 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Introduction to longterm outcome]
[Introduction to longterm outcome]
Thank you very much for being with me at this time of the day. The original topic was “treatment strategy and limitations of standard ESD”, but I slightly changed it into “treatment strategy based on long-term outcome data.”
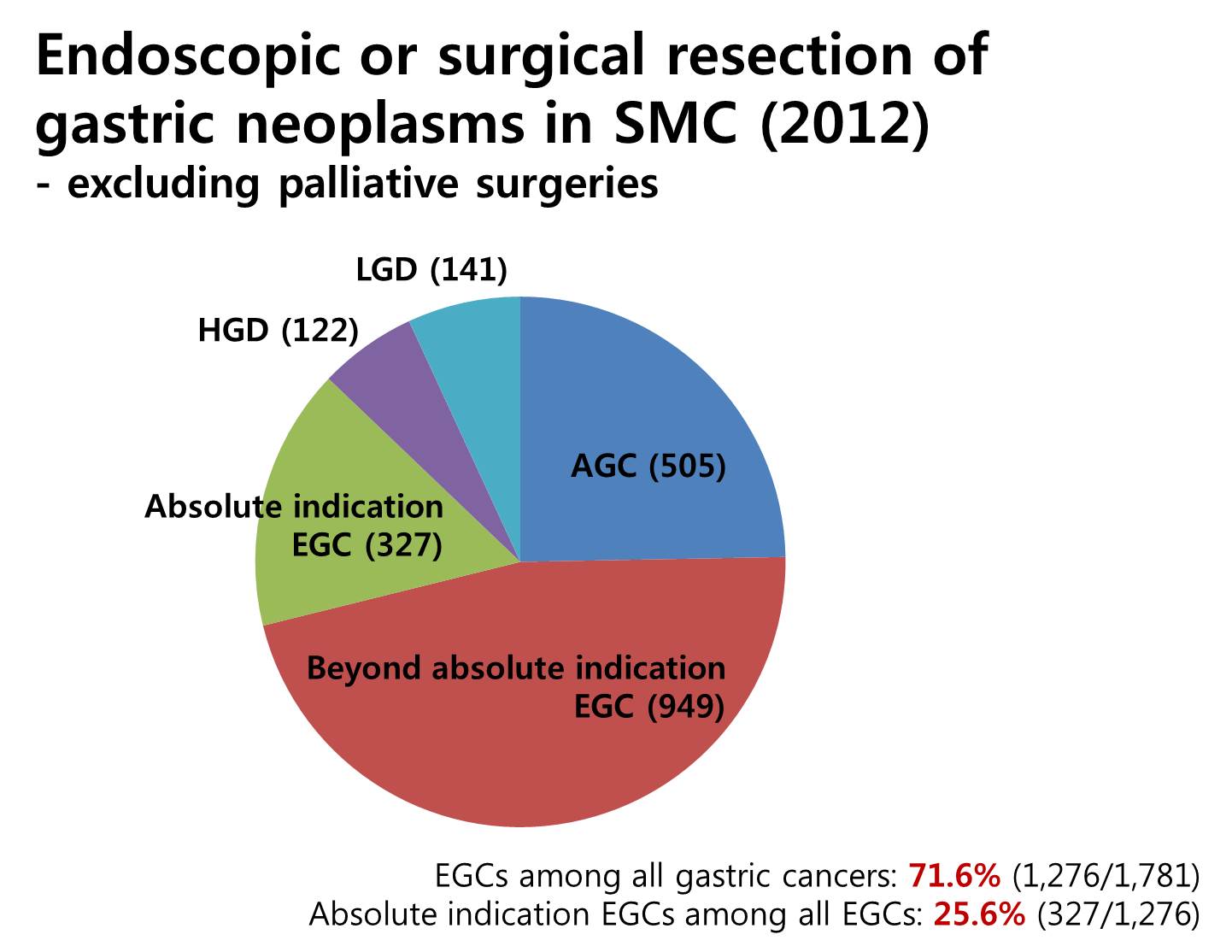
As you know, the proportion of early gastric cancer is increasing. This is how we are doing in my institution. Excluding palliative surgeries, we have endoscopically or surgically treated more than seventeen hundred gastric cancers in 2012. Among them, 72% were early gastric cancers. In early gastric cancers, cases within absolute indications were 25%. So the role of ESD for the treatment of gastric cancer is getting bigger and bigger.
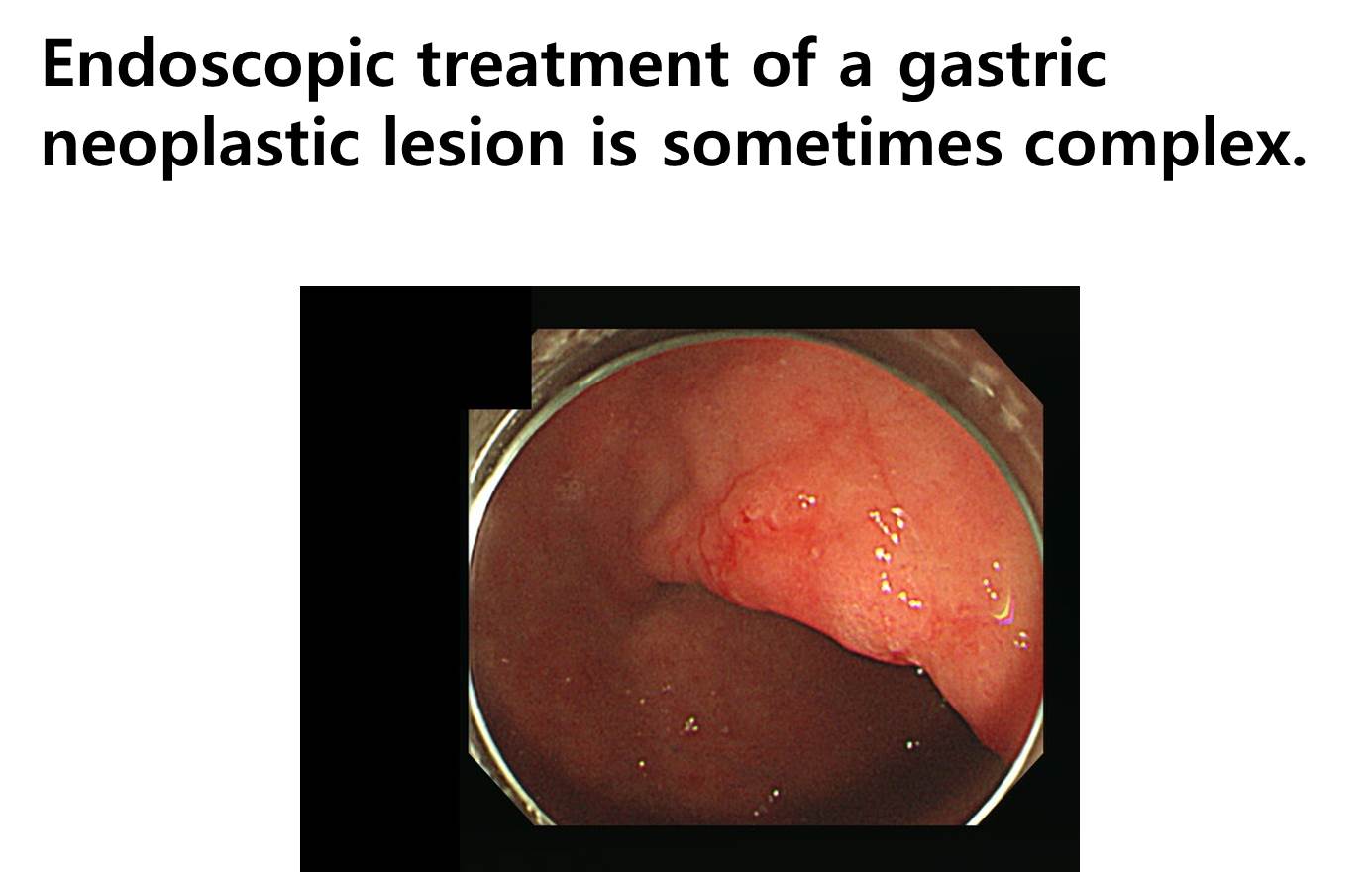
Endoscopic treatment of a gastric neoplastic lesion is sometimes complex, so the evaluation of the outcome is not straightforward. I’ll start with an interesting case. The treatment course was complicated but the final outcome was good.
I’d like to split my discussion into three topics. First, lessons from oncology about outcome analysis. Second, long-term outcome of ESD for EGC at my institution. Third part will be “learning from endoscopic pictures”. I prepared a lot of endoscopic images for you. I hope you enjoy them.
![]() First of all, I will discuss what we can learn from oncology about outcome analysis.
First of all, I will discuss what we can learn from oncology about outcome analysis.
What do you think is the best way of presenting long-term outcome data? There are two types of outcome analysis - one is intention to treat analysis, and the other is per protocol analysis. Of course, data from intention to treat analysis is more realistic. In the survival analysis, the rate of follow-up loss is very important. It should be minimalized, usually less than 15 percent in prospective clinical studies.
![]() Let’s consider the intention to treat analysis first.
Let’s consider the intention to treat analysis first.
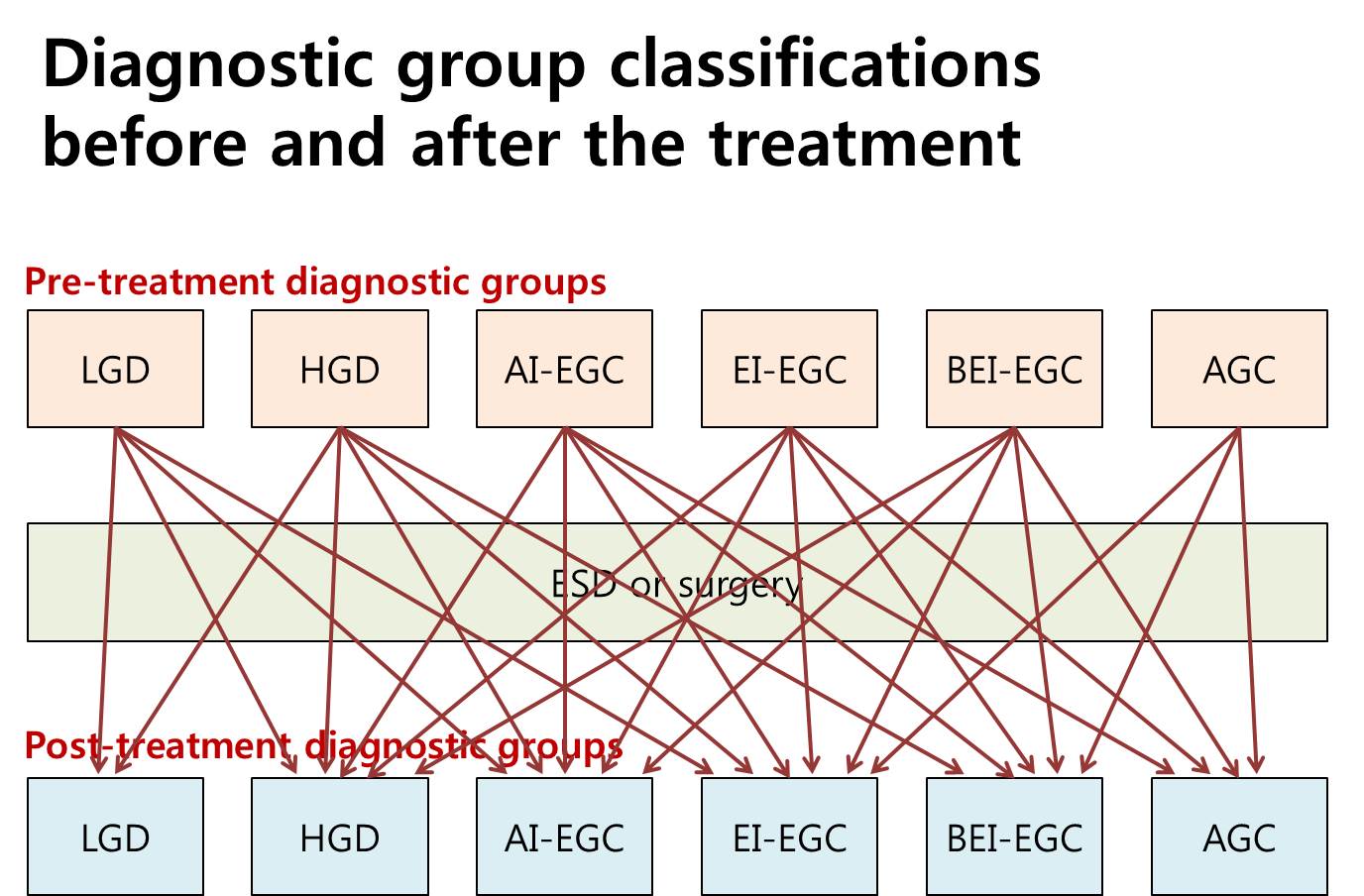
Gastric neoplastic lesions can be divided into 6 groups, such as LGD, HGD, AI-EGC, EI-EGC, BEI-EGA and AGC. Diagnostic group classifications before the treatment can be changed after the treatment. The relationship is very complex. So the outcome analysis can be based on either pretreatment diagnostic groups or posttreatment diagnostic groups.
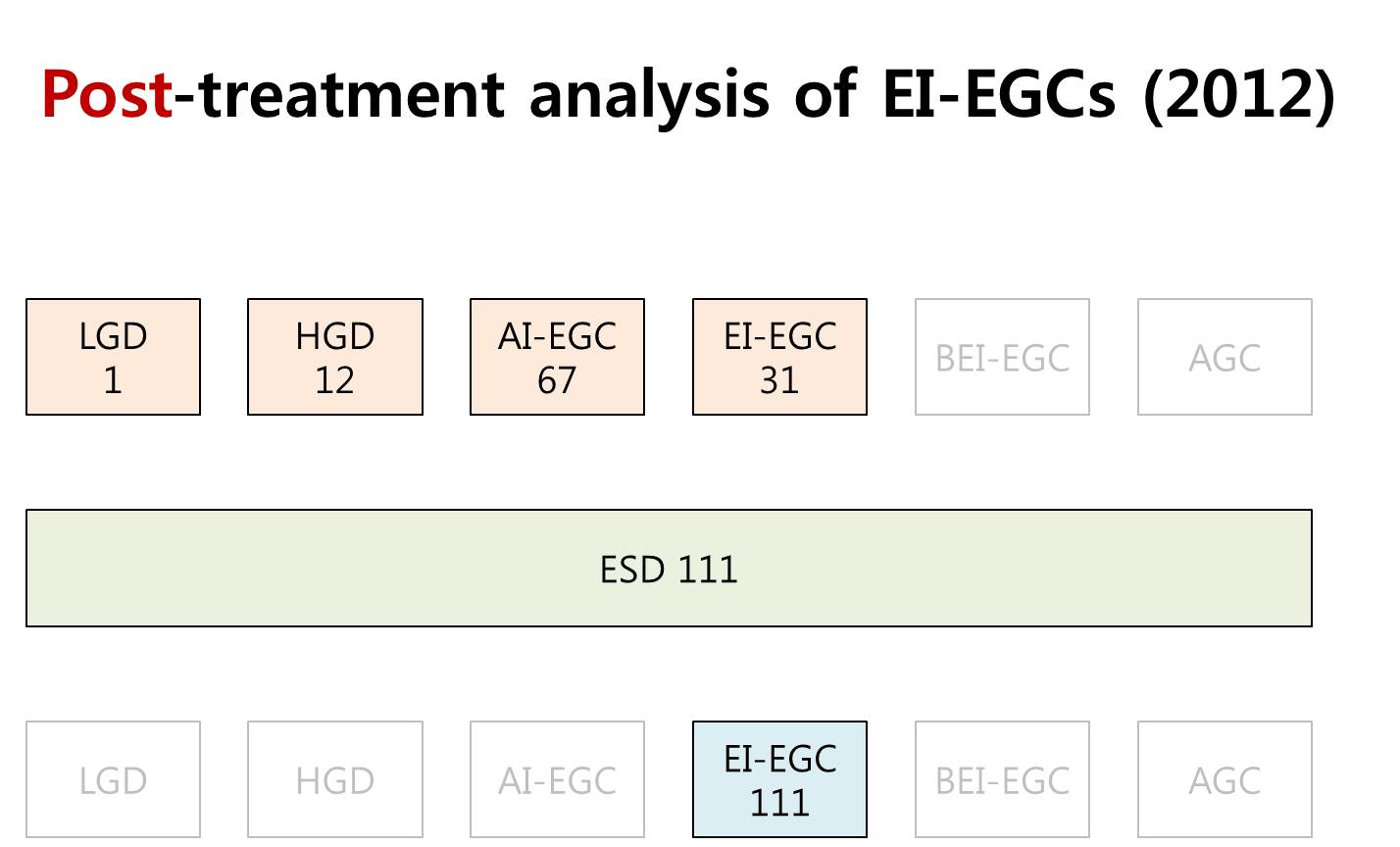
The outcome analysis is usually based on the post-treatment diagnostic groups. In the year 2012, we performed 111 ESDs for post-treatment EI-EGCs. In the beginning, however, the diagnosis was one LGD, 12 HGDs, 67 AI-EGCs and 31 EI-EGCs. So, if you analysis 111 post-treatment EI-EGCs, most of them were actually AI-EGCs before the treatment.
