EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [식도 점막하종양. Esophageal submucosal tumor (SMT)] - 終
[식도 점막하종양. Esophageal submucosal tumor (SMT)] - 終
![]() 1. Introduction
1. Introduction
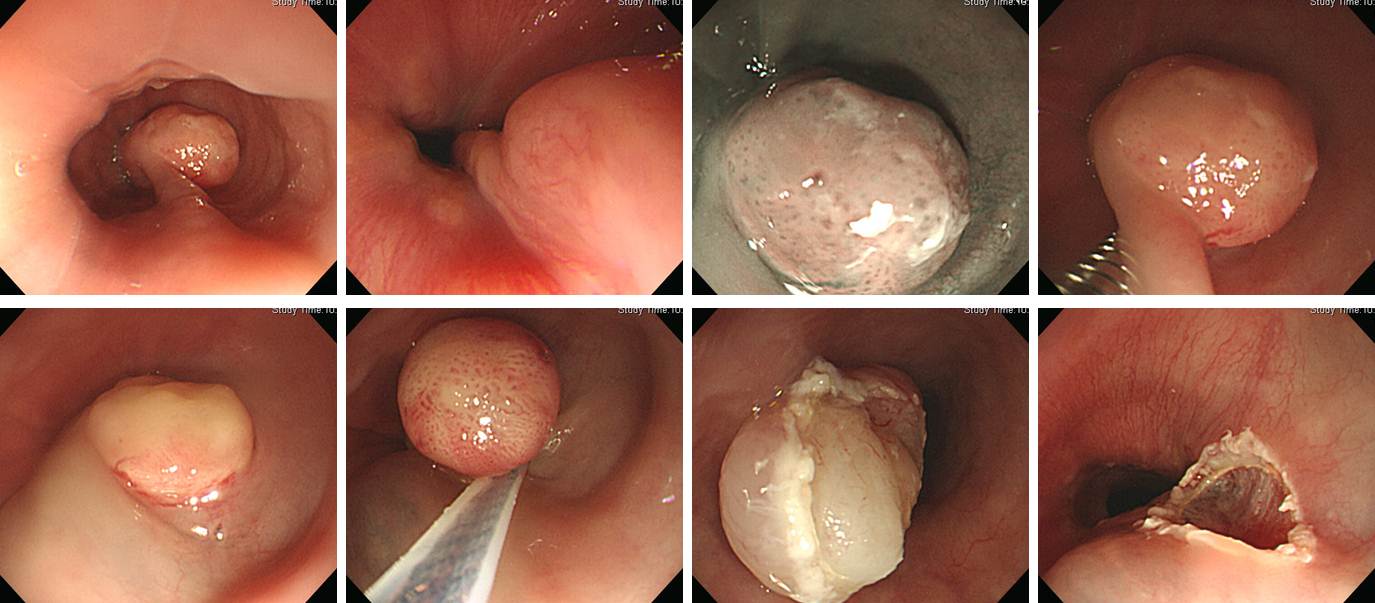
The majority of small esophageal SMTs are benign. When a small esophageal SMT is found for the first time, 1-2 biopsies are sufficient. When the esophageal SMT is smaller than 5 mm, no biopsy may be OK in some cases. If there is no significant change, you don't need to take biopsy in the follow-up.
The most common esophageal SMT is the leiomyoma of the far distal esophagus. They are benign.
r/o esophageal leiomyoma (histology is unavailable).
Most of the biopsies for esophageal SMTs are reported as normal esophageal mucosa. One rare exception is granular cell tumor.
Esophageal granular cell tumor
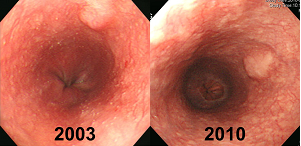
5년 동안 변화가 거의 없는 식도 SMT. 이와 같은 경우 표면에서 forceps biopsy를 반복하는 것은 거의 의미가 없습니다.
