EndoTODAY ���ð� ����
EndoTODAY ���ð� ����
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [�����ð� �պ��� (õ�� �̿�)] - ��
[�����ð� �պ��� (õ�� �̿�)] - ��
�����������ð� ���� �پ��� �պ����� �����մϴ�. ���� õ���� ���� �߿��� �պ����Դϴ� (EndoTODAY õ��). õ�� �̿��� �պ��� �� ������ �Ұ��մϴ�.
![]() 1. ���
1. ���
���ð� �˻�� ����� �ʷ��� �� �ִ� ������ �ü��Դϴ�. �� �����սô�.
���༺ �ĵ���. CCRT�� ������ progression�Ͽ��� ���� ���� ���ð� ���� ���ڱ� �뷮 ������ �ϸ鼭 arrest�� ���Ͽ���. CPR�� �Ͽ����� ����� �������� ���
![]() 2. TM joint dislocation
2. TM joint dislocation
���� ȯ�ڿ��� ���ð� �˻糪 �ü� �� ���� ���� �����ϴ�. ������ Ż���� ȯ�ڴ� ������ reduction�� �ϱ �մϴ�. ȣ������ ������ ġ���� �ȳ��ϴ� �� �ۿ� �����ϴ�.
* ����: Jaw Dislocation as an Unusual Complication of Upper Endoscop (Case Rep Gastroenterol. 2016)
![]() 3. ���ð� �� CVA
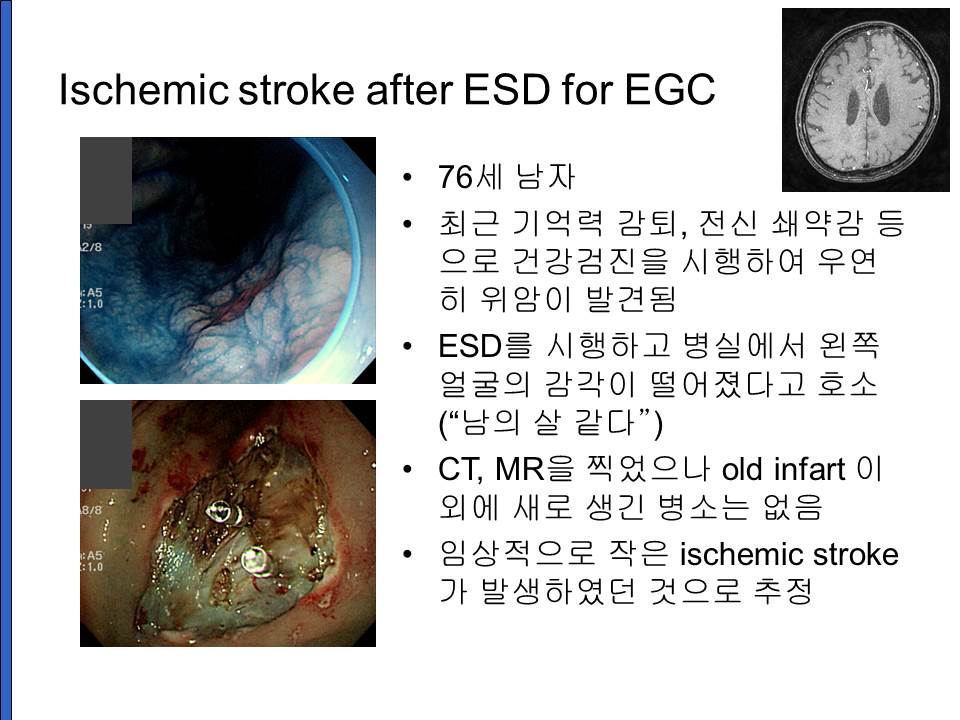
3. ���ð� �� CVA
[2017-10-10. �ֵ��� ����]
�����ǽ��� �� �Ҿƹ����� �Կ����Ͽ� ������ ���ð�ǿ��� �����Բ� ���� ���� ���ð��� (��������) ħ�� �긮�ð� �������� ������ ��Ű�� ���ϰ� ���� �����ٴ� ���Դϴ�. ��¥ ħ�� �� �� ��Ű�ð� ��Ȥ �ݷ��ݷ� ���ε� �ణ�ǽð�.. ��ȣ�ڴ� �ſ� ������ �������� �� ������ 1������ �Ĵٺ��� ��̰� �Ϸ���Ʋ ������ ������ ȣ������ �ʰ�...�ᱹ �������� �ణ �ҿ����� �����������ı��̶�� ������ ã���߰� ȯ�ڴ� ����Ʃ�긦 ���� ��Ȱ�������� ����߽��ϴ�. ���������̶� �ƽ��Ǹ��� ���� Ȥ�� ���� ������ �������� ��̴��� ����� ���� �ʰ� ���ð�� �������� ������ ������ ������� '�ǿ�+��Ȳ'���������̿����ϴ�
[2017-10-10. ������ �亯]
�����������ı��� posterior inferior cerebellar artery Ȥ�� vertebral artery�� ���� ��찡 ���ٰ� �ϴ�... �ƹ����� ���� embolism�̾��� ����Դϴ� (����). ���ð� �� CVA�� ���� �ֽ��ϴ�. ���� 20��° ���ð��� �ϴٺ��� ������ ����� ���ϴ�. ���� ��ﳪ�� �����... �������� ���� ESD�� �ߴµ� ���ǿ� �� ���� ���� ������ �������ٴ� ���Դϴ�. ���� CVA�� �Դ� ���̾����ϴ�. ���ེ���� sequale ���� �� ȸ���Ǽ̽��ϴ�.
History�� �ٽ� �� ����.. ȯ�ڰ� ���� �ൿ�� �������� ���� ��������� ��� ������ �Ҵ� ���Դϴ�. ���������� �����غ��� recurrent small CVA�� �ݺ��Ǹ鼭 multiinfart dementia�� �����ϰ� �־��µ�... �Ű������ ���ܰ� ġ�Ḧ ���� �ʰ� �׳� ���ϴٴ� ������ ������ �Ҵ� �� �ƴѰ� �����˴ϴ�. �̷� �� �� �����ϴ�. �ǰ��� ����� �ƾ� �� �˻縦 ������ �ִ� ����� �Ҵ� ��������. ���� �������� �������� ���ܵǾ� �Ƿڵ� �е��� �Ű����� ������ ������ ���� �����ϰ� �ֽ��ϴ�. ������ �����̳� physical examination �ѹ� ���� �˻縸 ��û ���� �ϴ� ���� ���� �����Դϴ�. ��ô ��������.
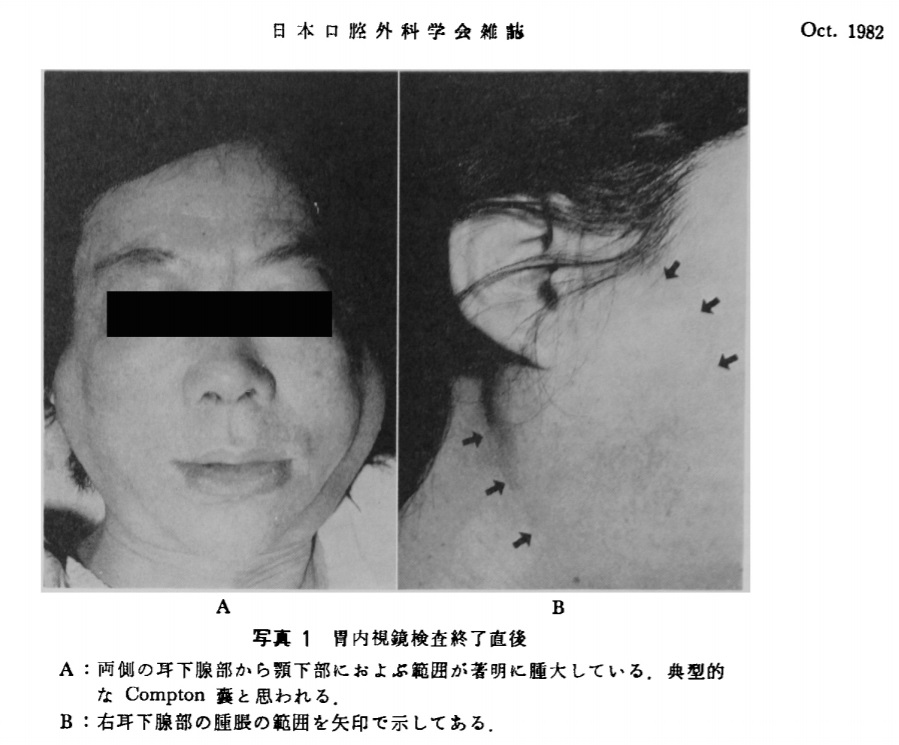
![]() 4. �ϰ��� Ÿ�� ��â (transient sialoadenopathy, Compton's pouch)
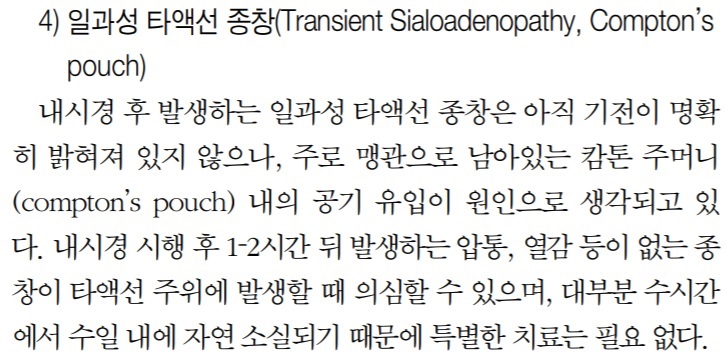
