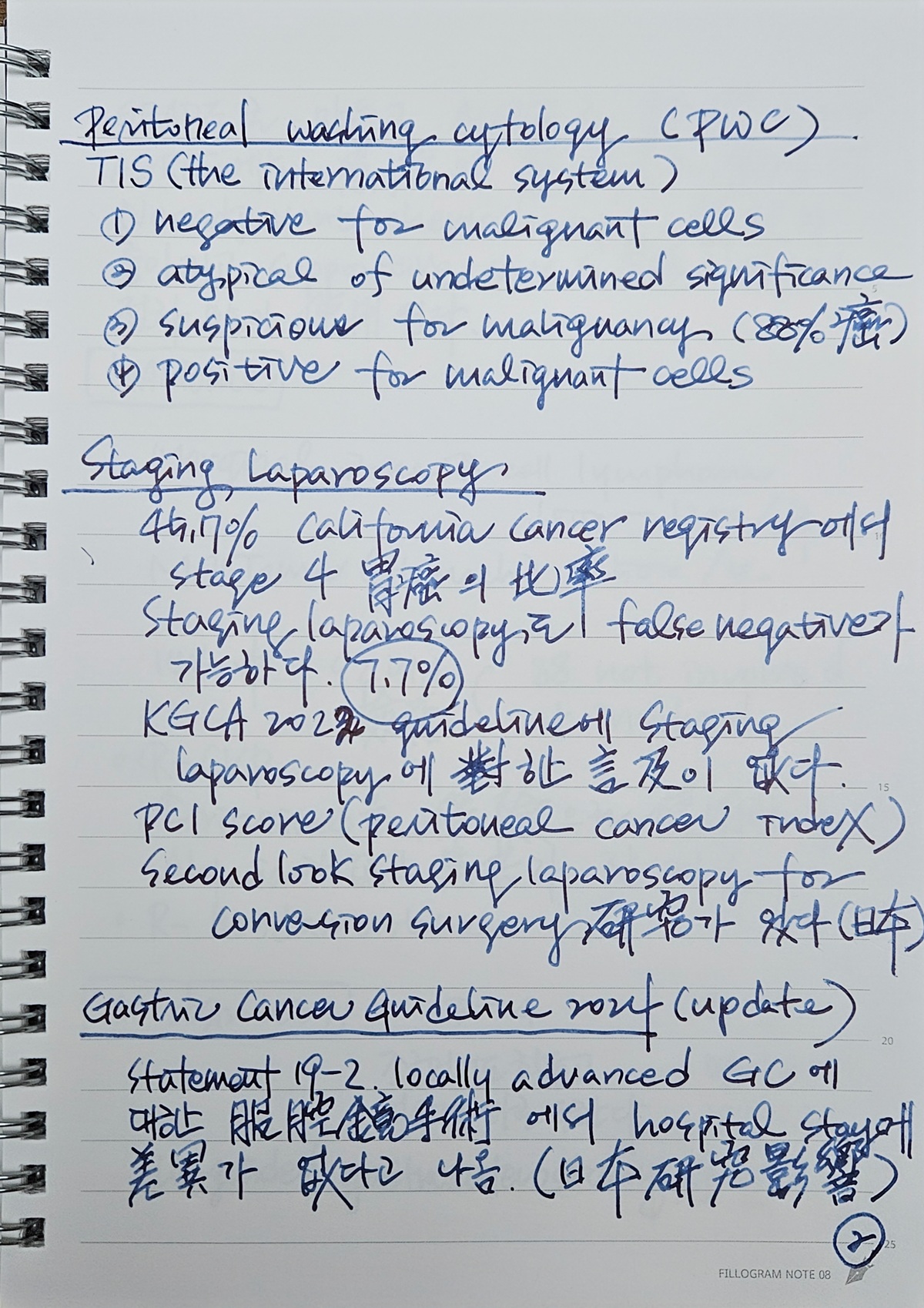
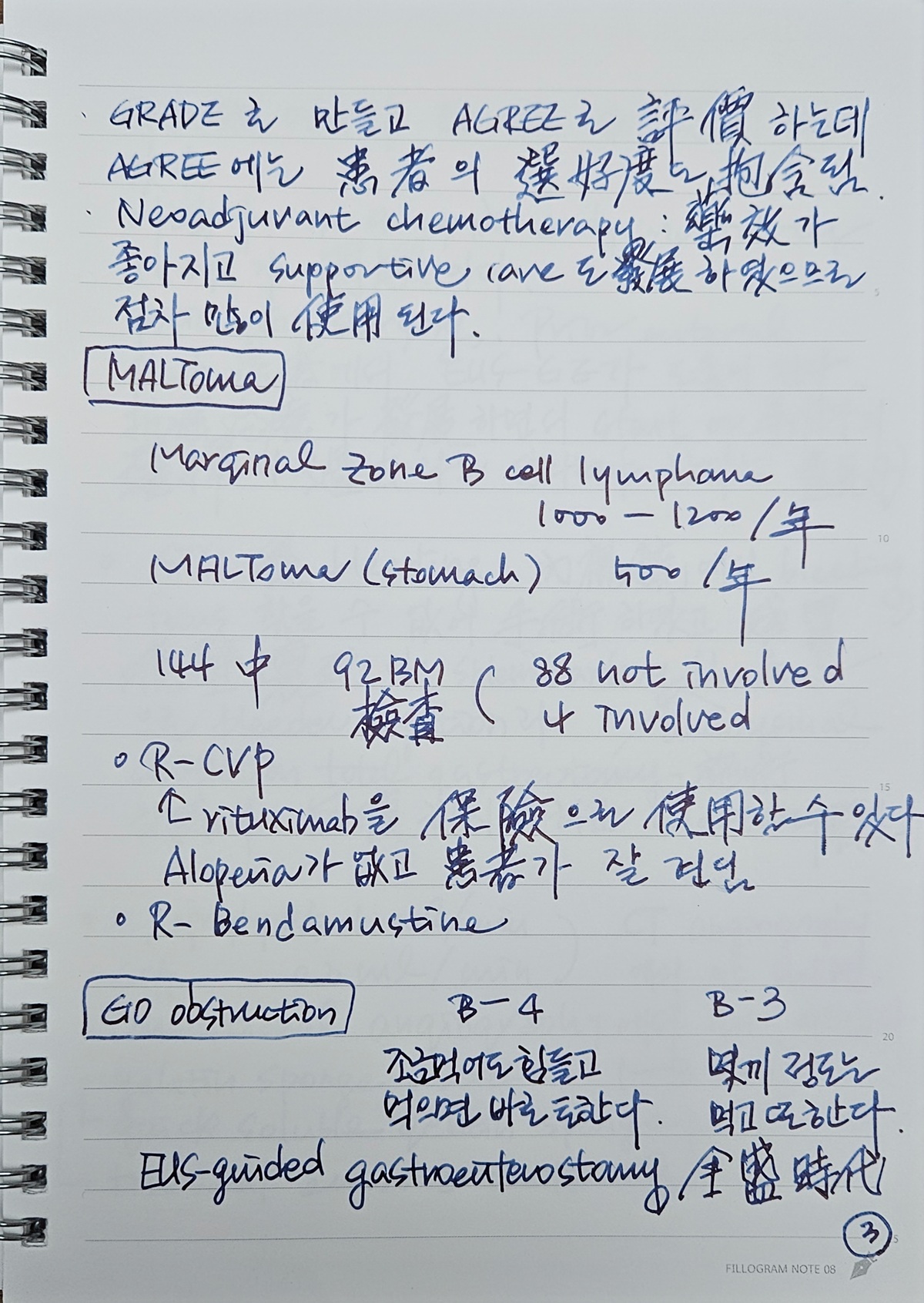
[2025-3-22] РЇОЯПЌМіАСТ (БЄСж)
2025-3-22. KGCA ПЌМіАСТ. Log-in щЉ


[2024-11-28] ДыЧбРЇОЯЧаШИ ДйЧаСІ С§ДуШИ
ПЉЗЏКа. ЙКАЁ ЛѕЗЮПю АЭ ЧЯГЊИІ ЙшПьБт РЇЧЯПЉ ОѓИЖГЊ ХѕРкЧиОп ЧвБюПф? РњДТ МіЙщИИПјРЛ ЕщПЉ ЙЬБЙ ЧаШИПЁ АЁМ ЦЏКАЧб АЭРЛ ЙшПьСі ИјЧб РћЕЕ РжНРДЯДй. РлРК ЙпЧЅАЁ РжОюМ ОюТП Мі ОјРЬ ТќМЎЧб 2014Гт Chicago DDWАЁ ИЖСіИЗРЬОњНРДЯДй. ЙКАЁИІ СЖБн ЙшПьБтДТ ЧпДТЕЅ РќУМРћРИЗЮДТ НУАЃАњ ЕЗРЬ ОЦБюПќНРДЯДй. ЦЏШї РЇОЯРЛ АјКЮЧЯДТ РњПЁАдДТ КАЗЮПДНРДЯДй. Chicago symphony ПЌСжШИПЭ Chicago cubs ОпБИ АдРг БзИЎАэ ЙЬМњАќПЁМ КЛ МшЖѓРЧ БзИВРК ССОвДТЕЅ ИЗЛѓ ЧаШИАЁ КАЗЮПДНРДЯДй. БзЗЁМ Дѕ РЬЛѓ ЙЬБЙПЁДТ ОШ АЉДЯДй. РЯКЛ ЧаШИДТ АЁВћ АЉДЯДй. ЙшПя СЁРЬ ИЙРИДЯБю. ЙнИщ БЙГЛПЁМ СјЧрЕЧДТ С§ДуШИПЁМ ИЙРК АЭРЛ ЙшПьАэ РжНРДЯДй. И№Еч С§ДуШИАЁ Дй ССРК АЭРК ОЦДеДЯДй. 1НУАЃ СЄЕЕ С§ДуШИИІ ЧЯАэ ЙфИдАэ МњИЖНУДТ БзЗБ ЧрЛчДТ no thank youРдДЯДй. С§ДуШИАЁ СпПфЧбСі МњРкИЎАЁ СпПфЧбСі ОЫ Мі ОјДТ БзЗБ ЧрЛчДТ ЛчОчЧеДЯДй. С§ДуШИ Рќ ЙЬИЎ НФЛчИІ ЧЯАэ С§ДуШИ РкУМДТ НУАЃПЁ БИОжЙоСі ОЪАэ ГЁРх ХфЗаРЛ ЧЯДТ БзЗБ И№РгРЬ С§ДуШИДфНРДЯДй. РЇОЯЧаШИ ДйЧаСІ С§ДуШИАЁ ЙйЗЮ БзЗЏЧеДЯДй. НЌСі ОЪАэ 3НУАЃРЛ Чб РћЕЕ РжНРДЯДй.^^ ОЦНБАдЕЕ РњДТ 11Пљ 28РЯ ДыЧбРЇОЯЧаШИ ДйЧаСІ С§ДуШИПЁ ТќМЎЧЯСі ИјЧеДЯДй. СњЧтЛѓЧаШИЖѓДТ QI ЧаШИПЁ ТќМЎЧиОп ЧЯБт ЖЇЙЎРдДЯДй. СІАЁ ОјДѕЖѓЕЕ ПЉЗЏКаВВ РЇОЯЧаШИ С§ДуШИ ТќМЎРЛ УпУЕЧеДЯДй. РЬЧѕ БГМіДдРЬ ДйЧаСІ С§ДуШИ ДуДч РЬЛчРЬНЪДЯДй. ЛчРќ ЕюЗЯРЛ ЧЯИщ РњГс НФЛчЕЕ СиКёЕЧДТ АЭРИЗЮ ОаДЯДй. РЬЕП НУАЃ 1НУАЃРЛ ХѕРкЧЯИщ ЧГМКЧЯАд ЙшПя Мі РжНРДЯДй. РкНХРжАд УпУЕЧеДЯДй.