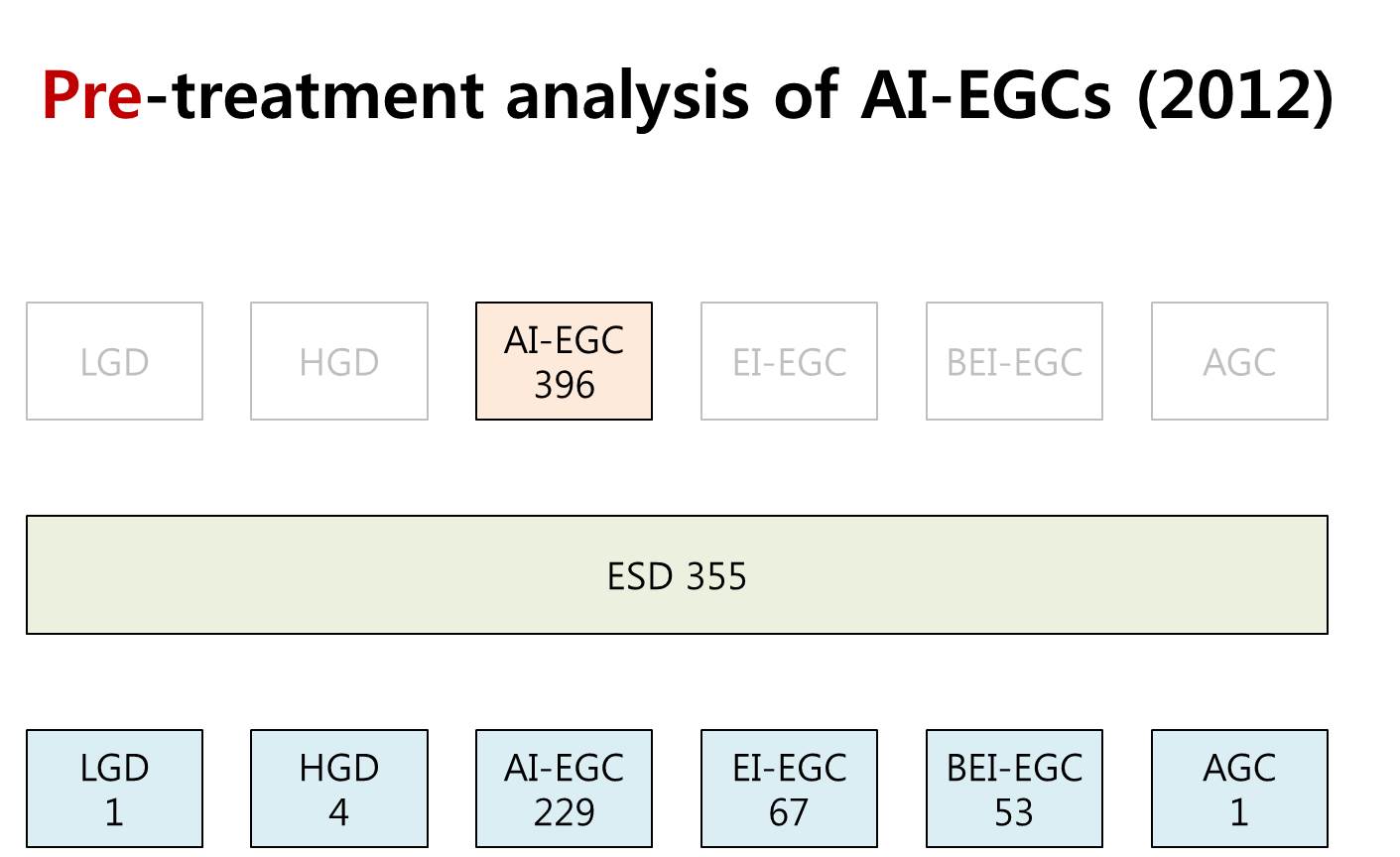
This analysis is based on the pre-treatment diagnostic groups. Among 396 pretreatment AI-EGCs, ESD was done for 355 cases. The final diagnoses were variable. As you can see, the post-treatment diagnosis can be actually everything.
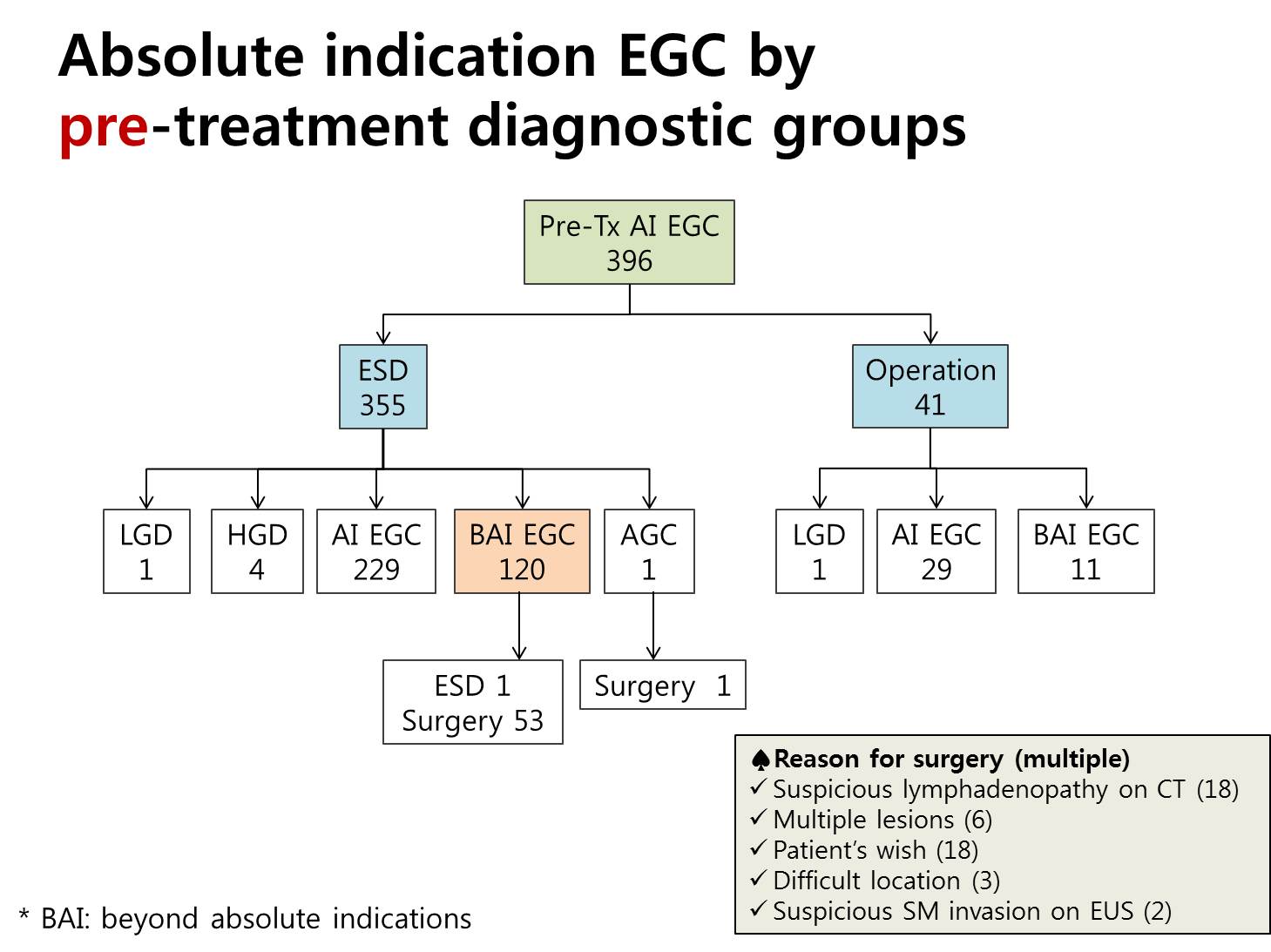
This flow diagram shows how we handled absolute indication early gastric cancers by the pretreatment diagnostic groups. Among 355 early gastric cancers initially treated by ESD, 120 cases, this is 34 percent, belonged to the beyond absolute indication group. Ten percent of patients in the absolute indication group were initially treated by surgery, and you can see the reason in the box at the right hand-side corner. Suspicious lymphadenopathy is the most common reason for surgery. I think this kind of analysis based on the pretreatment diagnostic group has a lot of clinical meanings in the decision making among the treatment options.
![]() Let’s turn to the second issue, lessons from survival analysis.
Let’s turn to the second issue, lessons from survival analysis.
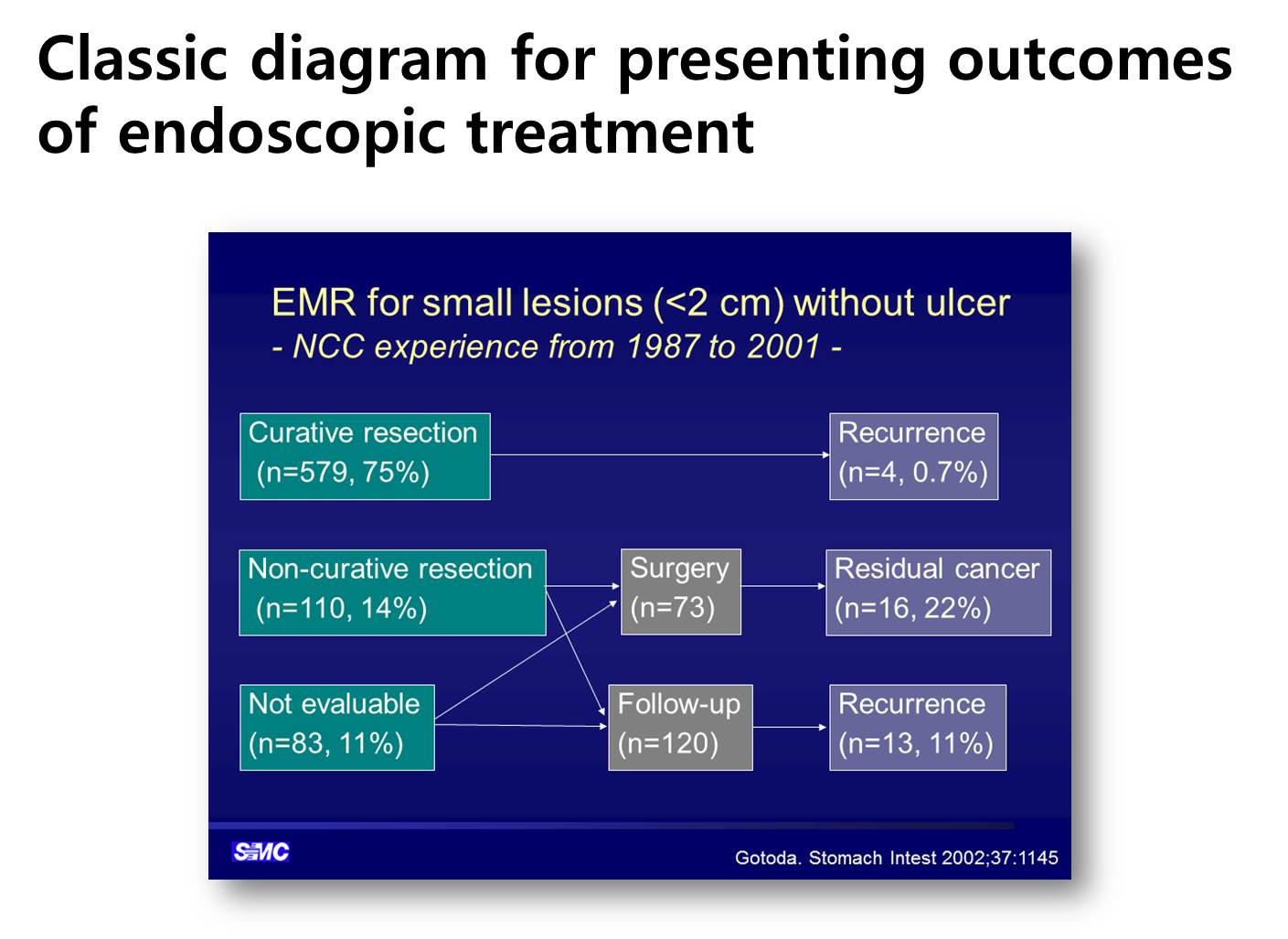
This is a typical example of classic diagram for presenting outcomes of endoscopic treatment.
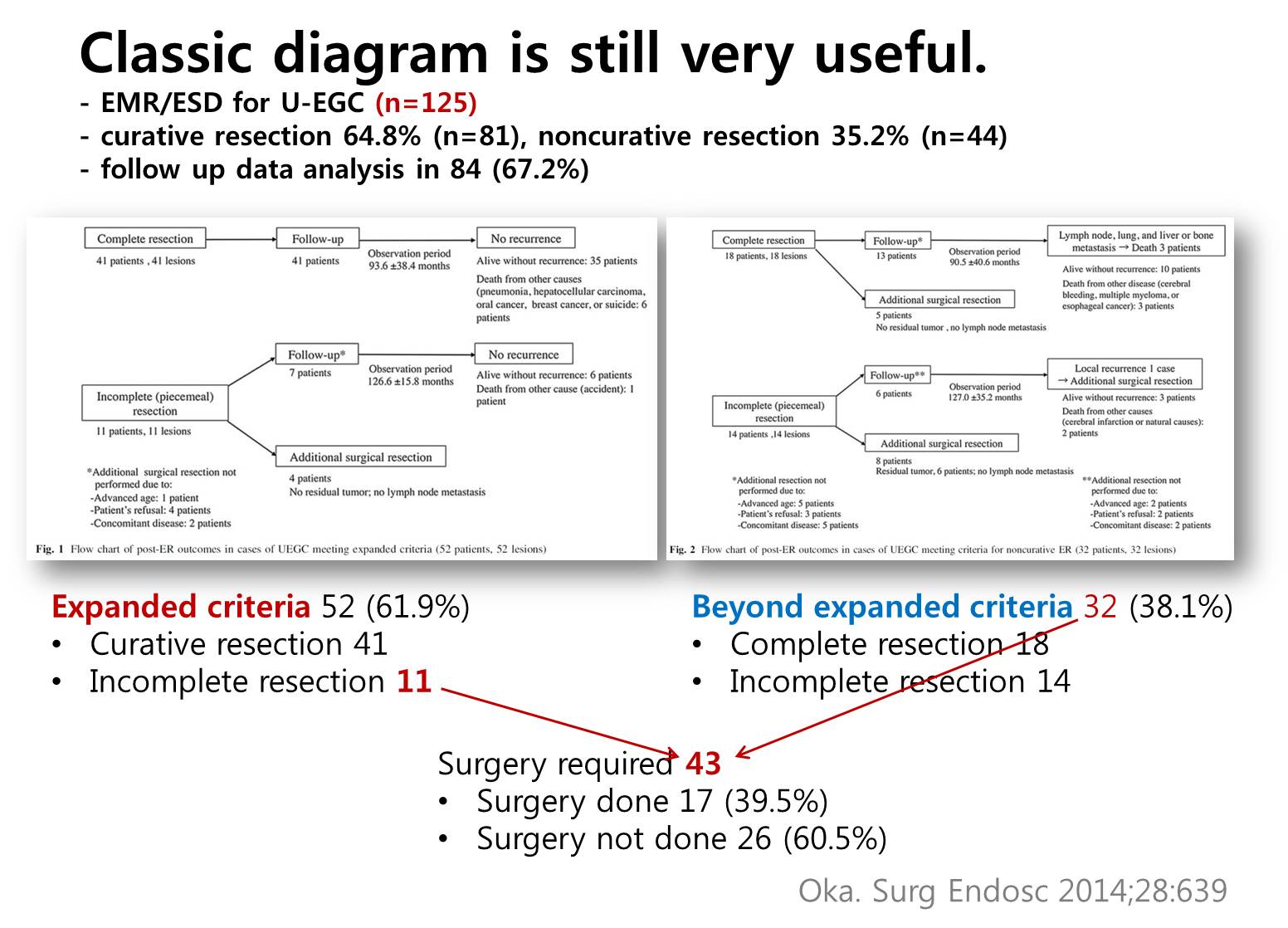
Classic diagram is still very useful and widely used. Professor Oka and his colleagues from Hiroshima University reported their outcome of endoscopic treatment for undifferentiated type early gastric cancers using classic diagrams. They divided their patients into two groups - expanded criteria group and beyond expanded criteria group. Lower part is my own interpretation of his data.