![]() 2. Superficial esophageal neoplasm + SMT
2. Superficial esophageal neoplasm + SMT
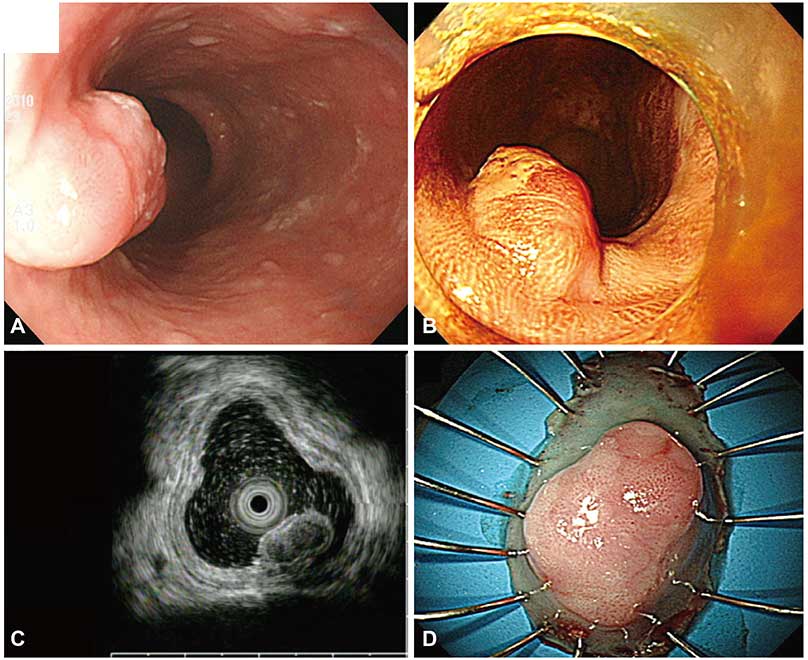
Clinical Endoscopy 2015년 7월호에 식도근종 위에 이형성이 있었던 병소를 내시경으로 치료한 증례 3개가 보고되었습니다 (아산병원. Myeongsook Seo. Clin Endosc 2015).
몇 년 전 저도 거의 비슷한 경험을 하였습니다. 식도 high grade dysplasia라고 오셨는데, SMT 위에 HGD가 위치한 모양이었습니다. 내시경절제술을 하였고 결과는 좋았습니다. 내시경 사진, 병리 사진, 병리 결과입니다.
Esophagus, low, endoscopic mucosal resection :
Squamous dysplasia, high grade:
1) size: longest diameter: 11mm, vertical diameter: 8mm
2) gross type: flat
3) negative resection margins
Leiomyoma
![]() 3. Esophageal SMT due to tuberculosis