4. �ϰ��� Ÿ�� ��â (transient sialoadenopathy, Compton's pouch)
Compton's pouch �� ������ ���ؼ��� ���� ������ �����Ͻñ� �ٶ��ϴ�. �Ѹ���� �� �ٴ� �̾߱��Դϴ�. �����ð� �˻� �� ���� �ϰ��� Ÿ�� ��â 2��. ���Ѽ�ȭ�⳻�ð���ȸ�� 1999
![]() 5. Vocal cord palsy
5. Vocal cord palsy
�������� ���ð��� �պ������� ���� ������ ���븶�� 2�� (���Ѽ�ȭ�⳻�ð���ȸ�� 2006;33:32-36)
�� ���ʿ� ���� ����
[2020-5-7. �ֵ��� ����] Crico-arytenoid dislocation
������ ���ǵ�ȴ� �����ڰ� EGD ���� ������ �� ����Ҹ� ���ӵǾ� local ENT���� ������ ���븶�� �ǽɵȴٰ� �ߴ� �� ������ ENT �����Բ� ���ǵ�Ⱦ��µ���... ��� �Ʒ� ÷���մϴ�.
"��ȭ�� ���ð� ���� �߿� ������ ���������� ����ϰ� �ִ� �ǿ�-���� ���� (crico-arytenoid) �̶�� �κп� ������ ����� ���� Ż��(dislocation or subluxation)�� �Ǵ� ��찡 �幰�� �ʰ� �ֽ��ϴ�. �� ��� ������ �������� �������� ������ ���븶����� ������ ���� �ʽ��ϴ�.
���볻 �ұ����� ������ �˻�� �Ű渶�� ���ٴ� ���� Ȯ���� ���� Ż���� �������� ���Ÿ����Ͽ� �õ��ϰ� �˴ϴ�. �������� �� ����Ǿ ���� �������� ȸ���Ϸ��� �� 1���� �Ѱ� �ʿ��մϴ�. �������� �ܻ� �� ���� ������ ���� ���İ� ������ �ܻ� 1�� ���Ŀ��� ����Ȯ���� �������ϴ�."
���� �̷� ��츦 ó�� ��ð� �� ���� ������, ENT�����Բ����� �幰�� �ʰ� �ִٰ� �ϼż� �� ����̾����ϴ�. �ĵκ��ô� ENT �������� ���� �̷� ���̽��� ���� �� ������, ���� ���ð� ��ȸ�� �������¿����� �̿� ���� ���� �� ���� �����ϴ�.