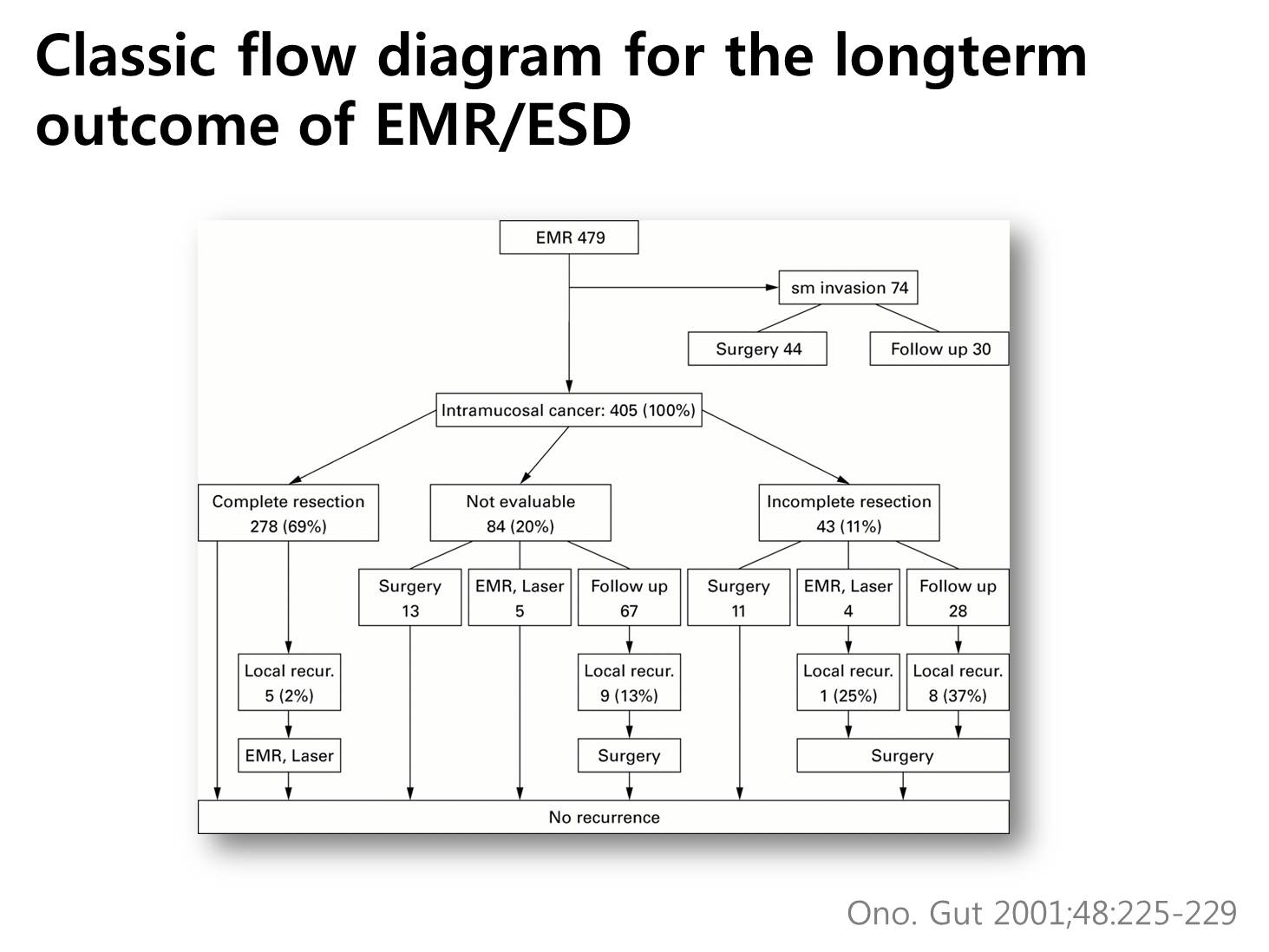
This is another form of classic diagram by doctor Ono.
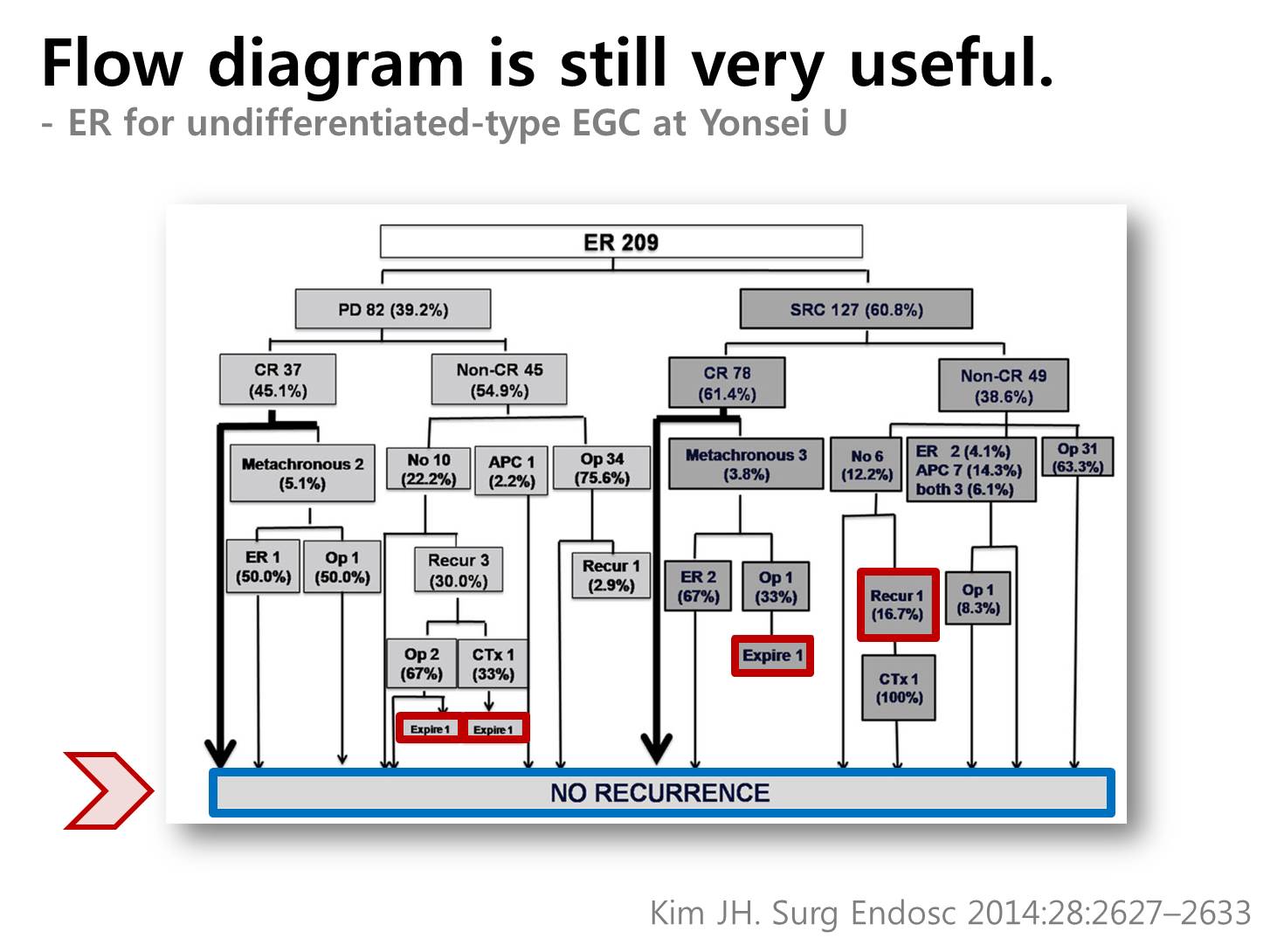
Classic flow diagram is still widely used. However, it is difficult to see the follow-up rate and the duration of observation. In addition, the bottom box of no recurrence is over-emphasized. Cases with bad outcome are frequently hidden in the middle of the diagram.
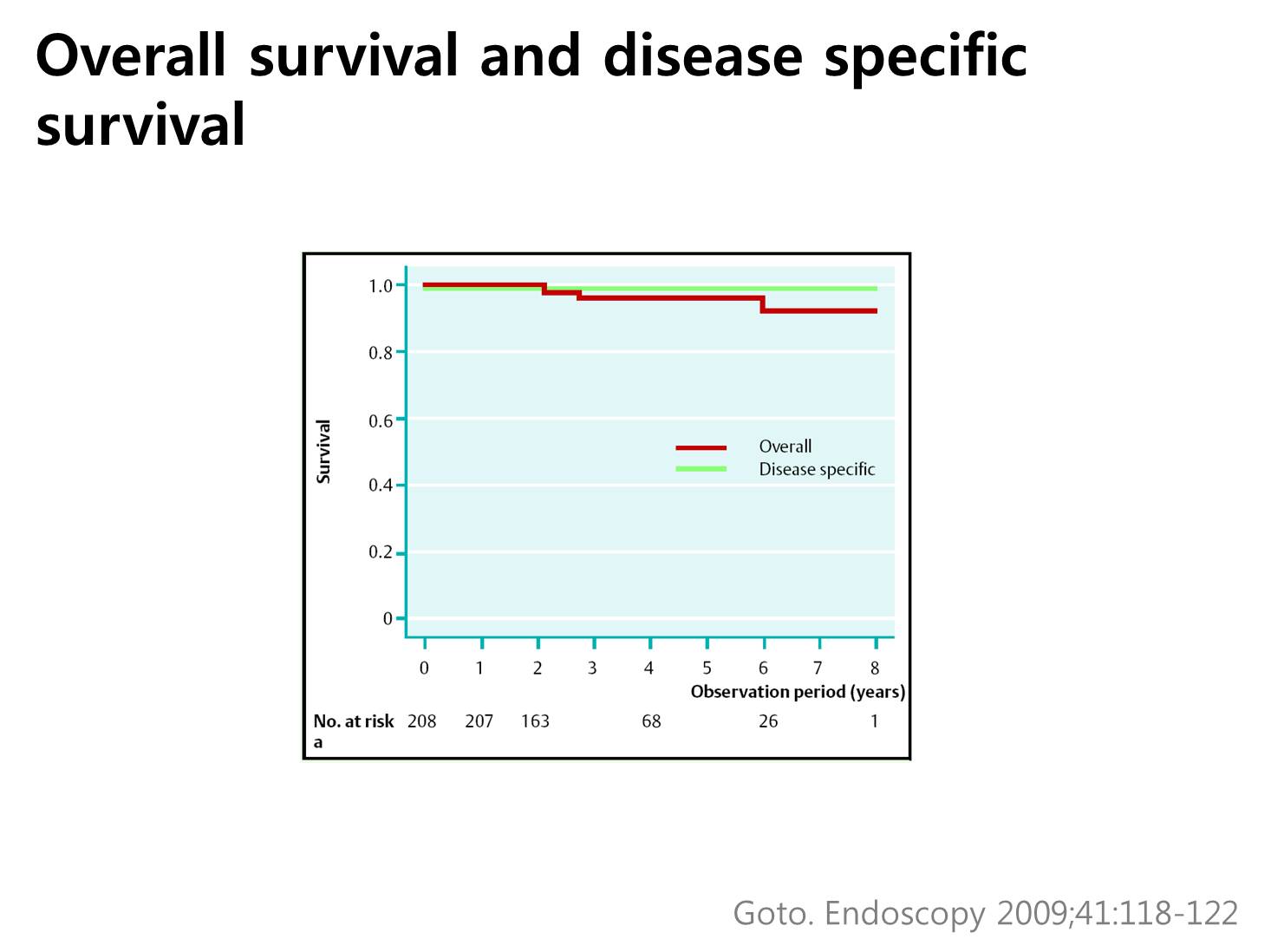
Recently, we can see the Kaplan-Meier survival curves in the ESD outcome studies. In this figure from Japan National Cancer Center Tokyo Hospital, the red line is overall survival, and green line is diseases-specific survival.
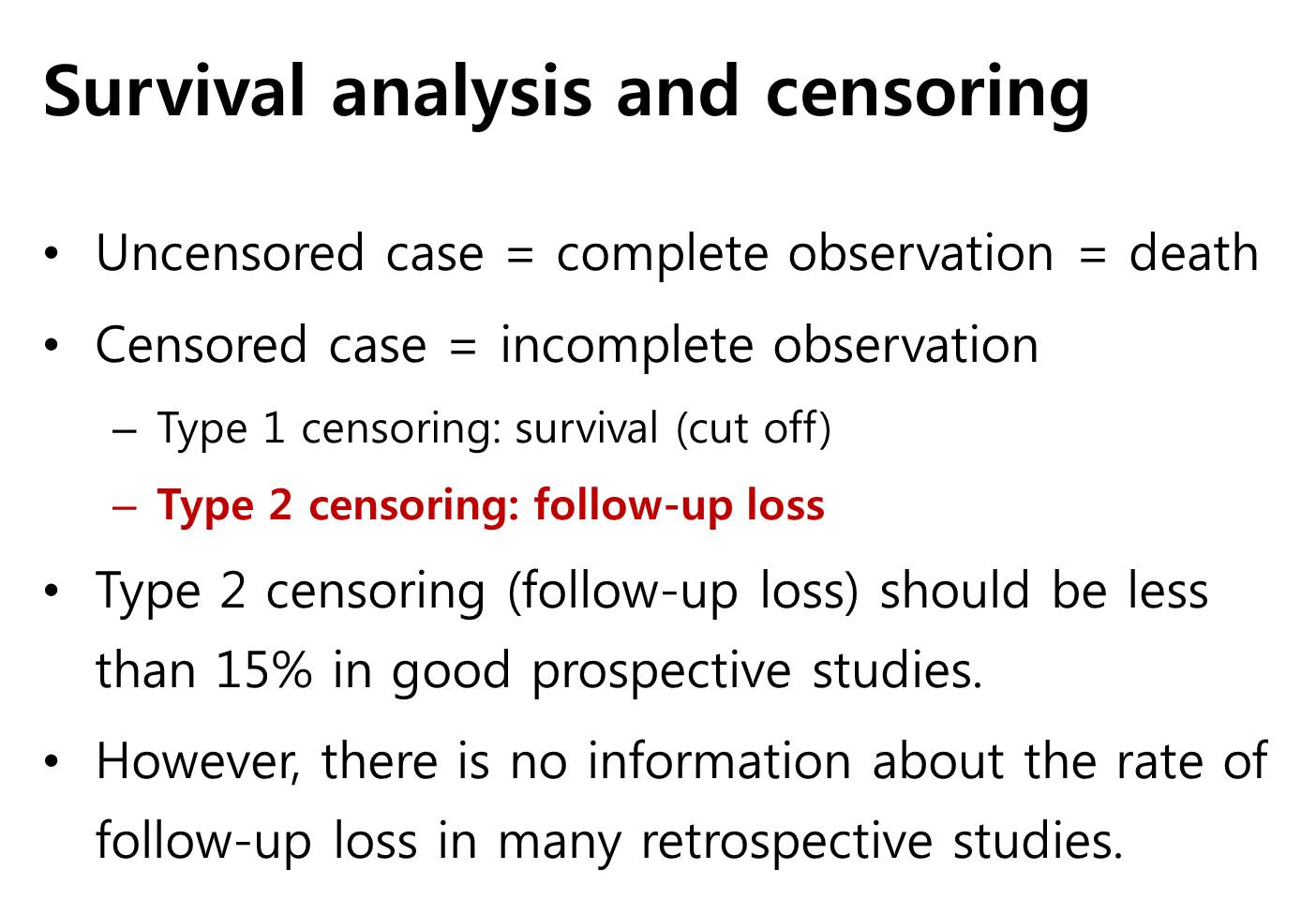
In the survival analysis, the concept of censoring is quite important. Uncensored case means complete observation, which again means death of the patient. Censored case means incomplete observation, and it can be divided into two groups. Type 1 censoring means survival, and type 2 censoring means follow-up loss. Type 2 censoring, follow-up loss, should be less than 15% in good prospective studies. However, there is no information about the rate of follow-up loss in many retrospective studies.
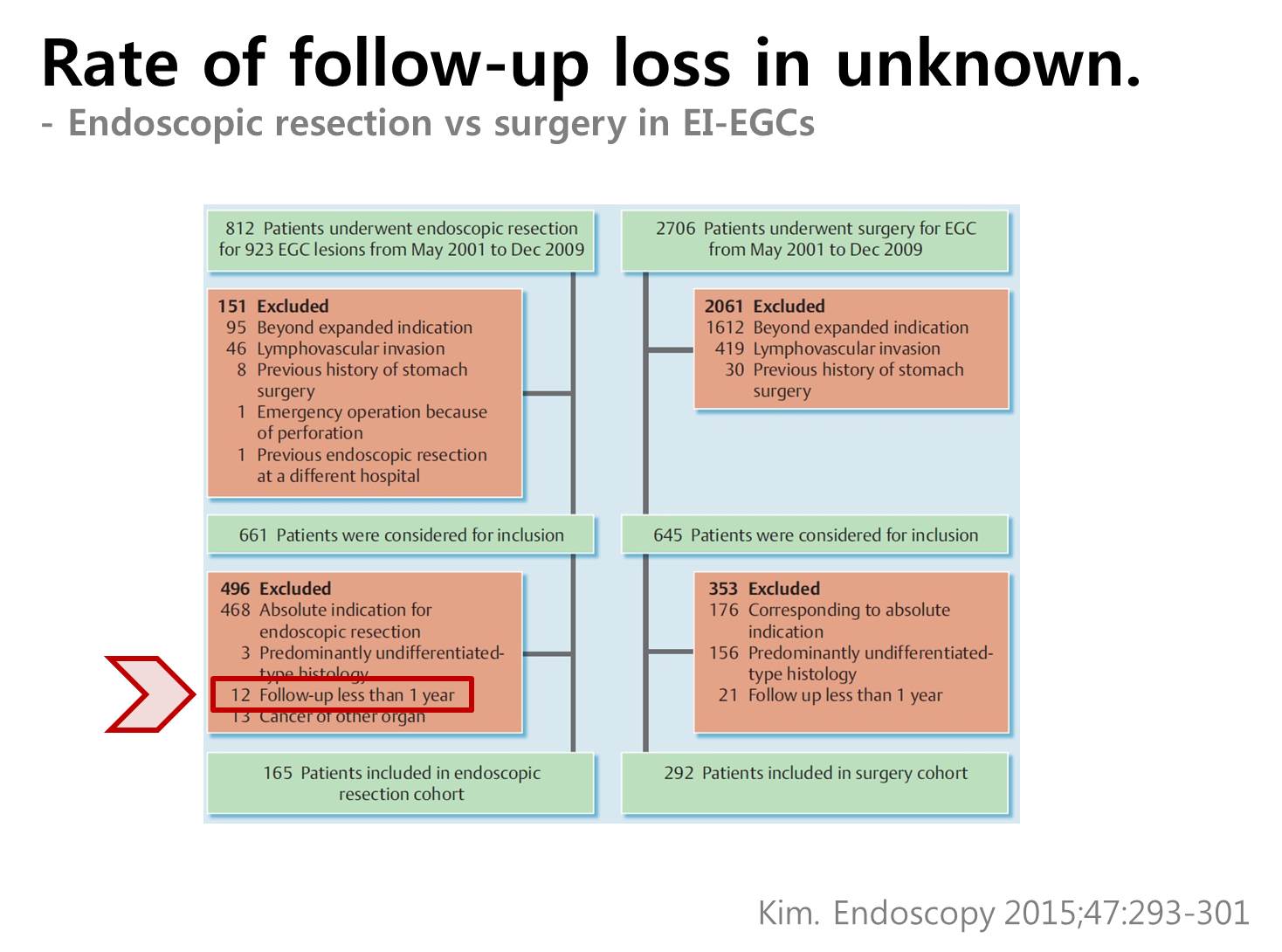
In the recent study from Korea National Cancer Center, cases with follow-up less than 1year was excluded.