3. Esophageal SMT due to tuberculosis
![]() 4. Neuroendocrine carcinoma of the upper esophagus (2016년 6월 10일 SMC 집담회 증례)
4. Neuroendocrine carcinoma of the upper esophagus (2016년 6월 10일 SMC 집담회 증례)
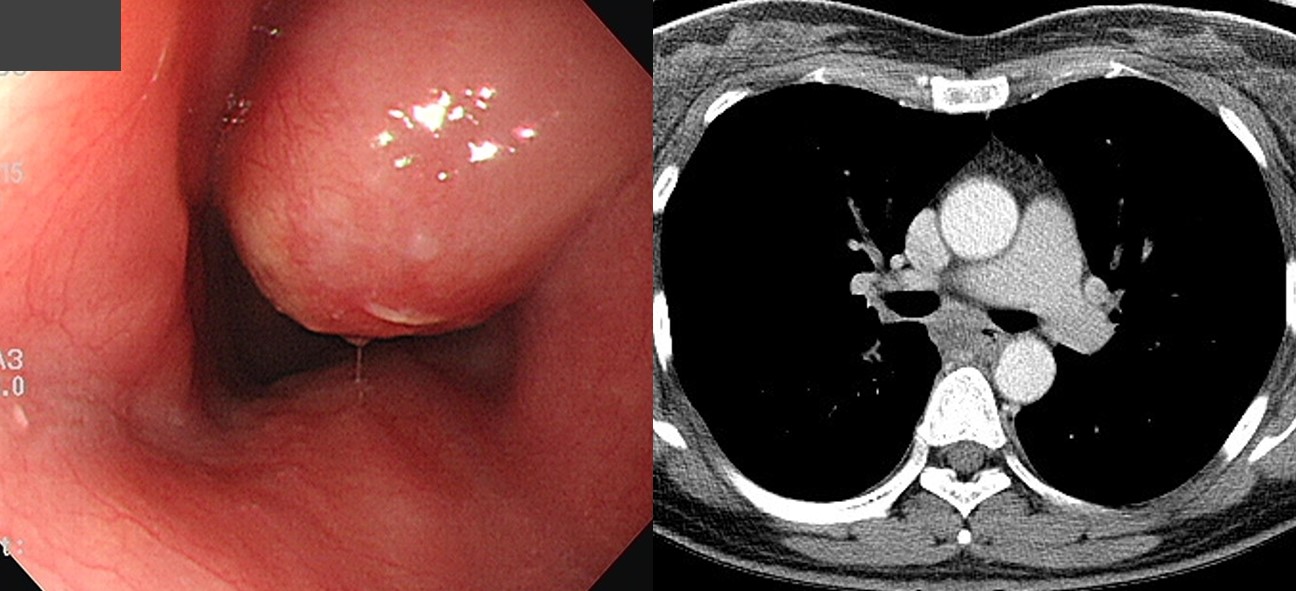
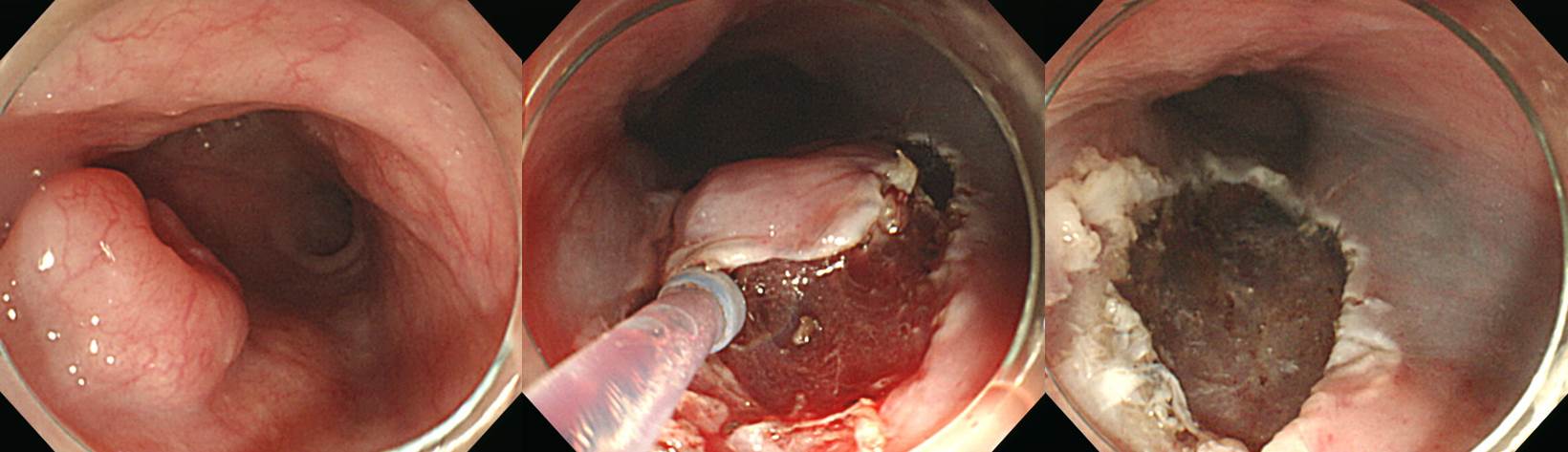
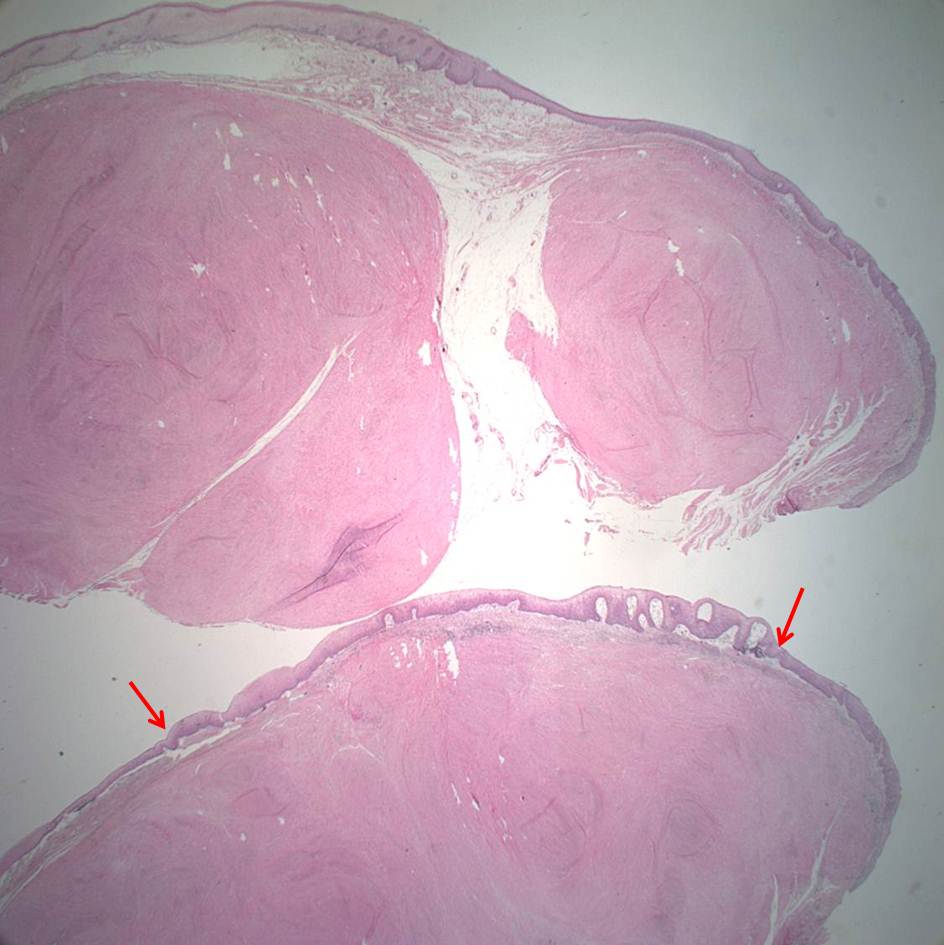
70대 여자가 비특이적 가슴 불편감으로 외부에서 시행한 내시경에서 식도 점막하종양이 발견되어 의뢰되었습니다. 외부슬라이드 재판독 결과는 SCC, M/D with focal neuroendocrine component였습니다. 상부식도 병소인 관계로 수술에 따른 위험성이 높을 것으로 판단되어 흉부외과로부터 내시경 치료가 의뢰되었습니다. ESD는 어려움 없이 시행되었습니다.
ESD 병리결과가 아래와 같았습니다. 수술을 의뢰하였습니다.