Ȥ�� �����Բ��� ��ȸ�� �ǽŴٸ� �ĵκ��ô� ENT������ �̷� �κе鿡 ���ؼ� ���� ���ð� �ǻ���� �� �Ѿ�� ������ ���̽��� �� �Ǵ���, EGD�� �ĵθ��� crico-arytenoid�� dislocation�� �����Ϸ��� ��� �ϴ°� �ּ�����, �̷� �������� risk factor�� � ������ �� ���� �ѹ� �ǰ��� ��ȯ�� ���ô°� ��� ���ɽ����� ��Ź������ϴ�. �ƹ����� ���ð� �ǻ��� ������ ������ ���ð� �ǻ��� EGD �� ��������� ���� �� �ִ� �պ����� ���ؼ� �˰� �־�� ������ ������ �� �����ϰ� ������ ��ġ�� ���� �� ���� �� ����, ���ð� ���Ǽ� ��� ���� ������ ���Խ��Ѿ� ���� ������ ���� ������ ��ϴ�.
�ƿ ���� �̷� ���� ������ ENT�������� �ǰߵ��� EndoTODAY ���ڵ�� �����ϸ� ������ �ͽ��ϴ�.
�ȳ��� ��ʽÿ�.
[2020-5-7. ������ �亯]
���� ���� �����մϴ�. ���� �� �־����ϴ�.
ª�� �˻��� �� ���� GI endoscopy ���ٴ� endotracheal intubation �̾߱Ⱑ ��κ��̾����ϴ�. ���� GI endoscopy�� ����� ����(Journal of Laryngology and Voice 2017:7:43)�� �ֱ�� �߽��ϴ�. �Ʒ� ����ϴ�.
Arytenoid dislocation is one of the complications encountered during laryngeal and esophageal procedures such as endotracheal intubation, laryngeal mask airway insertion, gastrointestinal endoscopy and transesophageal endoscopy probe placement. Traumatic insertion of laryngoscope blade, prolonged and/or difficult intubation, overzealous use of lighted stylet intubation, or extubation with partially deflated cuff were reported as the causes of arytenoid dislocation. Endotracheal intubation is a common cause of arytenoid dislocation and it results in hoarseness, aphonia, and dysphagia. Early identification and treatment leads to arytenoid motion restoration and improvement in voice. Treatment varies between spontaneous resolution, speech therapy, and closed reduction through direct/indirect laryngoscopy."
Arytenoid subluxation�̶�� ������ �� �� �ڼ��� ������ �Ϻθ� �ű�ϴ�.
"Arytenoid subluxation is partial displacement of the arytenoid cartilage within the cricoarytenoid joint. It is a rare complication that typically occurs after a traumatic injury to the cricoarytenoid junction during laryngoscopy and intubation, upper airway instrumentation, and external laryngeal trauma. The arytenoids are a pair of small pyramid-shaped cartilages which articulate with the cricoid cartilage at the cricoarytenoid joint. Both the arytenoids and cricoarytenoid joints are relatively fragile and very vulnerable to injury during laryngoscopy and intubation. Clinicians commonly visualize the bulge in the mucosal surface overlying the arytenoids during laryngoscopy.
The arytenoids are composed of an apex, a base, and two processes (vocal and muscular). The vocal processes extend anteriorly and provide attachment to the vocal ligament, and are responsible for tension, relaxation, or approximation of vocal folds, while the muscular processes extend posterolaterally and provide a point of insertion for the lateral and posterior cricoarytenoid muscles. These muscles are responsible for opening and closing the glottis by creating lateral and medial movements of the attached vocal cords. The apex articulates with the aryepiglottic fold and corniculate cartilages, and the base articulates with the cricoid cartilage through several ligaments that form the capsule of the synovial cricoarytenoid joint. The cricoarytenoid joint controls the abduction and adduction of the true vocal cords, allowing respiration, phonation, and airway protection.
One often sees the terms subluxation and dislocation used interchangeably. However, a dislocation refers to a complete separation of the arytenoid cartilage from the joint space, whereas a subluxation is partial displacement of the arytenoid within the joint. Both can be considered the same disease with varying degrees of severity, sharing the same pathophysiology. A subluxation can be classified as anterior when the displacement is anteromedial or posterior when the displacement is posterolateral.