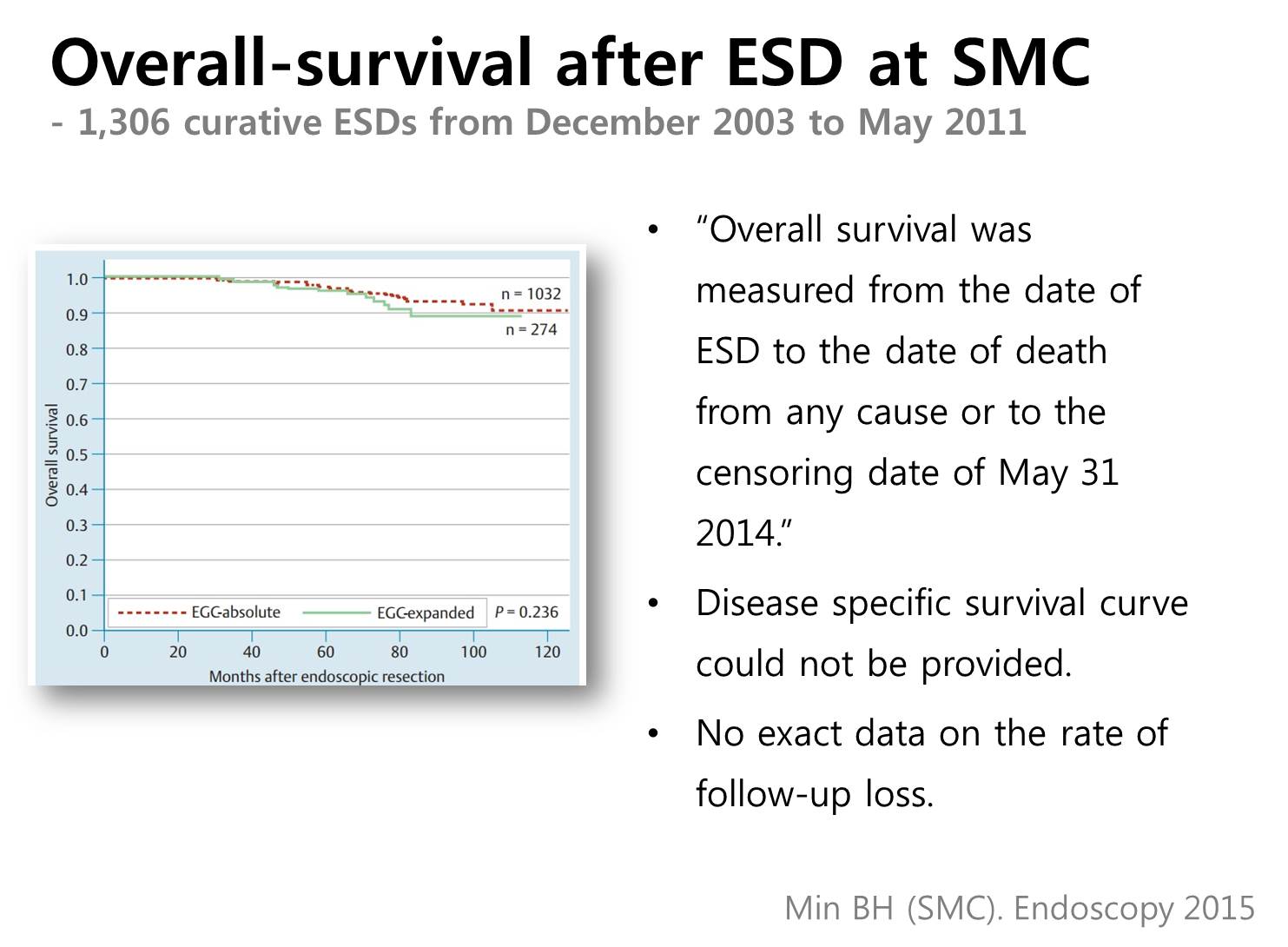
This graph is the survival curve after ESD for EGC at Samsung Medical Center. The red dot line is the absolute indication group and the green solid line is the expanded indication group. In the article, we wrote that “Overall survival was measured from the date of ESD to the date of death from any cause or to the censoring date of May 31, 2014.” Disease specific survival curve could not be provided. And we did not report the rate of follow-up loss.
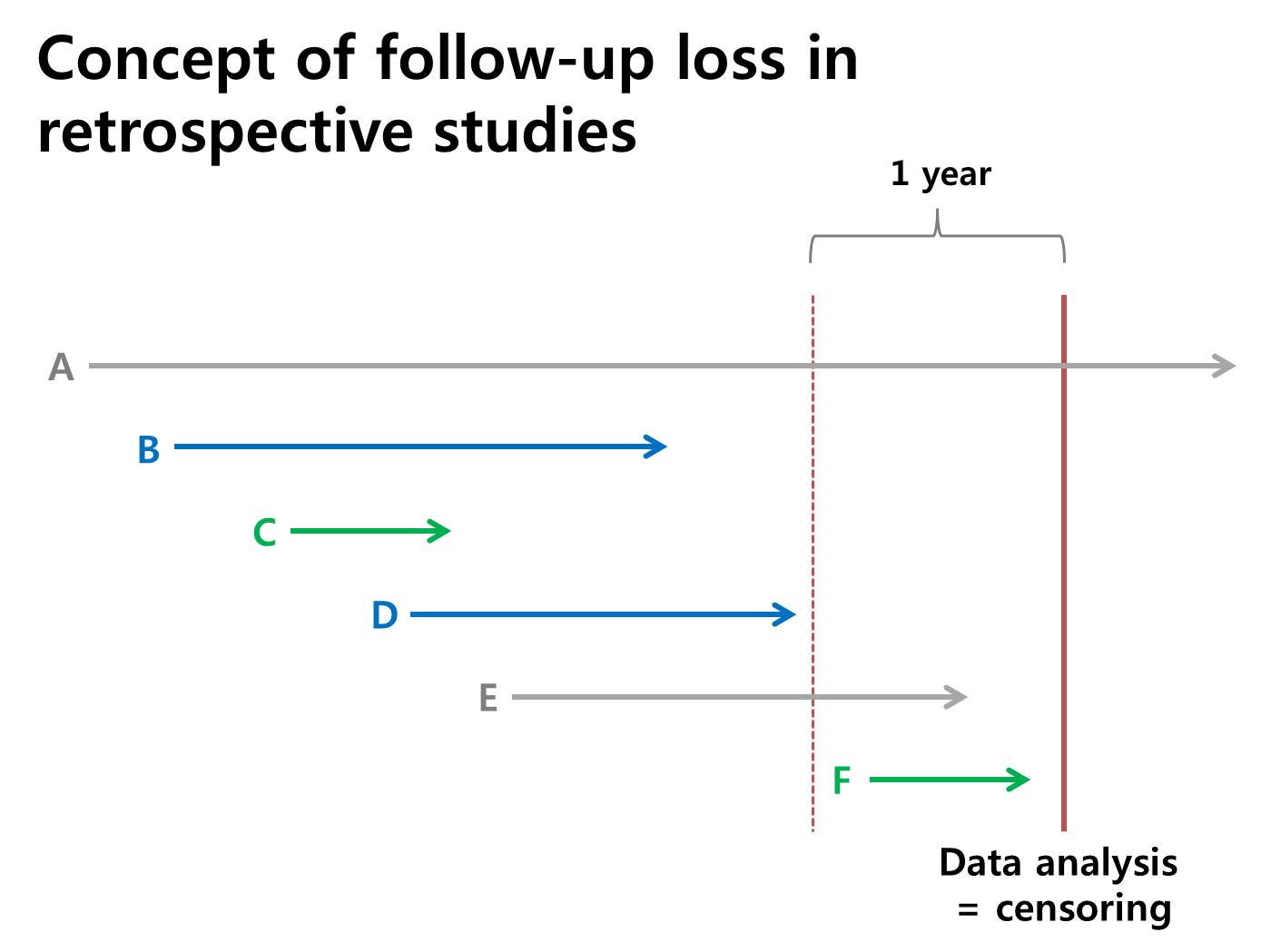
Let's think about the concept of follow-up loss in the retrospective studies. Data analysis is usually set to a specific day. We call it a censoring day. In most studies, cases in green color, C and F, are excluded because the follow up duration is short, such as less than a year. I worry about the cases in blue color, B and D, because they are included in most retrospective studies, but actually they are follow-up loss cases. They did not appear for a long time. I propose that we would report the percentage of cases like B and D, that is the follow-up loss rate.
![]() Next, I would discuss why the failure cases are important.
Next, I would discuss why the failure cases are important.
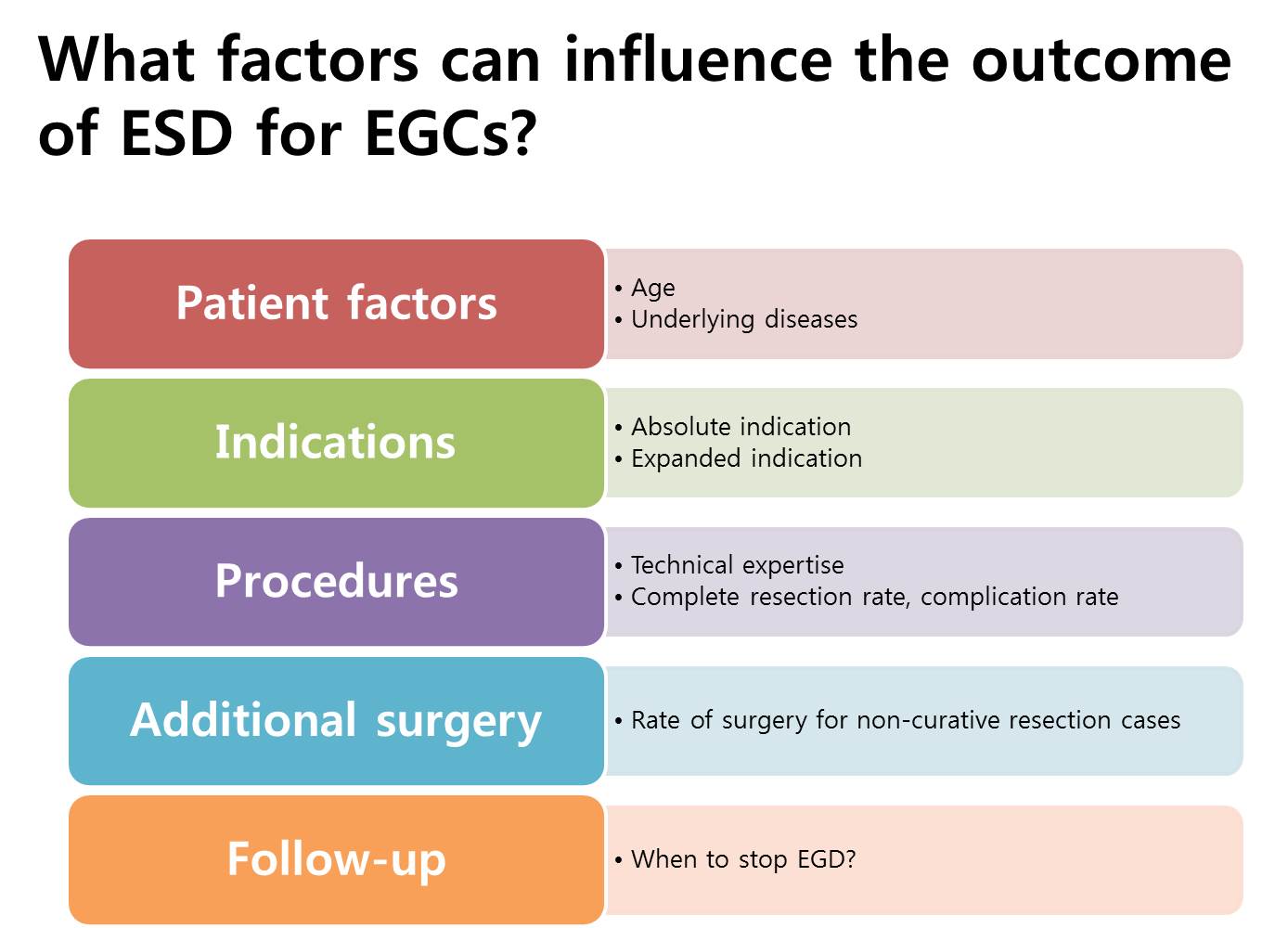
What factors can influence the outcome of ESD for EGCs? Of course, indications are most important. However, technical aspect is not a big problem for experienced hands. In my opinion, the rate of additional surgery and follow-up strategies are more important than our expectation.
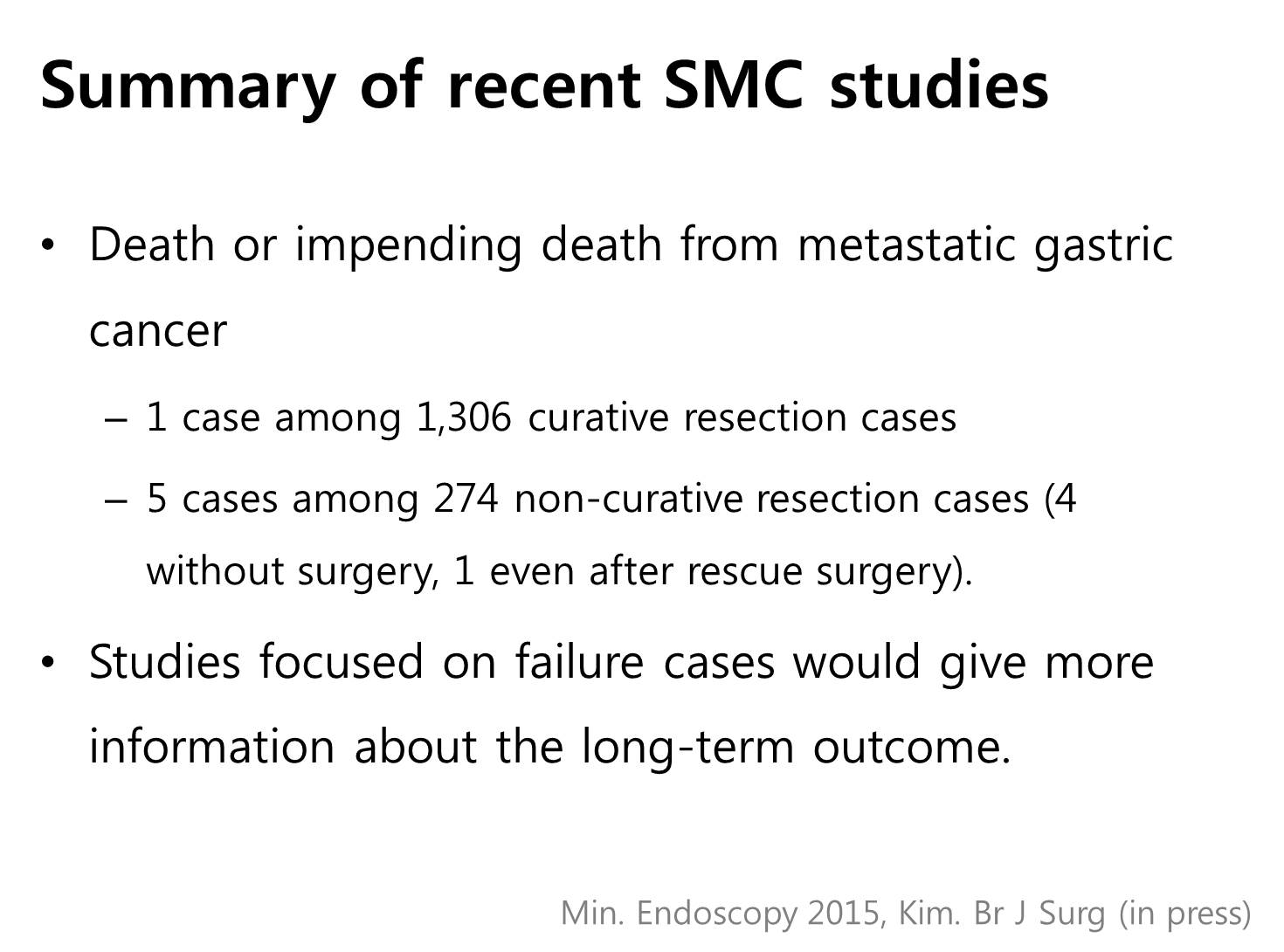
In our center, most death or impending deaths from metastatic gastric cancer after endoscopic treatment came from non-curative resection group. Five out of six fatal cases came from non-curative resection group - 4 cases without surgery, 1 case even after rescue surgery. I guess studies focused on failure cases would give more information about the long-term outcome.