ДыЧбРЇОЯЧаШИ KGCA ШЈЦфРЬСіПЁМ ЛчРќ ЕюЗЯЧв Мі РжНРДЯДй.
ITP ШЏРкРЧ РЇРќР§СІМњ (МКДСЖ) log-in щЉ
New ascites in AGC on chemotherapy (ЧќРчПј) log-in щЉ
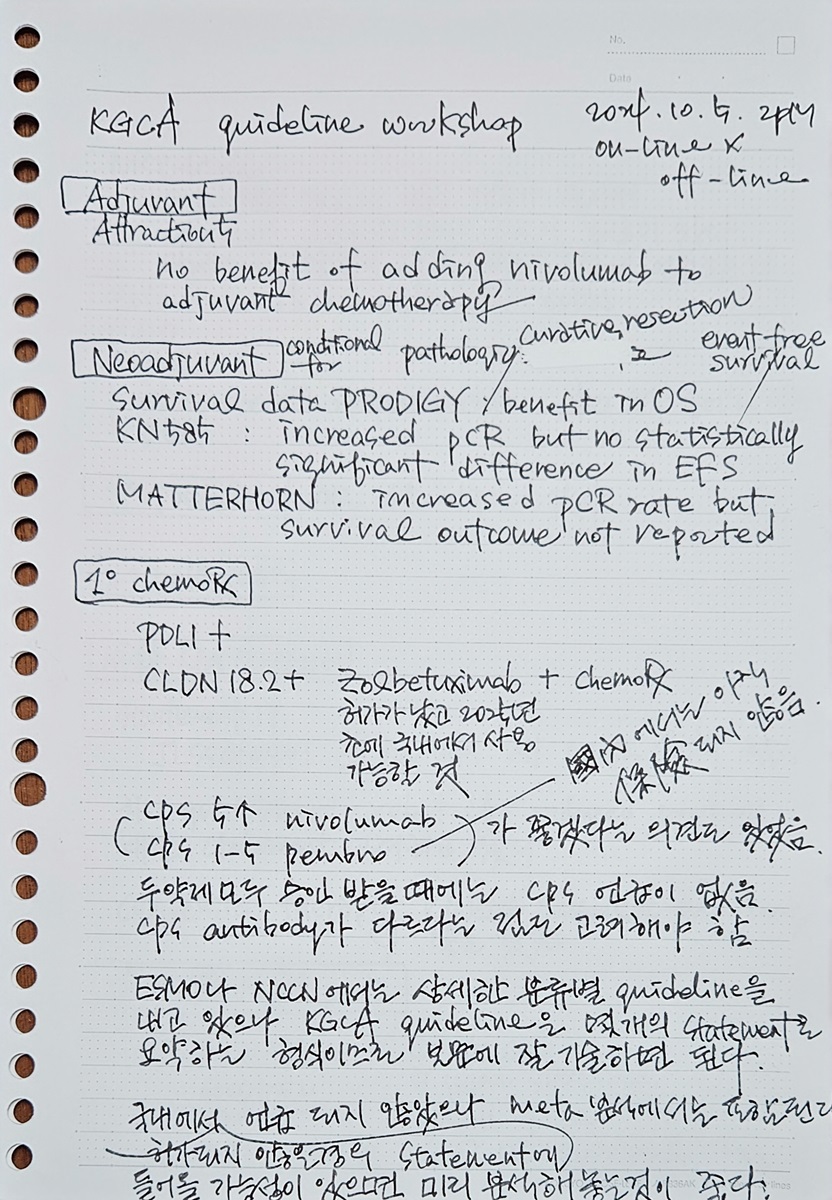
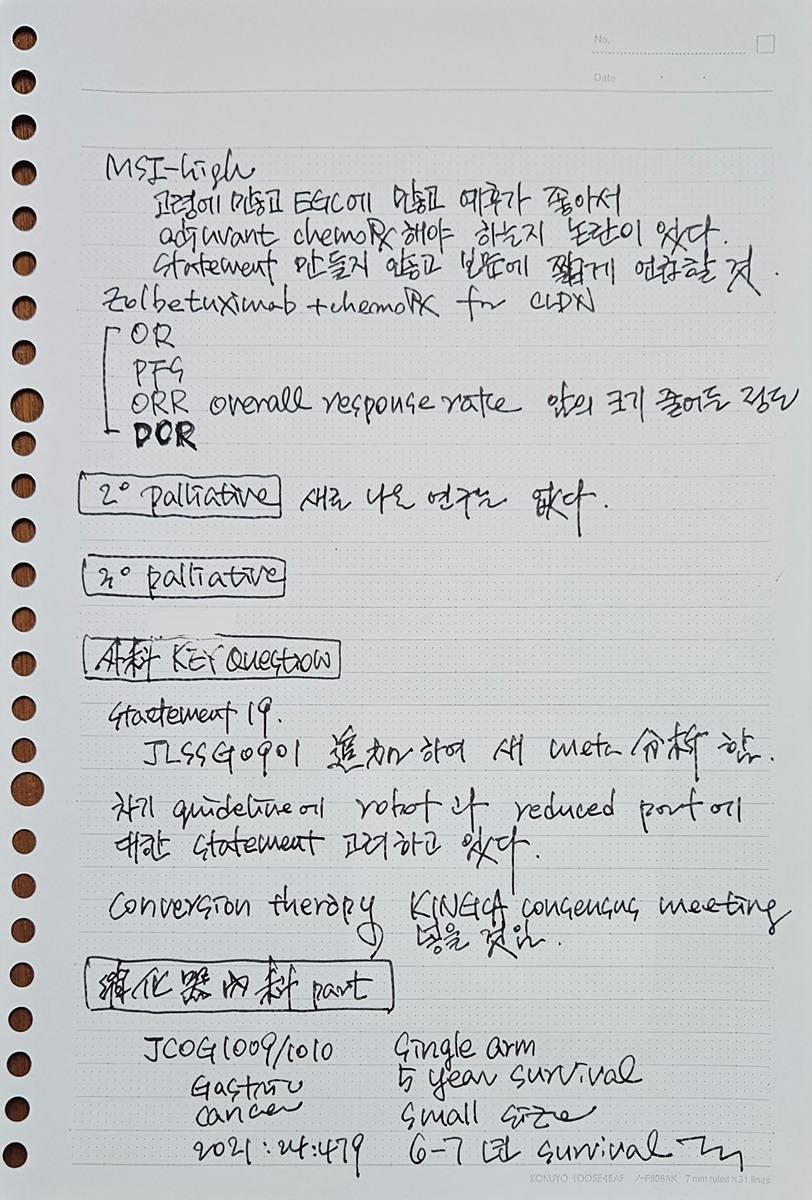
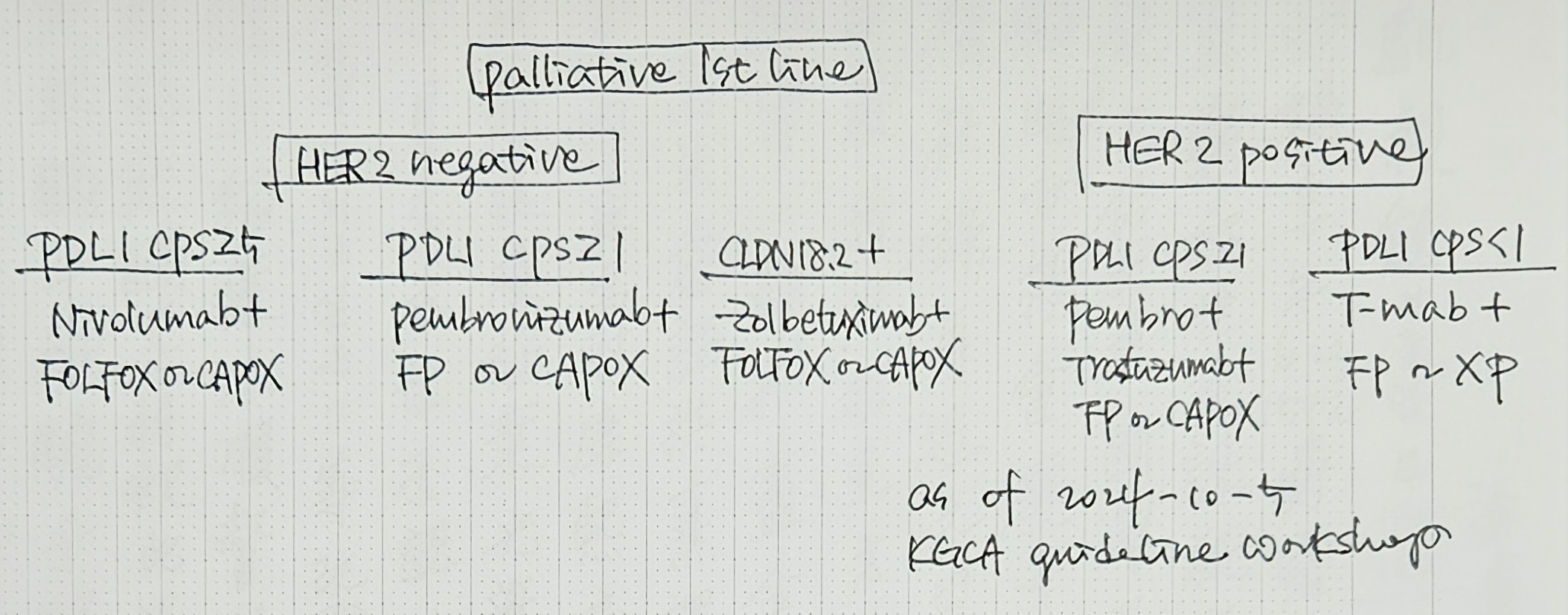
[2024-10-5] KGCA guideline symposium. ЧзОЯФЁЗсКЮКаРЧ ЛѕЗЮПю ПЌБИЕщРЬ ИЙОЦМ РЬИІ ЙнПЕЧЯПЉ КЮКаРћРИЗЮ updateИІ АшШЙЧЯПДБтПЁ АГЙпРк СпНЩРЧ symposiumРЛ ЧЯПДНРДЯДй.