1. Diagnosis: Large cell neuroendocrine carcinoma
2. WHO classification(2010): Neuroendocrine carcinoma
3. Size: 0.9x0.8 cm
4. Extent: Mucosa and submucosa
5. Grading: Mitotic Count: >20/10 HPF, Ki-67 labeling index: G3>20%
6. Lymphovascular invasion: Present
7. Perineural invasion: Not identified
8. Resection Margins: Involved by tumor with cautery artifacts
Chromogranin: Positive, Synaptophysin: Positive, CD56: Positive, Ki-67: Positive (60%), PHH-3: Positive (198/10 HPFs)
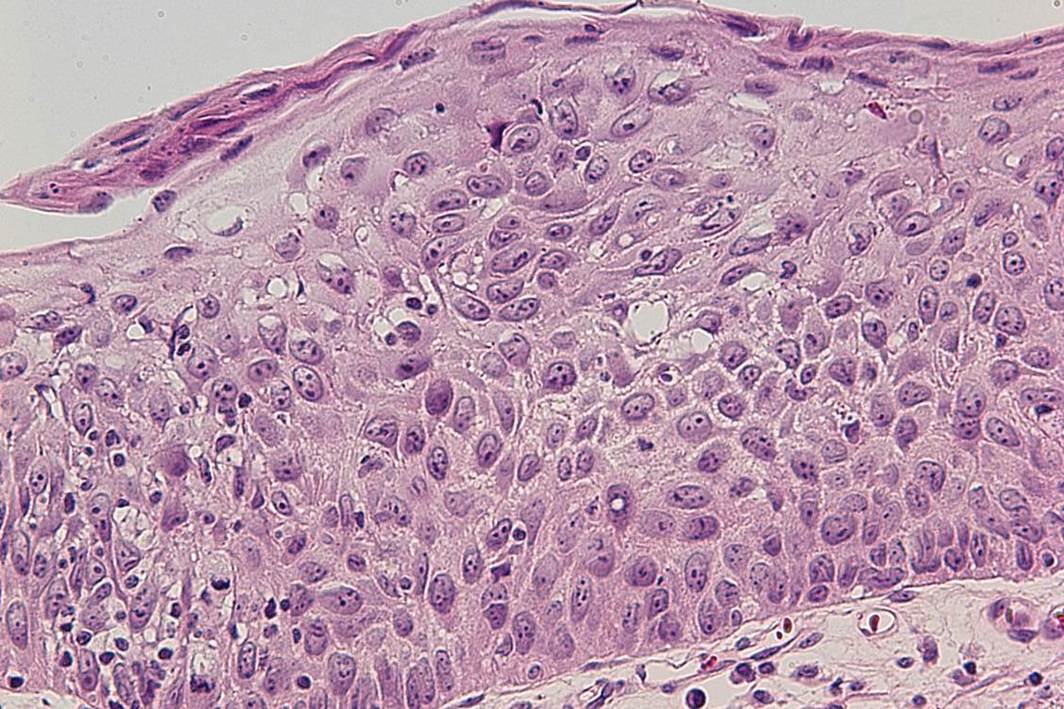
ESD 병리. 점막층은 비교적 intact 한데 그 아래로 homogenous한 신경내분비세포가 넓게 보임
ESD 병리. 뚜렷한 endolymphatic emboli가 관찰되었음.