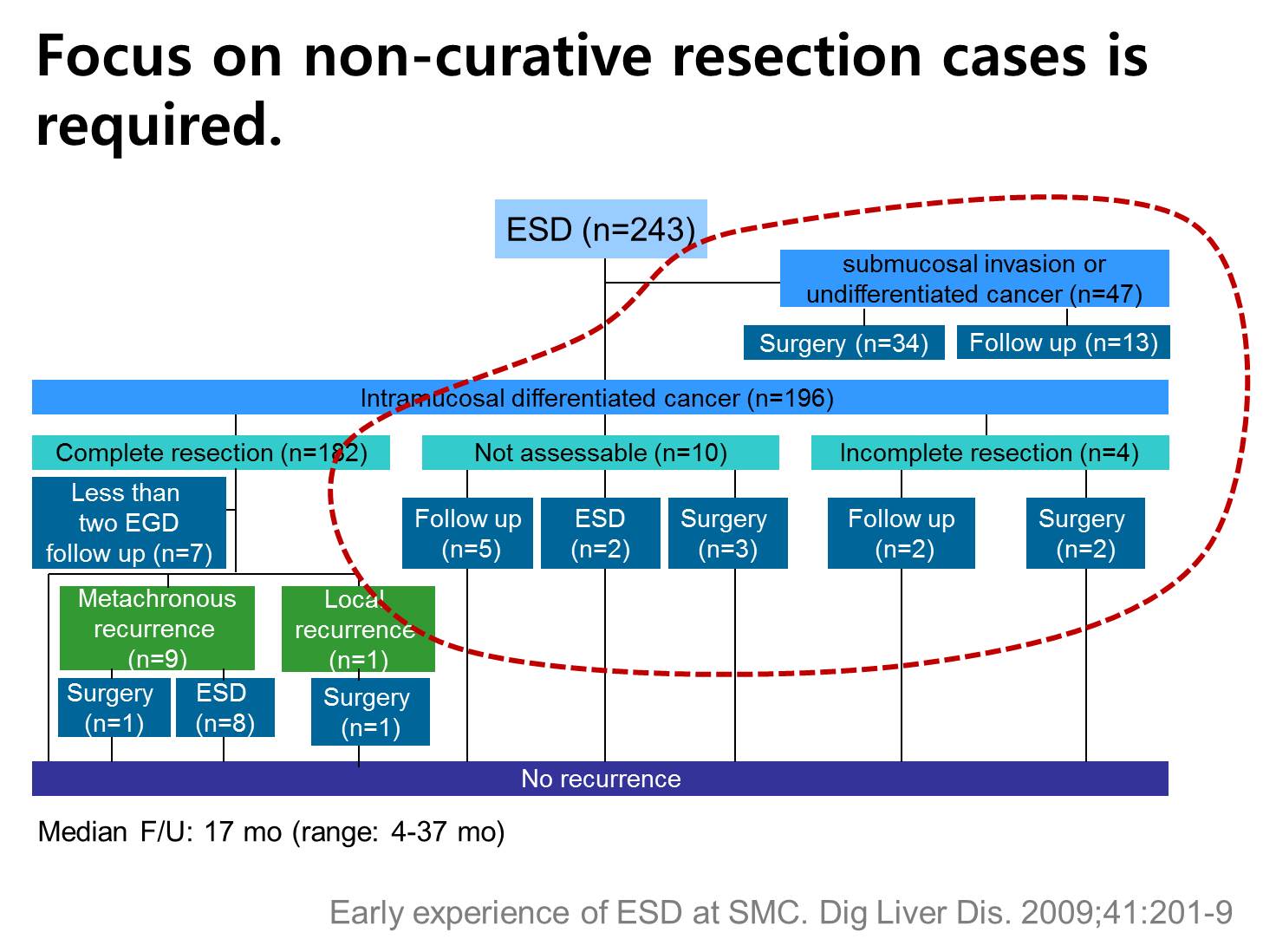
This is our early experience of ESD at our center. Cases with submucosal invasion, incomplete resection or not assessable result should be carefully observed.
![]() The next topic is the role of endoscopic pictures.
The next topic is the role of endoscopic pictures.
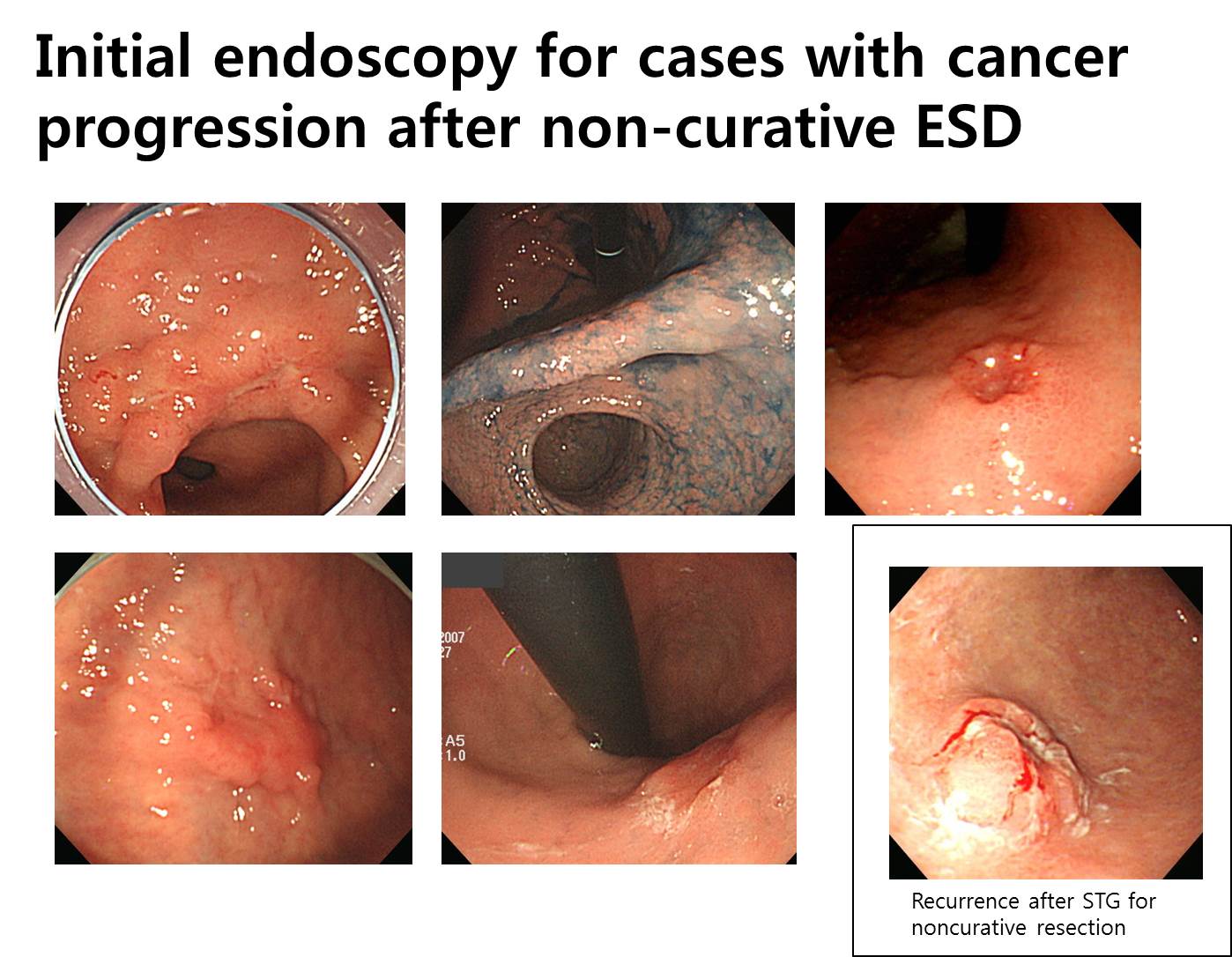
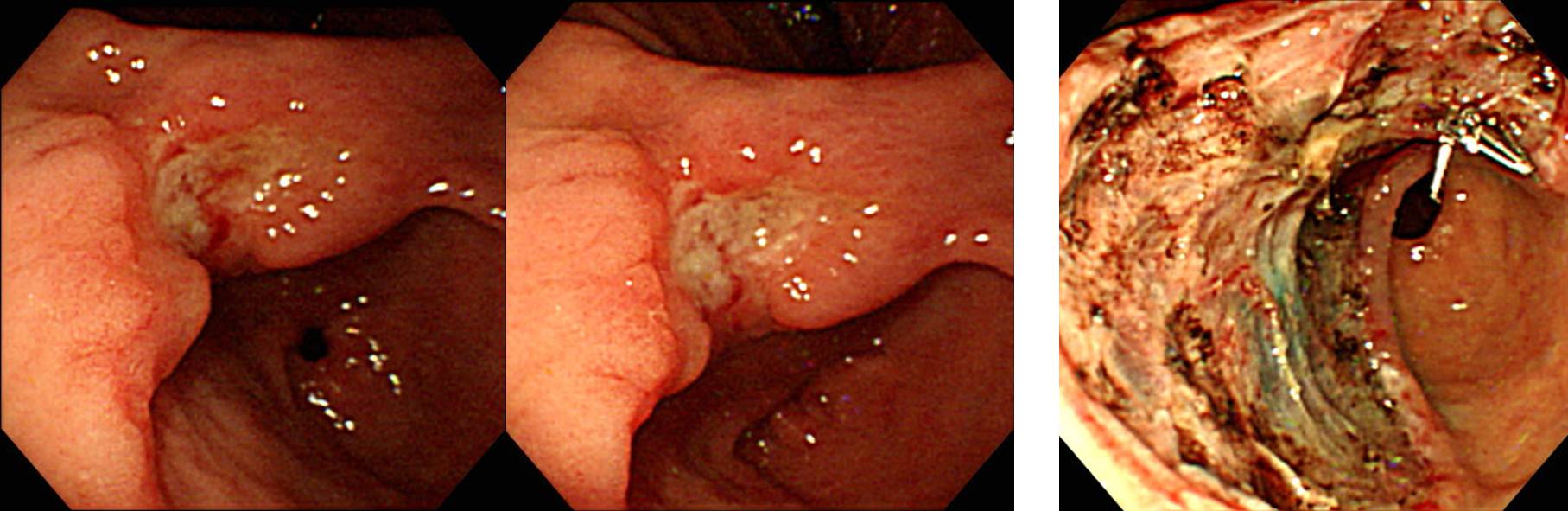
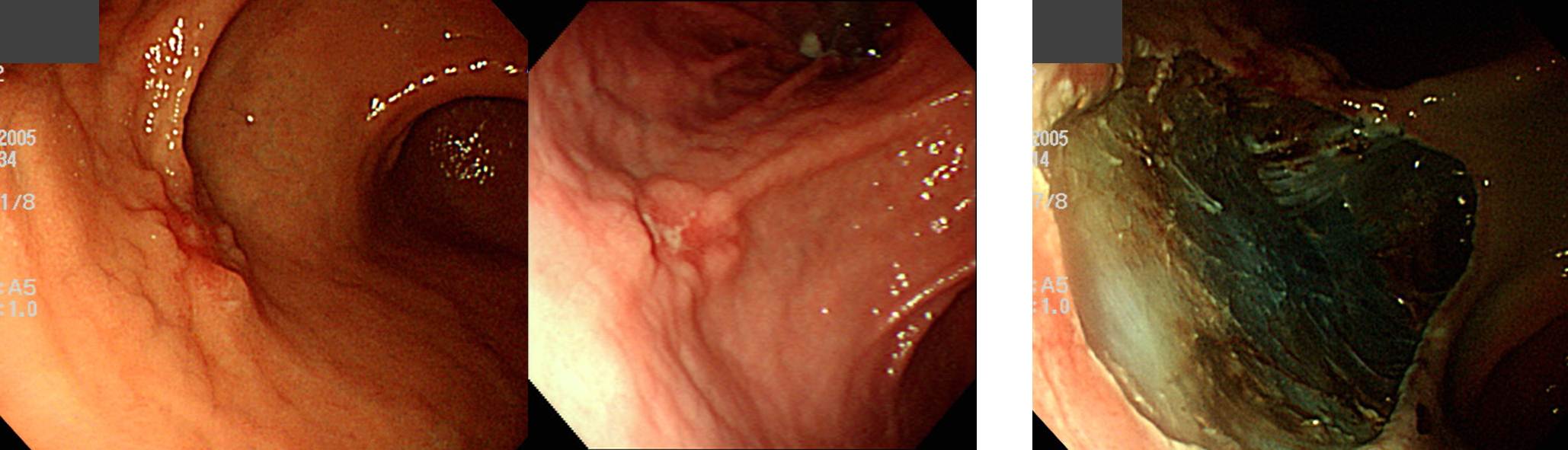
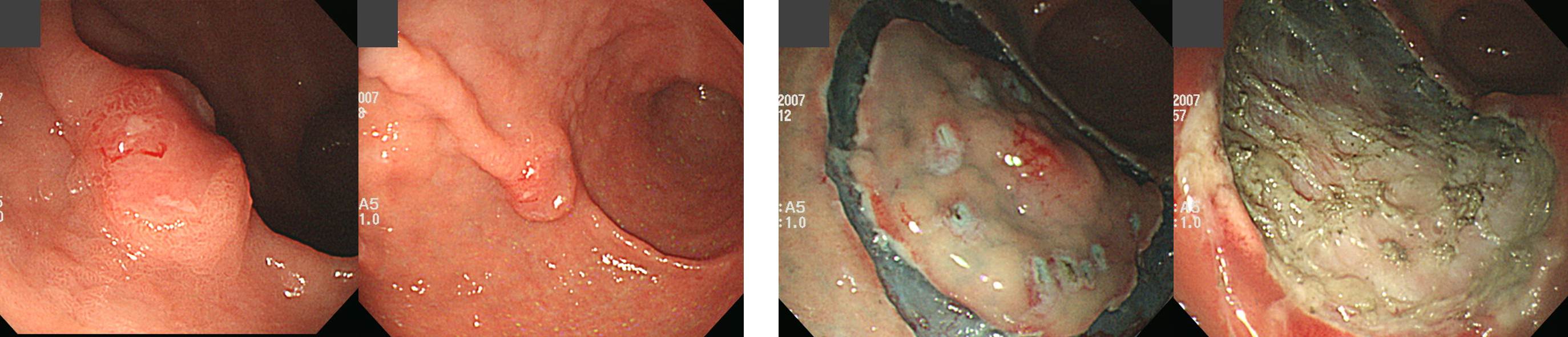
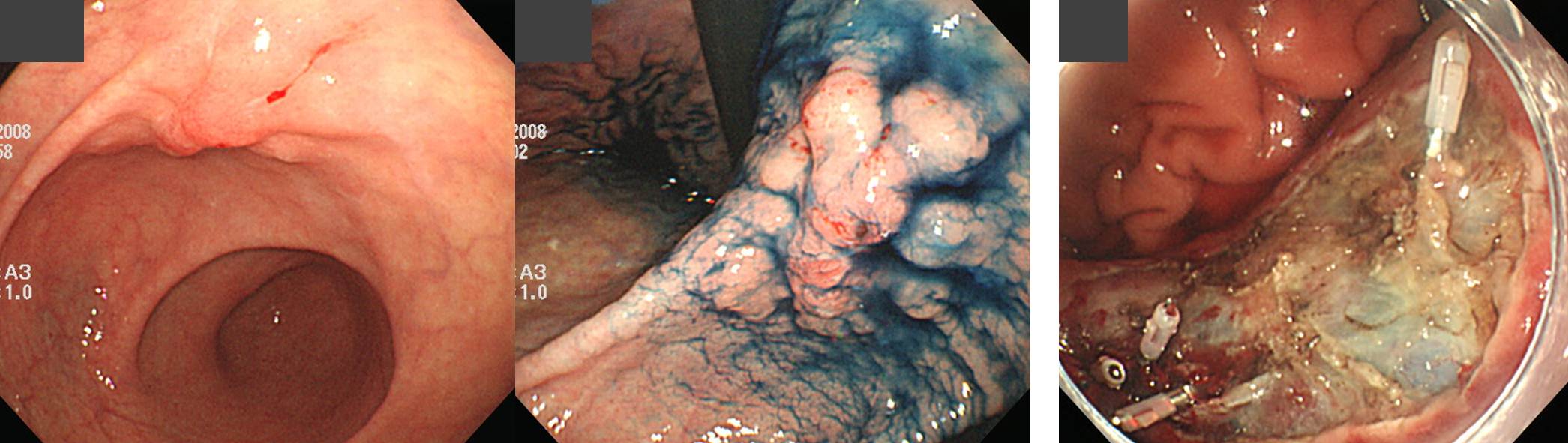
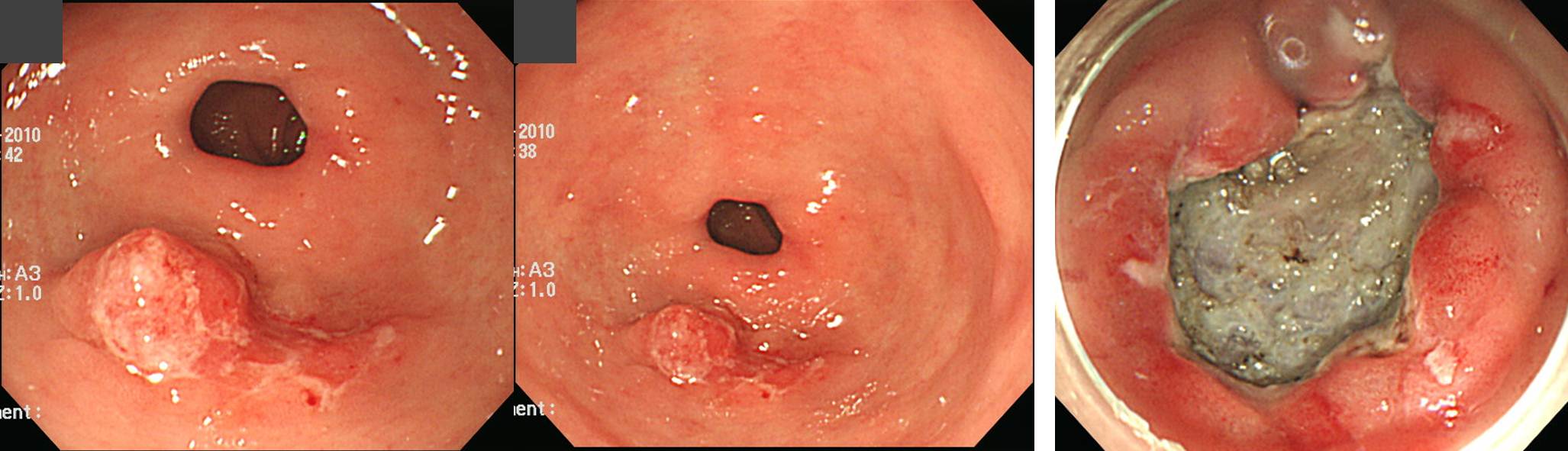
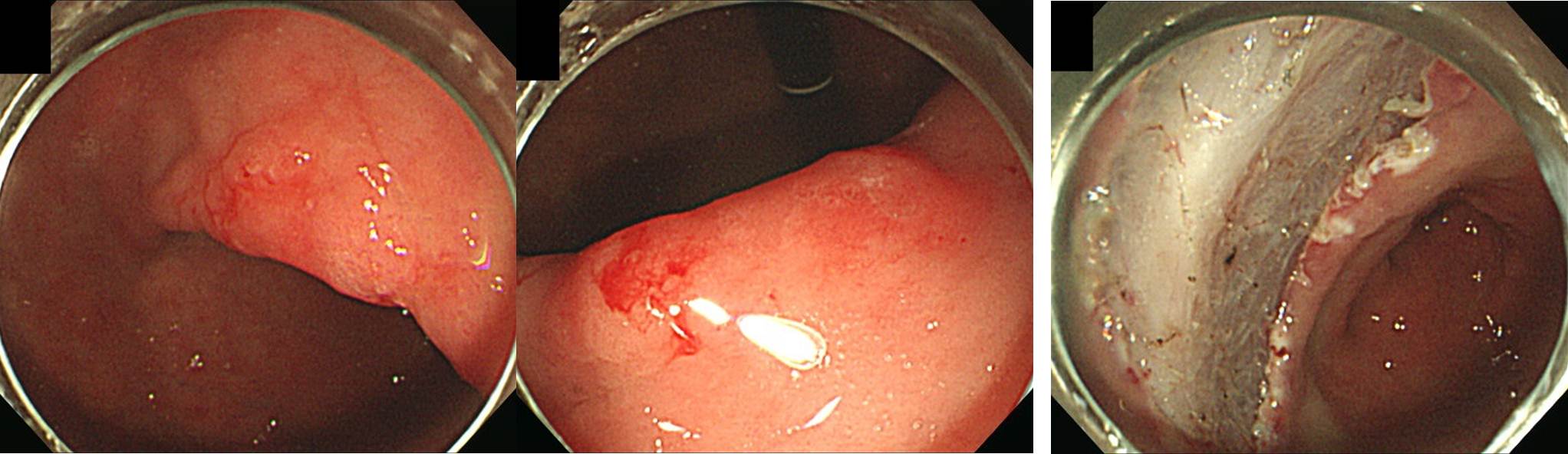
A few months ago, I had a presentation about the long-term follow-up after non-curative resection. I showed this slide of 6 cases with cancer progression. Some are elevated, some are depressed, and some are flat. There is no uniform characteristics. After my presentation, I got some questions, most of them were about the endoscopic pictures. They have specific questions about each cases. I learned a lot from case-based discussions. After that experience, I began to think about the role of endoscopic pictures in the endoscopy literature.