[2024-9-26] KINGCA 2024 ШИРхРИЗЮМ СјЧрЧб KINGCA WeekПДБтПЁ ГВДйИЅ АЈШИАЁ РжОњНРДЯДй.

СЄШЦПы БГМіДдАњ ЧдВВ СТРхРЛ КИОвНРДЯДй.

KINGCA 2024 wrapup
[2024-8-3] KGCA ГЛНУАц Йз КЙААц hands-on symposium
[2024-5-23] KGCA ДйЧаСІ С§ДуШИ
АЃРќРЬШЏРк ЧзОЯФЁЗс ШФ МіМњ (БшЕПСј) log-in щЉ
ШЃШэАяЖѕРИЗЮ ГЛПјЧб РЇОЯ ШЏРк (БшХТММ) log-in щЉ
[2024-4-20] ДыЧбРЇОЯЧаШИ РЇОЯ ШЏРк ЛюРЧ Сњ ПЌБИШИ УсАш ЧаМњДыШИ (СпОгДыЧаБГ БЄИэКДПј 5Уў БшКЮМЗШІ)
[2024-3-23] РЇОЯЧаШИНЩЦїСіОі (ЬдёЖ)
ШИРх РЮЛчИЛ
УЙ МММЧ ГыЦЎ
ШЋИХШ
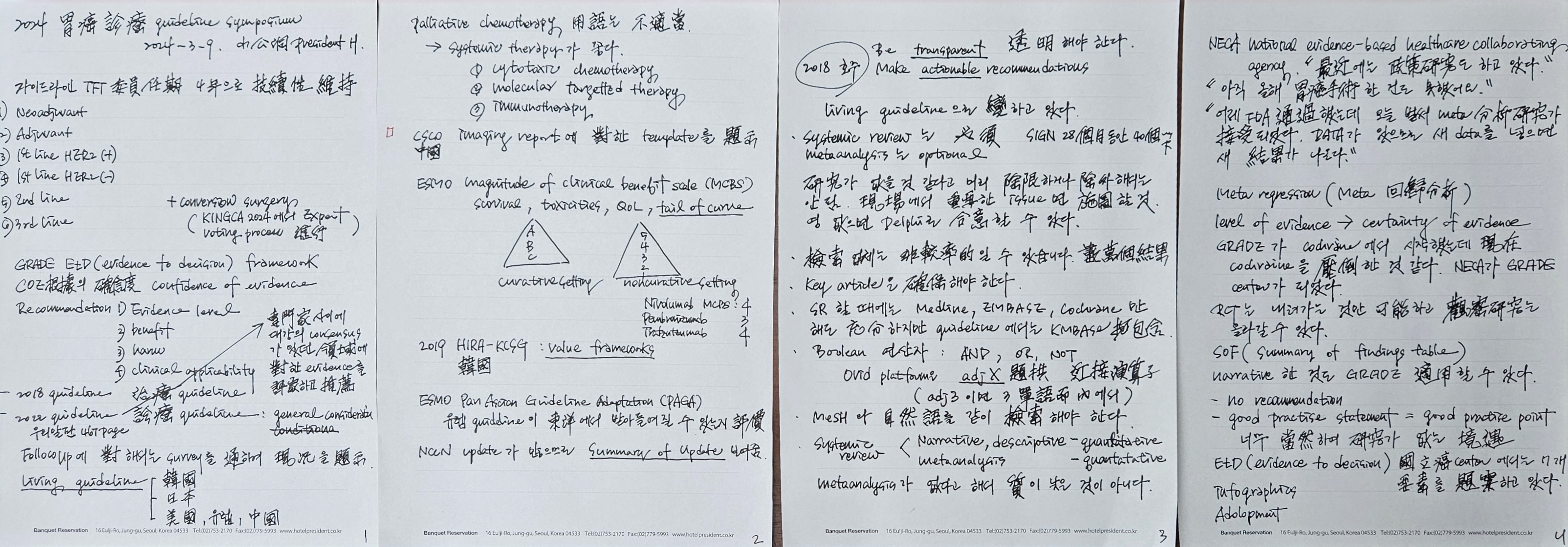