Arytenoid subluxation is usually related to acute traumatic events to the cricoarytenoid junction. Protrusion of an endotracheal tube stylet, an unanticipated difficult airway leading to prolonged or traumatic intubations, the use of a gum elastic bougie, blind intubation techniques (e.g., utilization of a lighted stylet or light-wand) and insertion of bulky double-lumen tubes, have all been implicated. The degree of experience of the laryngoscopist, dental malocclusion, retrognathia, and a large tongue may also play a role. There are also reports of severe cough and even spontaneous arytenoid dislocation.
Several systemic diseases, as well as chronic corticosteroid use, laryngomalacia, and acromegaly may lead to the weakening of the cricoarytenoid joint capsule, thus exacerbating this complication. An elevated BMI might be an independent risk factor, and major cardiac surgery involving the use of transesophageal echocardiography (TEE) probe may also be a possible explanation for the increased incidence.[15] Insertion of the TEE probe is the likely inciting event in these cases.
The incidence of arytenoid subluxation after endotracheal intubation has been reported to be between 0.01% and 0.1%. Although the reported incidence suggests that it is rare, the true incidence may be higher. Rudert et al. reported a much higher incidence of 30% in his case series of patients referred to him with prolonged hoarseness following instrumentation of the larynx; 80% to 90% of all cases were related to intubation trauma.
���� ó�� ��� �պ����̰� ���忡���� GI endoscopy���ٴ� tracheal intubation�� �� �������� �Ǿ� ������, �ĵο� �ĵ��� ������ ����̰� �����ð��� �ϸ鼭�� tracheal intubation �� ��찡 ���� ������ �����ϸ� crico-arytenoid dislocation�� GI endoscopy�� �幮 �պ����� �� �� ���� �� �����ϴ�.
���ð��� �پ��� �պ����� ���� �� �����Ƿ� �ſ� serious�� �µ��� �����ؾ� �ϴ� �ü��Դϴ�. �ǻ糪 ȯ�ڳ� ������ å���ϴ� ���� �籹�ڳ� ��� serious�ؾ� �մϴ�. �׳� ������ ���� �� �� �ִ� ������ �˻簡 �ƴմϴ�. ����� ������ ����� �Ʒð� ����� ������ġ�� �� �� ���¿��� ����� �ð� ���� õõ�� õõ�� ����Ǿ�� �����մϴ�.
* ����: Korean J Anesthesiol 2016
* ����: Dislocation of the cricoarytenoid joint: diagnosis and therapy Laryngorhinootologie. 1998
![]() 6. ġ�� �ջ�
6. ġ�� �ջ�
�����ð� �� mouthpiece�� ����մϴ�. ȯ�ڰ� ����ġ�� ���� �ִ� ��� incisor teeth�� �ջ��� ���� �� �ֽ��ϴ�. ���� ���ð��� ��� �ڱ �� ���Ѱ� ���� ��찡 �־ �� �� ���� �������� �� �����ϴ�. ������ ġ�� �ջ����� ġ����� �п��� ġ�� �ջ��� �� �� �����ϴ�. ���Ǽ����� �и��� ����ϰ� ������, ȯ�ںе��� ��Ȥ �Ҹ��� �����մϴ�.
�Ƿ������������� ��ʵ� ���� �ֽ��ϴ�.
������ ���� �����ϰ� ���Ǽ��� ����� ����� �����Ͽ� �ü��Ͽ������� ���� ġ�� �ջ� ���Ͽ� �Ƿ����� ������ �����ϴ� ���� ����� �� �����ϴ�.
![]() [Others]
[Others]
Subcutaneous hematoma of the uvula and soft palate (during EMR-C)
ȯ�ڰ� ������ �ϸ鼭 �Ϻνĵ� ������ �ణ�� �ջ��� �־��� ���� �Ͻ����� ������ �������ϴ�. �̳� ���������ϴ�. "���� �ε巴�� �Ļ��ϼ���"��� ���ǻ��� �帮�� ���� �̿ܿ��� Ư���� ��ġ�� �ʿ��� ��Ȳ�� �ƴ� ������ �����˴ϴ�. (����: ó�� ����, ����: �˻縦 ��ġ�� ���� �� ����)
�������ð� ���� ȯ�ڰ� ������ �����ڰ� ���� �����ϴ� �������� ���� skin abrasion (2015��, 85�� ����)
![]() [References]
[References]
© �Ͽ����ð汳�� �ٸ����ð濬���� ������. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.