This is the first EMR article in Korea. I was the first author and the corresponding author was professor Hyun Chae Jung. In that article, there were only four pictures from one case.
This report from Asan Medical Center is very important. It has very rare information about the natural course of non-curative resection without additional treatment. There were 3 mortality cases. However, there were no endoscopic pictures. This is a typical example of endoscopy report without endoscopic picture.
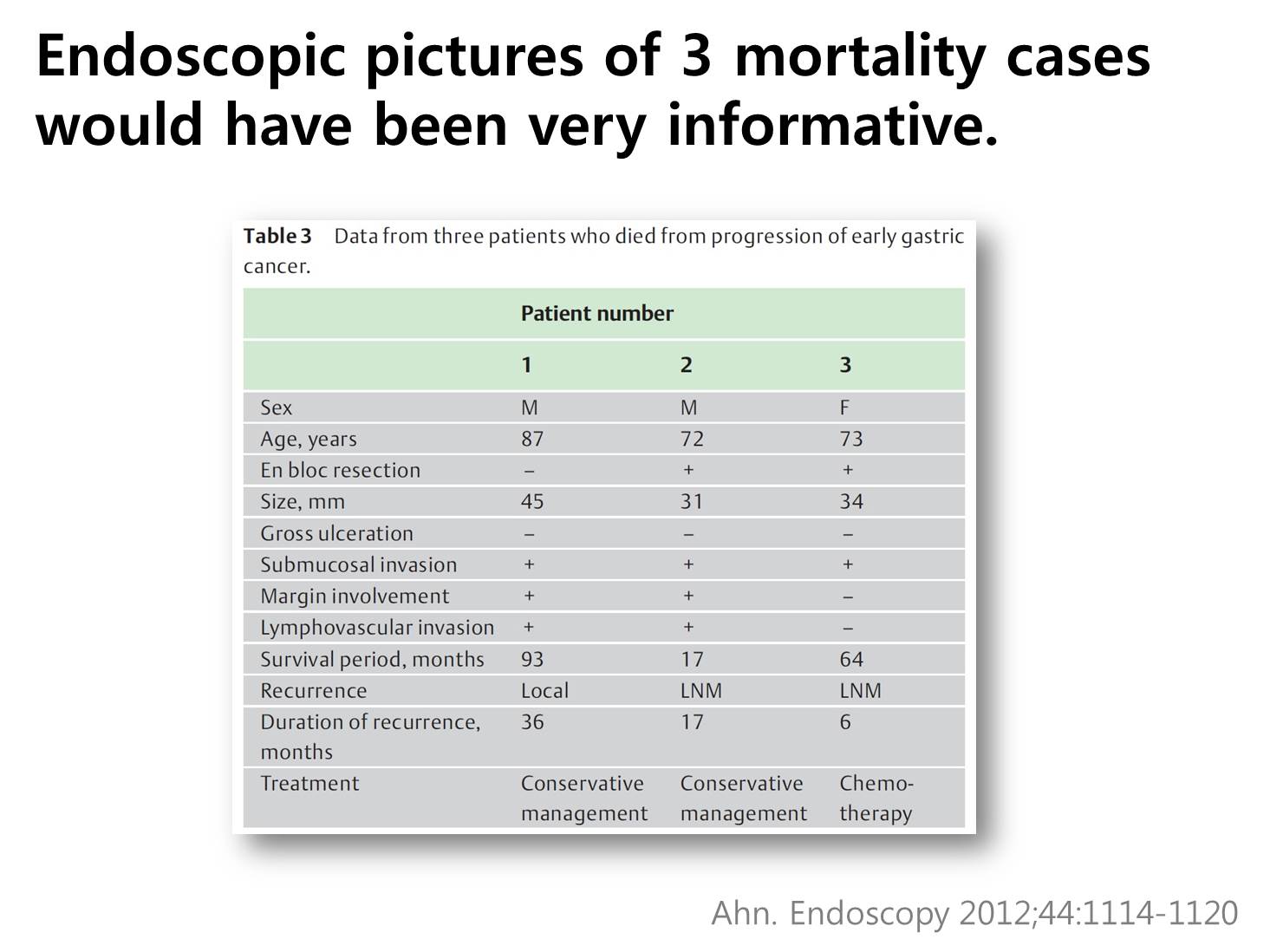
If we have endoscopy pictures of this three cases, we can learn a lot.
We are endoscopists. We are making articles without endoscopic pictures. Why? Do we pursue the theoretical endoscopy. It means endoscopy by the brain rather than by the hands and the heart. It also means number-based endoscopy rather than case-based endoscopy. With more endoscopic pictures in our articles and presentations, we can make our discussion more realistic and more practical.
![]() From now on, I’d like show you follow-up data of endoscopic resection for differentiated type gastric cancers at my institution.
From now on, I’d like show you follow-up data of endoscopic resection for differentiated type gastric cancers at my institution.
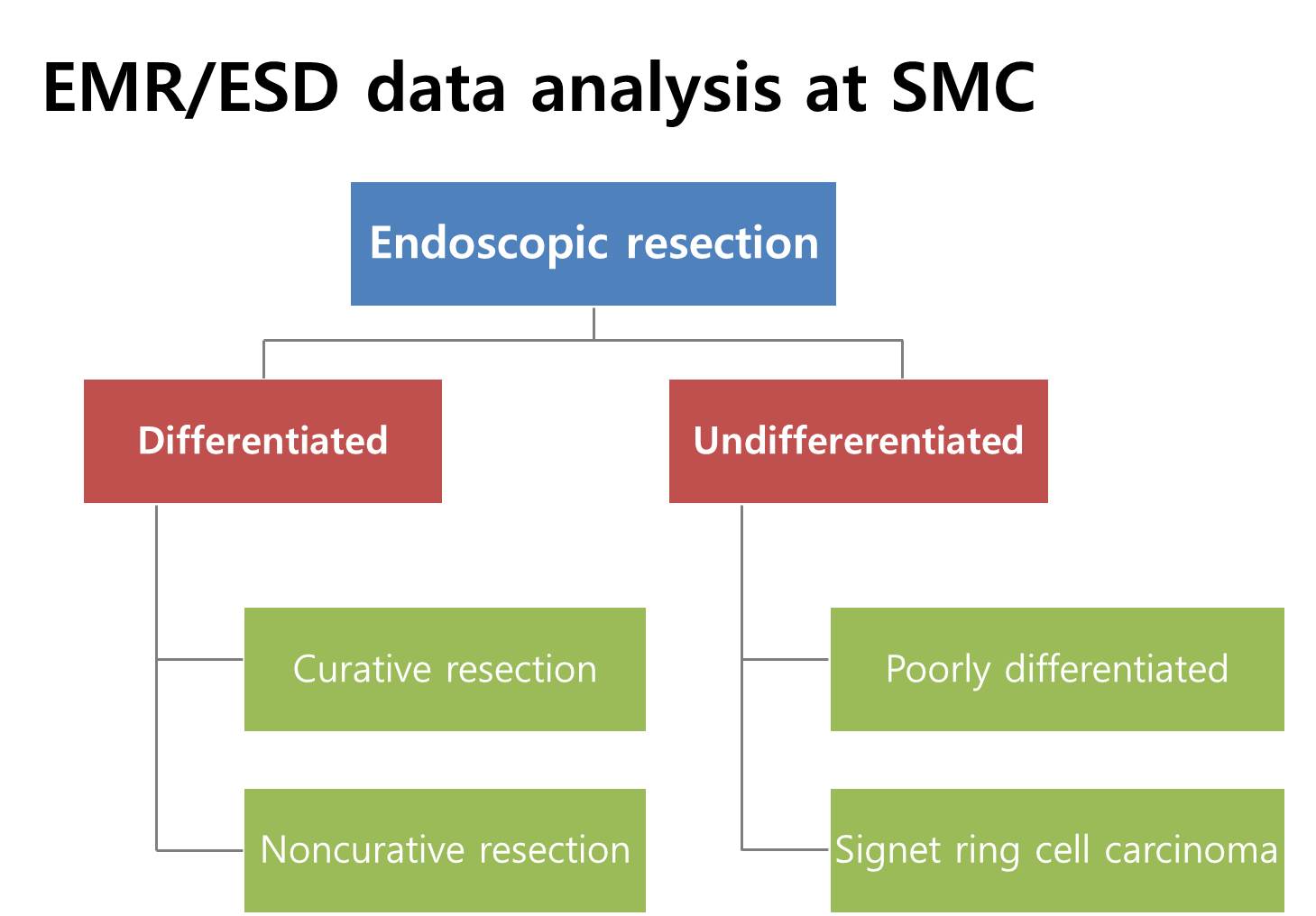
In our institution, we usually recommend surgery for EGCs with undifferentiated histology, so most cases have differentiated histology. After endoscopic resection, the results can be either curative resection or non-curative resection based on the pathological findings.
After endoscopic resection of differentiated type EGCs, the results can be either curative resection or non-curative resection based on the pathological findings.
![]() I'll start with long-term outcome after curative resection.
I'll start with long-term outcome after curative resection.
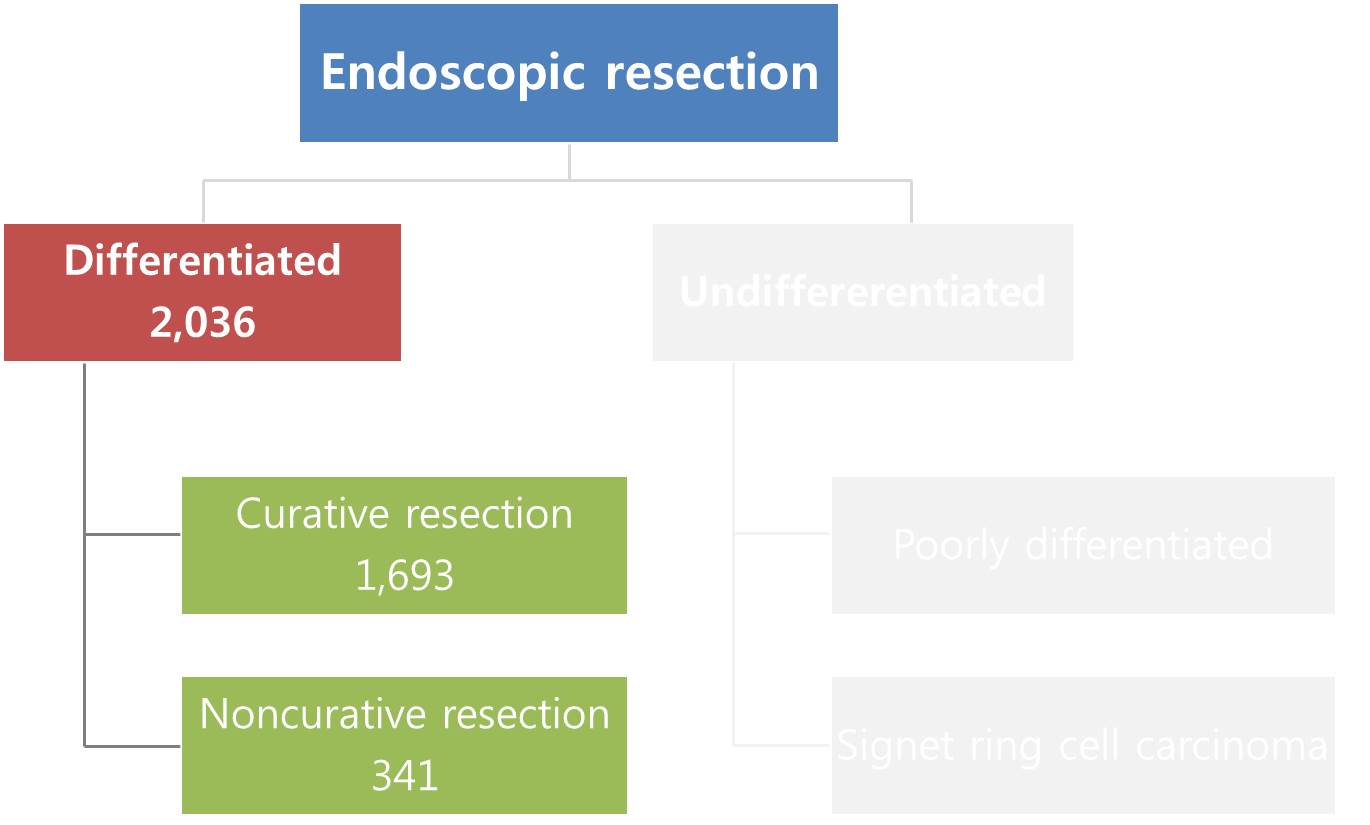
We reviewed the long-term outcome of early gastric cancers, which were treated by ESD at Samsung Medical Center. There were 1,838 patients with 1,889 differentiated-type EGCs. Cancers with both differentiated and undifferentiated component were classified according to the quantitatively predominant histologic type.