[2024-3-9] АЁРЬЕхЖѓРЮ НЩЦїСіОі. ШИРх РЮЛчИЛ, ГыЦЎ
[2024-1-19] ЧаШИЙпРќММЙЬГЊ (КЮЛъ АэНХДы)
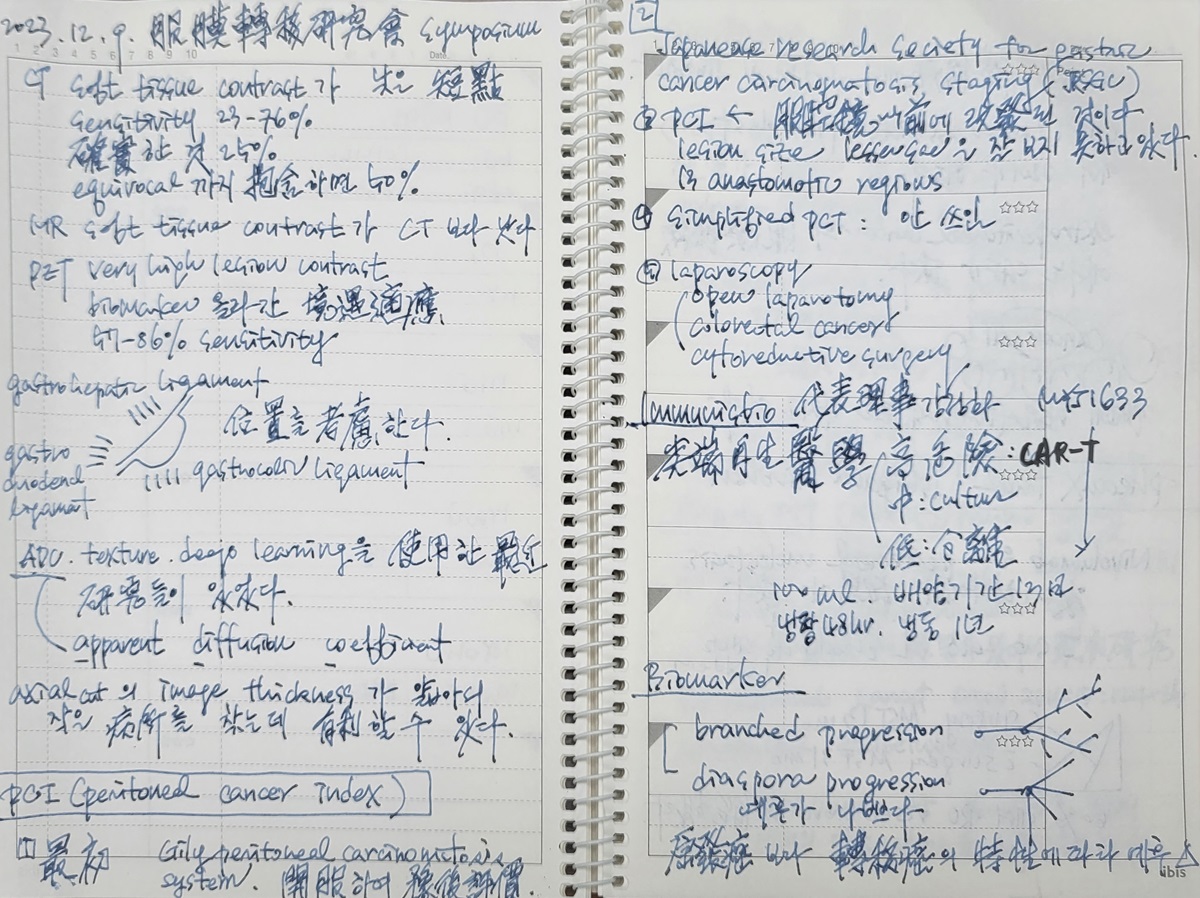
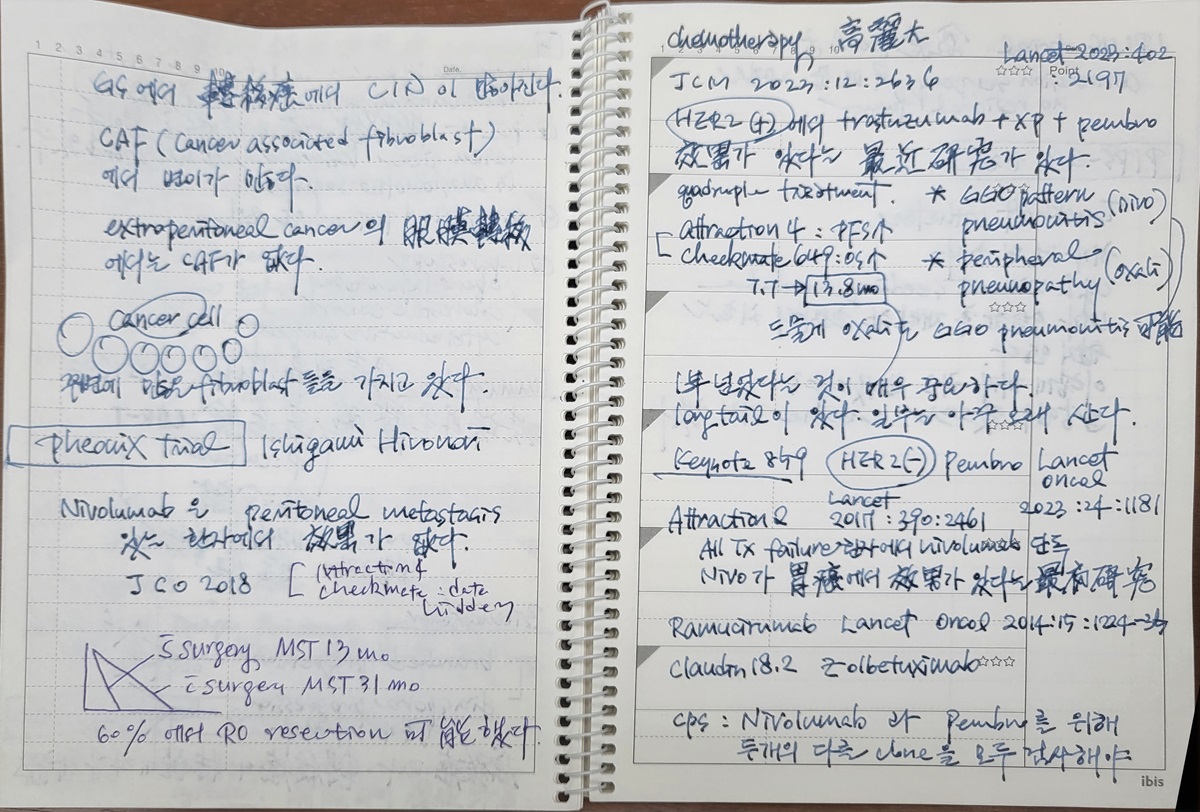
[2023-12-9] РЇОЯКЙИЗРќРЬПЌБИШИ НЩЦїСіПђ (БИЗЮ АэЗСДыКДПј)
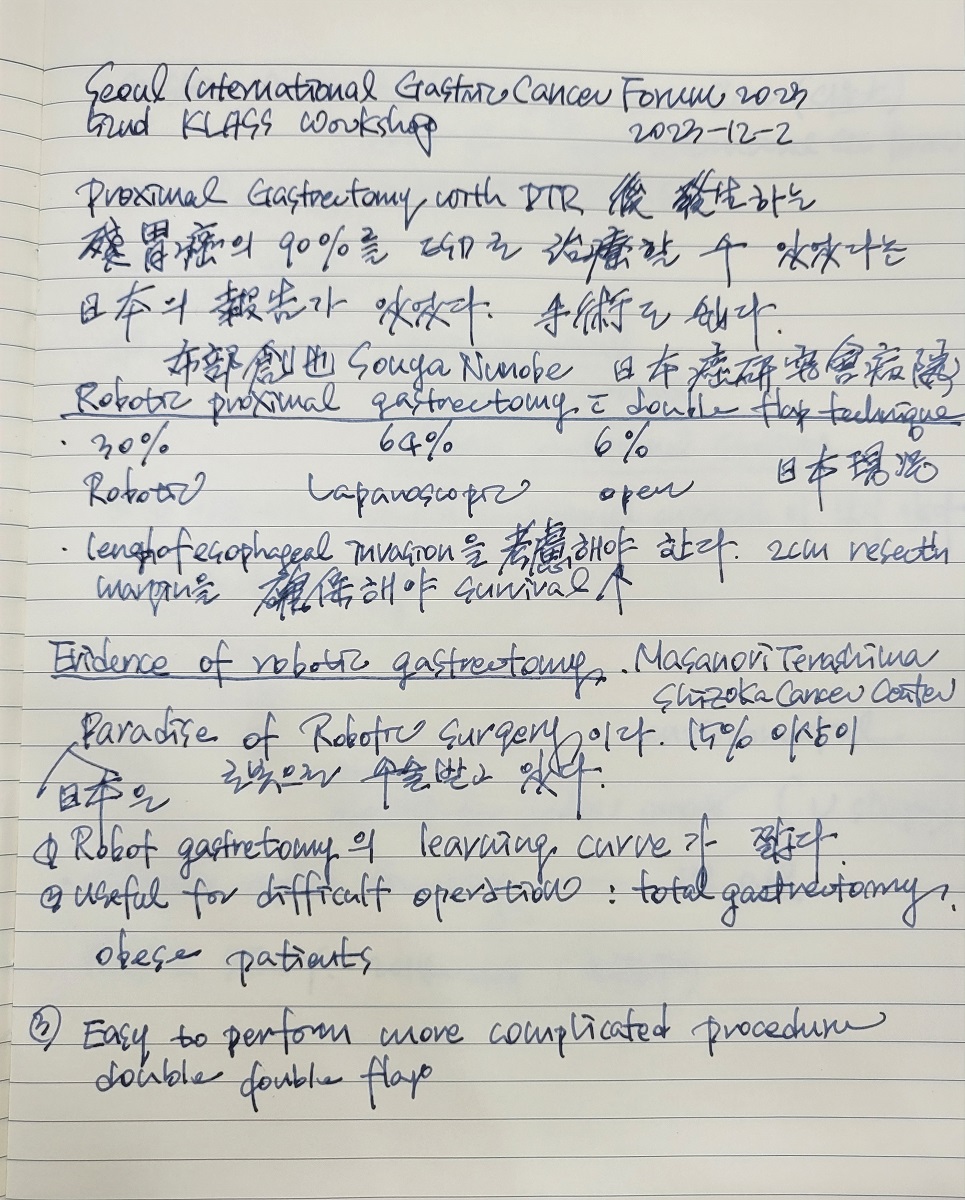
20231202 БЙСІРЇОЯЦїЗГ (МПяДыКДПј)
[2023-11-23] ДйЧаСІ С§ДуШИ ДйНУКИБт
20230914-6 KINGCA (Lotte Hotel)
Satellite symposium
20230304 ДыЧбПмАњРЇРхАќГЛНУАцМіМњПЌБИШИ УсАшНЩЦїСіОі.