수술 결과는 아래와 같았습니다.
Esophagus and upper stomach, Ivor Lewis operation:
Status post endoscopic submucosal dissection (D13-7695)
No residual tumor
1) tumor size: cannot be determined (no residual tumor)
2) depth of invasion: cannot be determined (no residual tumor)
3) endolymphatic tumor emboli: not identified
4) perineural invasion: not identified
5) resection margins: free from carcinoma, safety margin: proximal, 1.5 cm ; distal, 18 cm ;
6) metastasis to 1 out of 25 regional lymph nodes (1/25: "LC omentum", 0/0; "G1", 0/3; "G2", 0/3; "G3", 0/8; "RRLN (right recurrent laryngeal nerve)", 1/2; "LRLN", 0/2; "L9", 0/1; "L10", 0/1; "RD", 0/1; "5", 0/1; "7", 0/2; "8u", 0/1)
7) treatment effect: not applicable
수술 병리 (림프절). 림프절에 신경내분비암의 침윤이 있었음.
![]() 5. [case report] 식도 상피하종양으로 오인된 대동맥식도누공
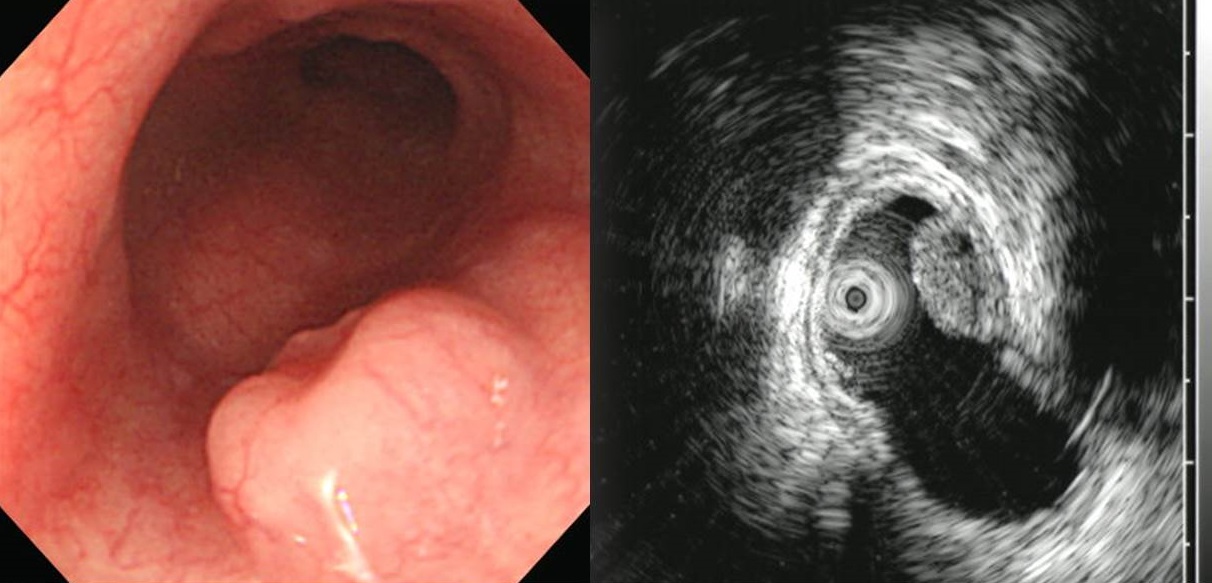
5. [case report] 식도 상피하종양으로 오인된 대동맥식도누공
2026년 증례보고에 실린 사진
![]() [FAQs]
[FAQs]
[2023-5-28] 며칠 전 있었던 KSGE webinar 식도 양성질환을 리뷰했습니다. 실시간을 듣는 것보다 훨씬 효과적입니다. 천천히 다시보기 하면서 공부할 수 있으므로
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Jun Haeng Lee.