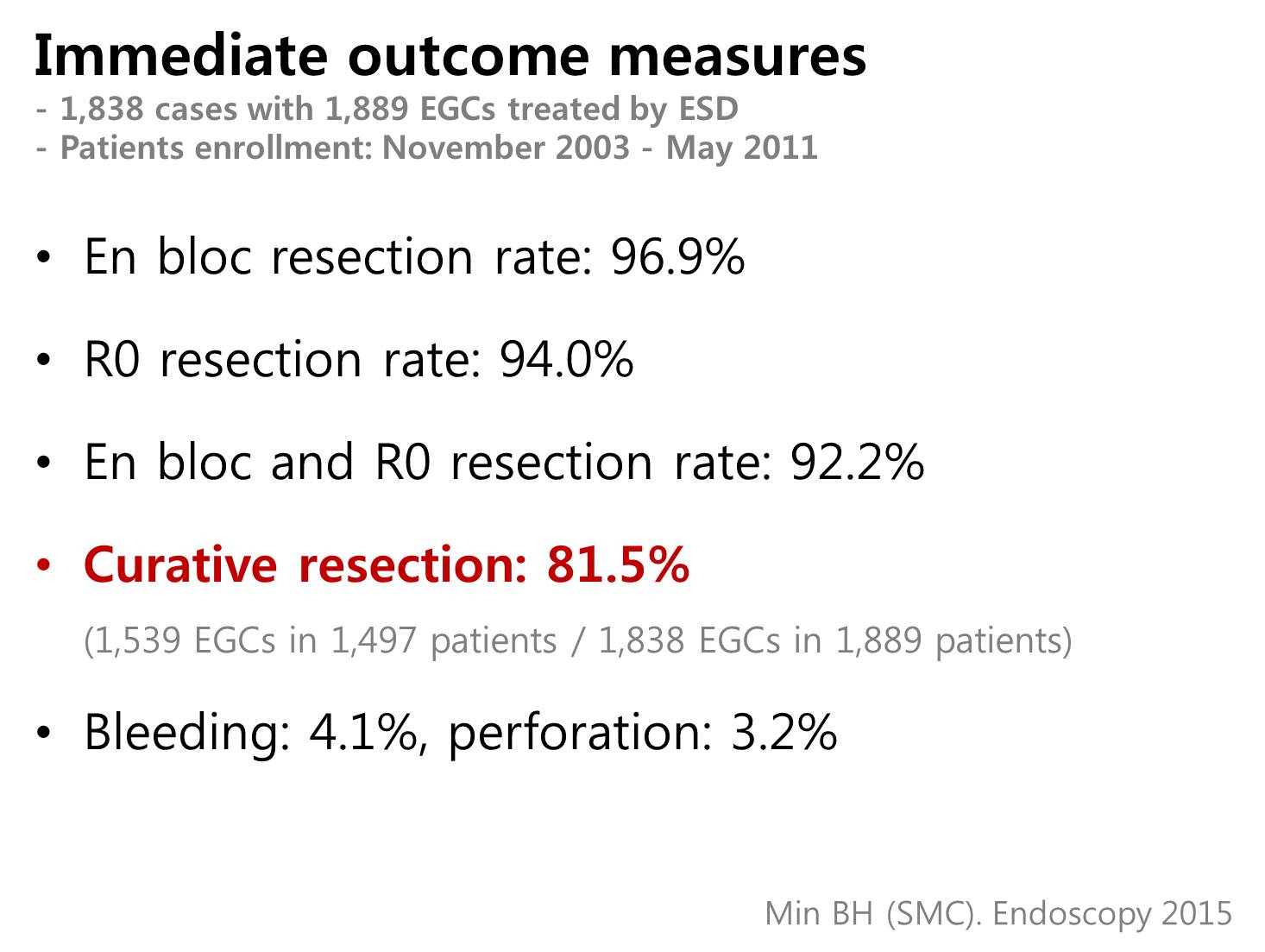
The immediate technical outcome measures were very good. The en bloc resection rate, R0 resection rate and en bloc plus R0 resection rate was 96.9% 94.0%, and 92.2%, respectively. The overall rate of curative resection was 8.15 percent. Complication rates - bleeding: 4.1%, perforation: 3.2% - were clinically acceptable.
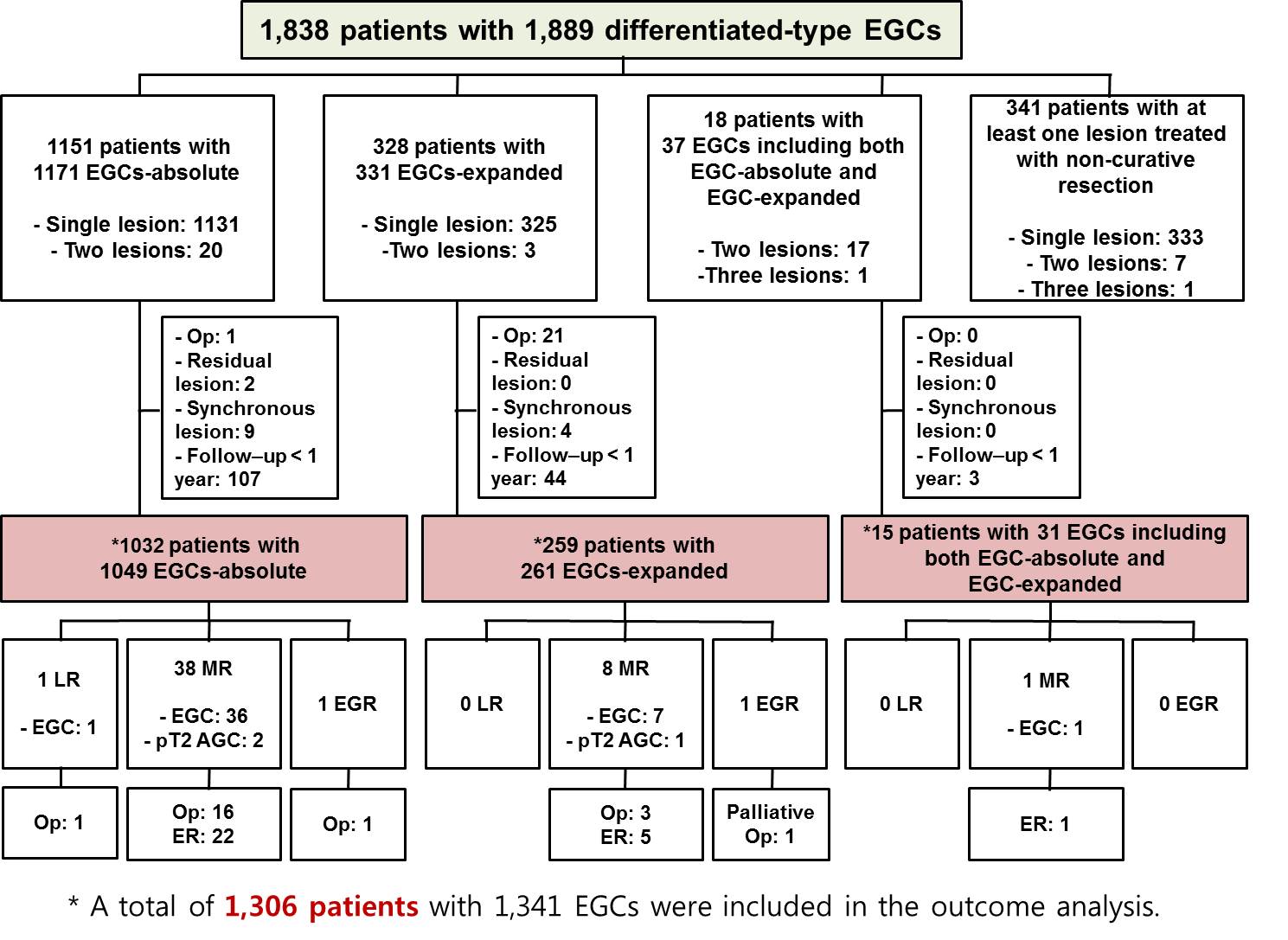
After exclusion of patients with surgery, residual or synchronous lesions, and short follow-up, a total of 1,306 patients with 1,341 EGCs were finally included in the analysis of long-term outcomes after curative ESD.
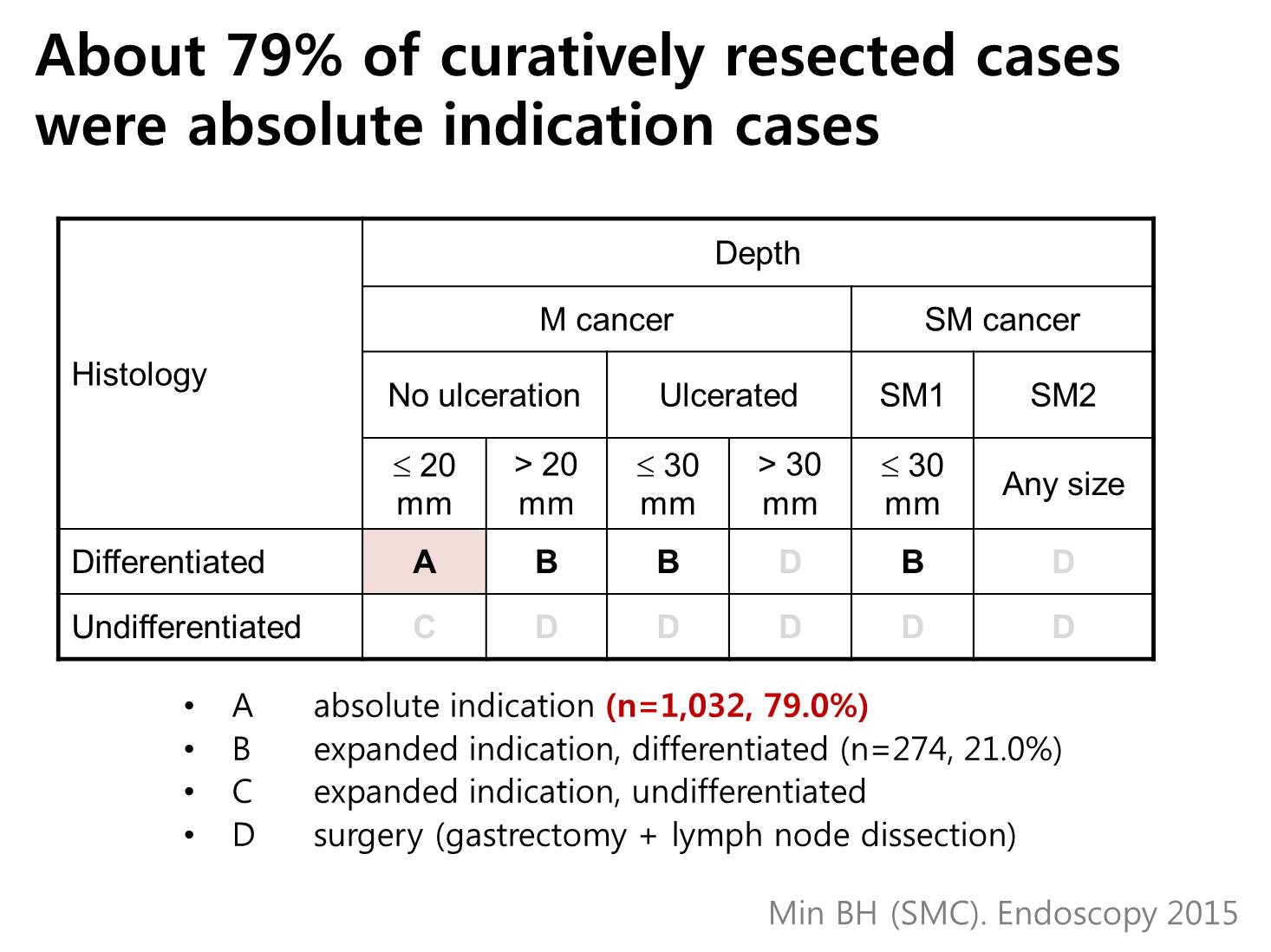
Among 1,306 patients, 79.0% (1,032/1,306) were absolute indication cases, and 21% (274/1,306) were expanded indication cases.
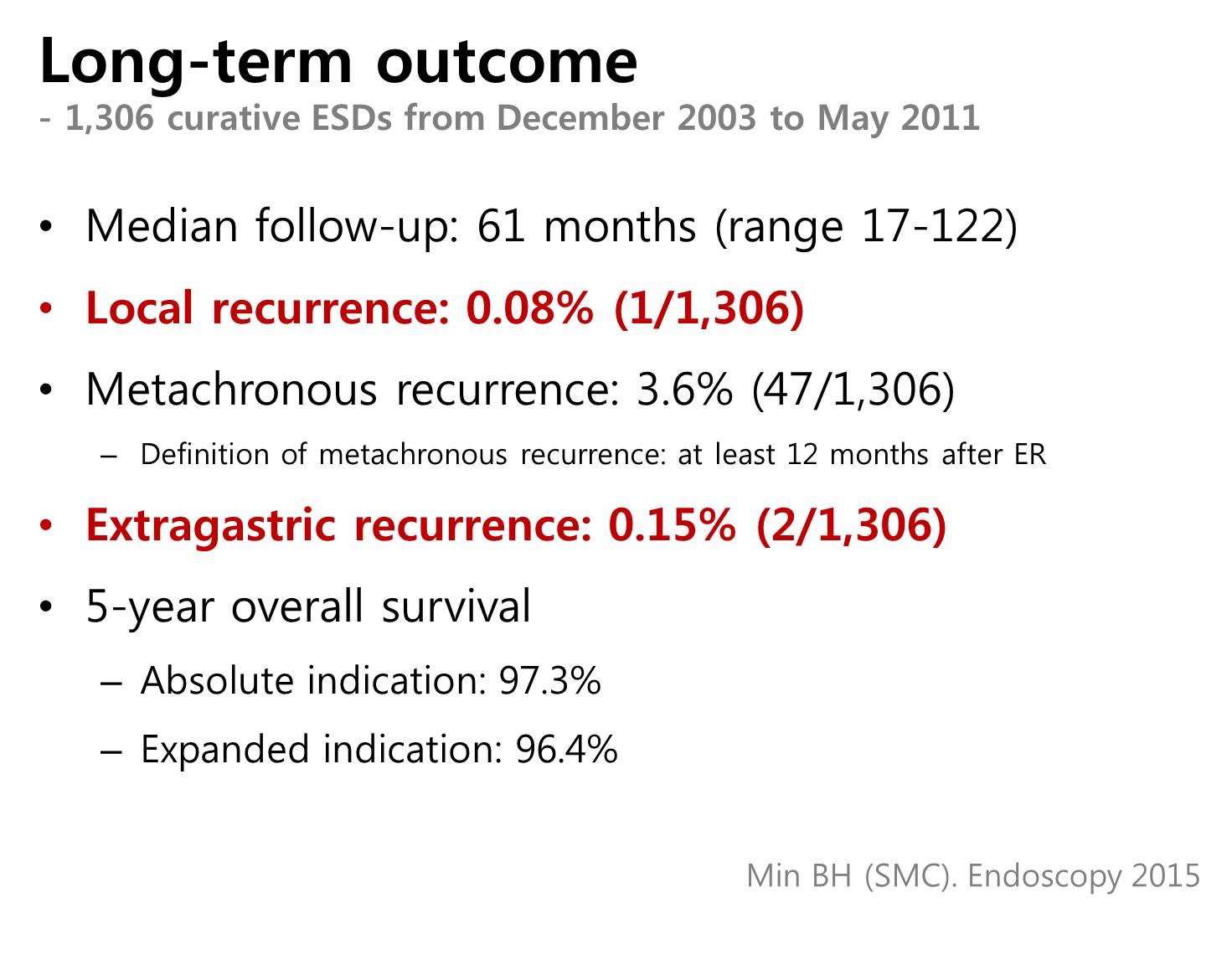
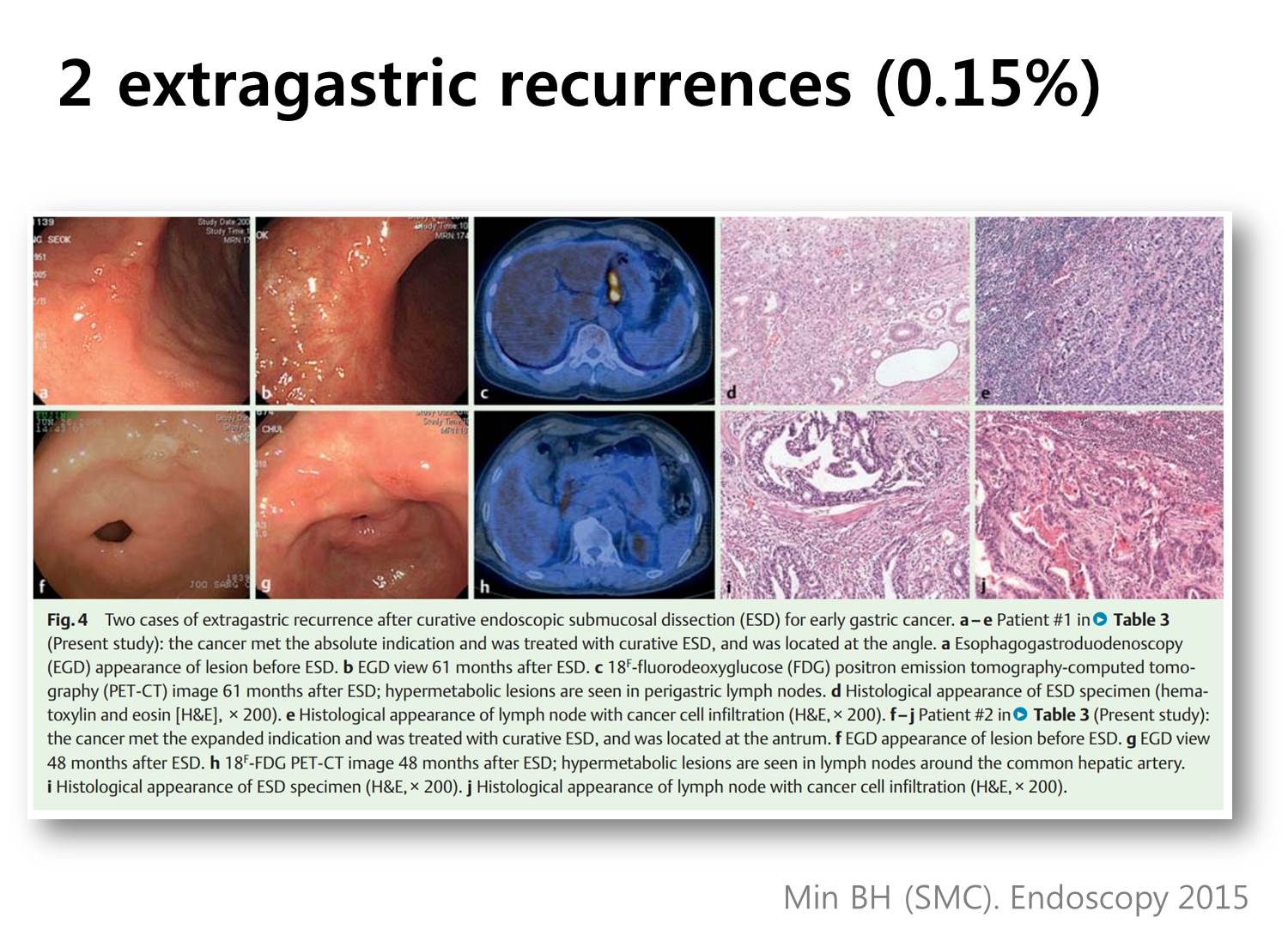
The median follow-up period was 61 months. Excluding metachronous recurrences, we experienced only one case (0.08%) of local recurrence, and 2 cases (0.15%) with extragastric recurrences. The 5-year survival rate was 97.3% for the absolute indication group and 96.4% for the expanded indication group.