20230218 РЇОЯПЌМіАСТ (ПЉМі) - ОШГЛЦїНКХЭ, memo
20221203 Seoul International Gastric Cancer Forum 2022
20220901-3 KINGCA2022 (МіПјФСКЅМЧ МОХЭ)
20200804 KINGCA2020 (МПяЗдЕЅШЃХк)
20190411 KINGCA2019 РЮУЕ МлЕЕ - master class
20181005 СІ2ШИ РЇРхАќПмАњ ПЌАќ ЧаМњДыШИ (КаДч ЧяНКФЩОю ЧѕНХЦФХЉ 4Уў ЙЬЗЁШІ)
20180623 The Second Korea-Mongolia Joint Symposium on Gastric Cancer ИљАэ, ИљАё
20180426 ДыЧбРЇОЯЧаШИ KINGCA (МПя ПіФПШњШЃХк)
20171209 ДыЧбРЇОЯЧаШИ РгПј ПіХЉМѓ
20171021 GERD academy (ПыЛъ dragon city)
20170323 KINGCA 2017 (КЮЛъ Bexco)
20170308 РЯКЛРЇОЯЧаШИ (Hiroshoma)
20160910 ДыЧбРЇОЯЧаШИ ПЌМіАСТ 2016 (РќКЯДыЧаБГ)
20160421 KINGCA 2016 (МПя ЗдЕЅШЃХк) - РЬСиЧр БИПЌ ЙпЧЅ (undifferentiated EGC)
20150402 KINGCA 2015 (СІСж)
20140515 KINGCA 2014 (ДыРќ)
20140321 РЯКЛРЇОЯЧаШИ (Yokohama)
20130426 ДыЧбРЇОЯЧаШИ 34ШИ ЧаМњДыШИ (ДыБИ)
20130425 ДыЧбКЙААцРЇРхАќЧаШИ ПЌМіАСТ
[References]
© РЯПјГЛНУАцБГНЧ ЙйИЅГЛНУАцПЌБИМв РЬСиЧр. EndoTODAY Endoscopy Learning Center. Jun Haeng Lee.









{kind=link}
{kind=link}