The median follow-up period was 61 months. Excluding metachronous recurrences, we experienced only one case (0.08%) of local recurrence, and 2 cases (0.15%) with extragastric recurrences. The 5-year survival rate was 97.3% for the absolute indication group and 96.4% for the expanded indication group.
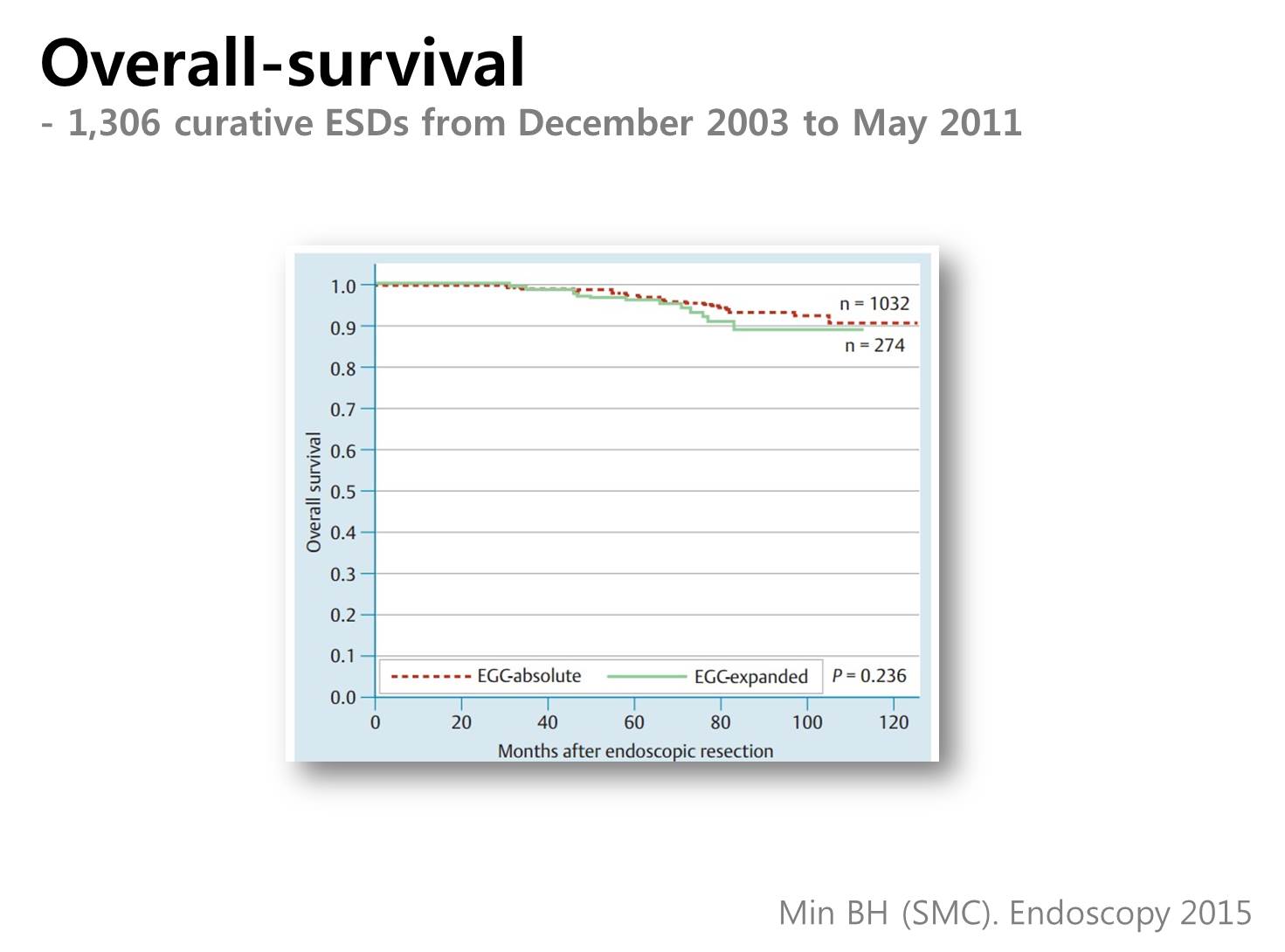
The red dot line is the absolute indication group and the green solid line is the expanded indication group. There was no statistical difference between them.
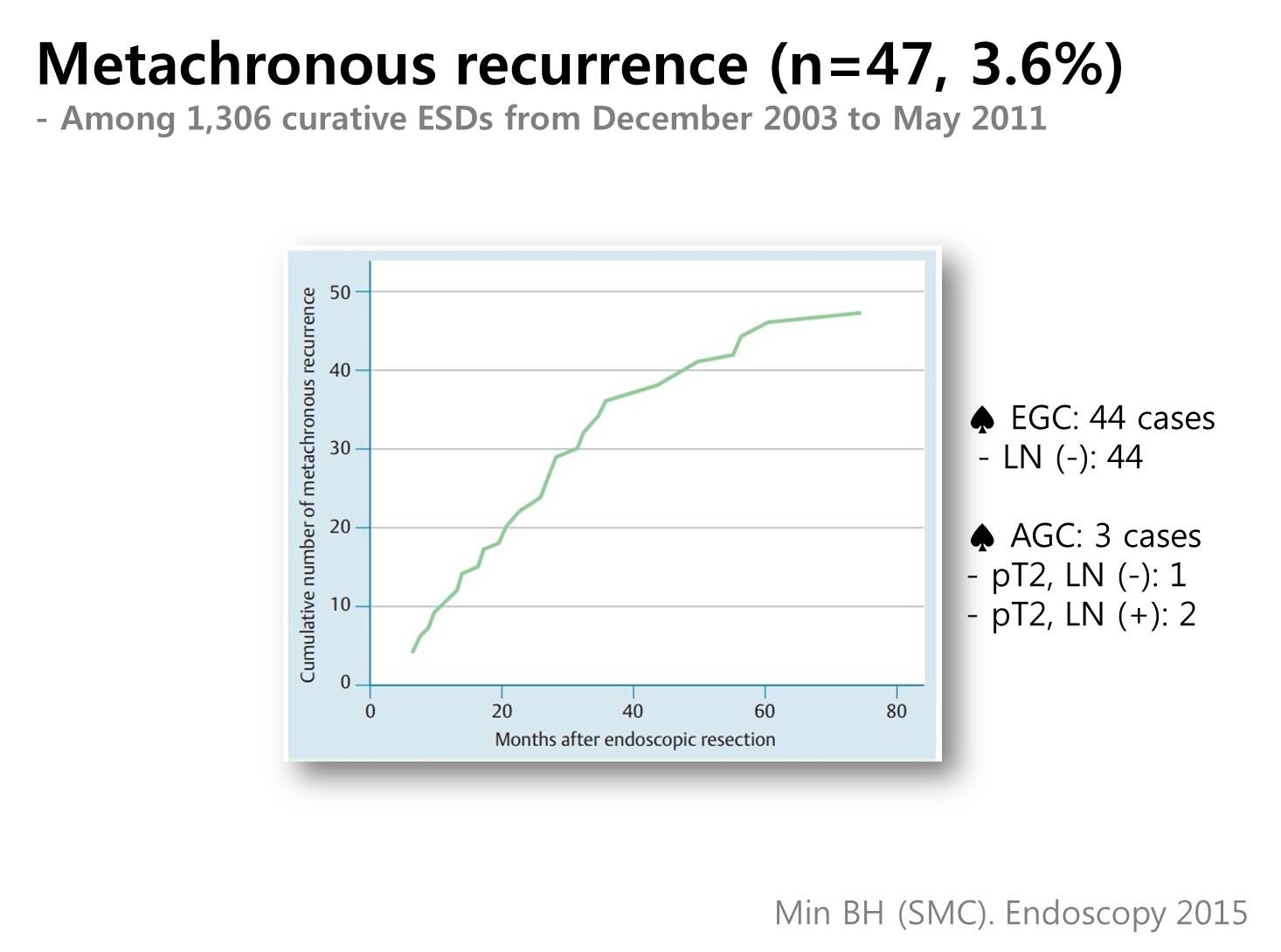
Metachronous recurrences occurred in 3.6% (47/1,306). The median interval from ESD to metachronous recurrence was 30 months. Forty-four metachronous cancers were early gastric cancers, and three were advanced gastric cancers. Sixty percent (28/47) were treated again by ESD, and others were treated by surgery.
![]() The next topic is non-curative resection.
The next topic is non-curative resection.
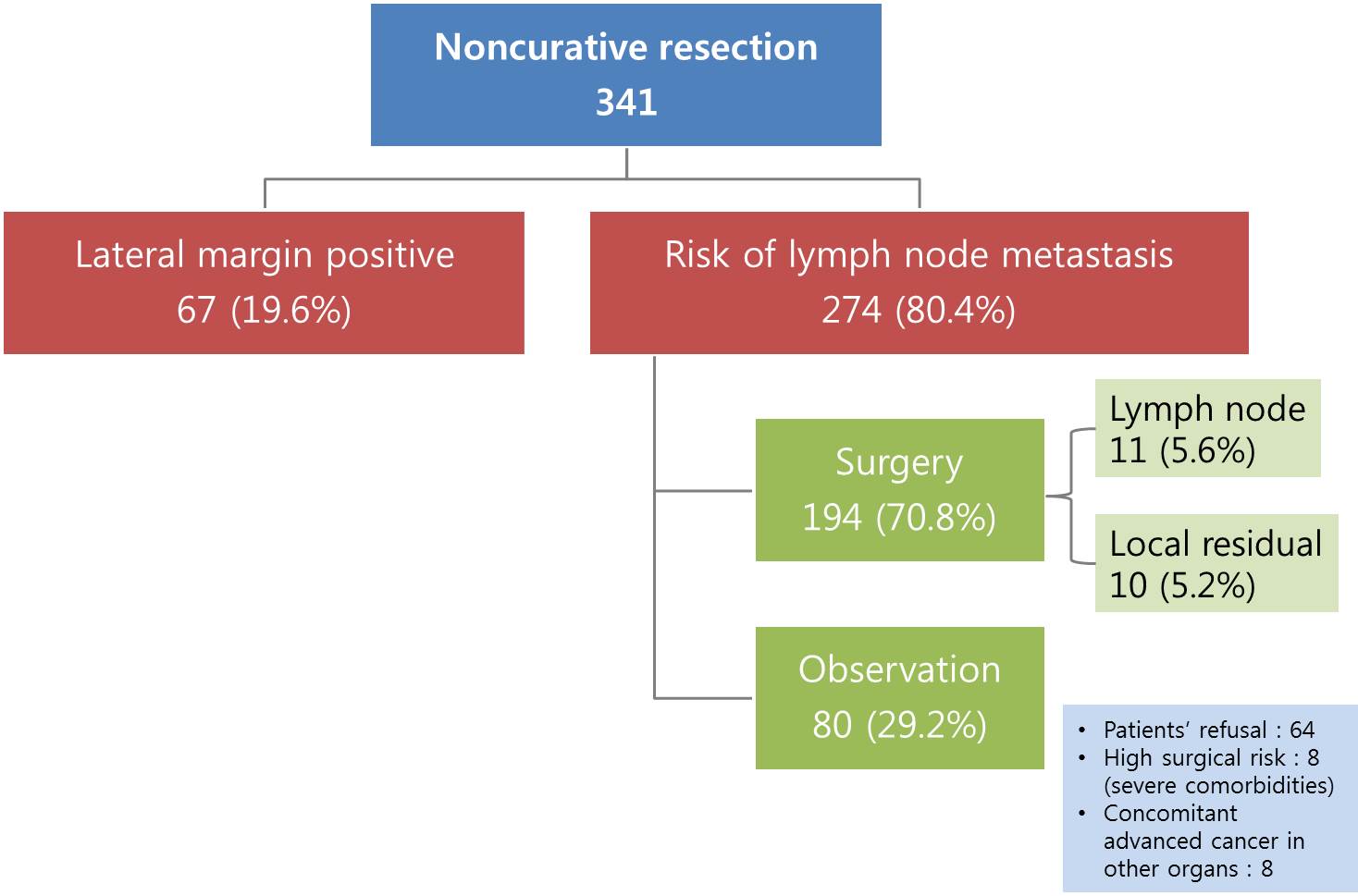
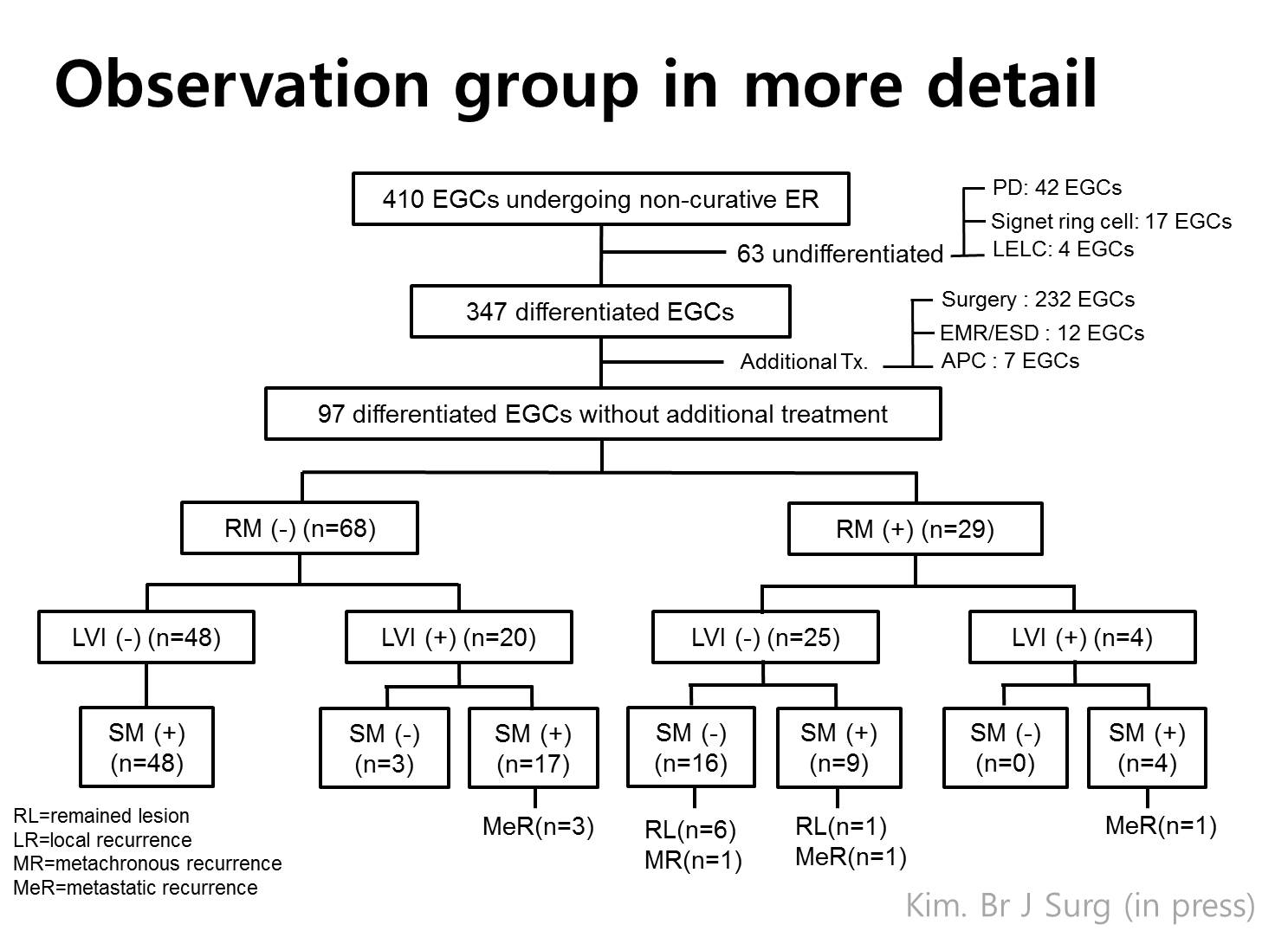
There are two subgroups in non-curative resection. One is lateral margin positive only group, and the other is cases with risk of lymph node metastasis. Lateral margin positive cases were excluded in this study, because most of them are treated by additional endoscopy. In cases with risk of lymph node metastasis, 70% were operated, and 30% were observed without surgery. The main reason of observation is patient’s refusal to surgery.
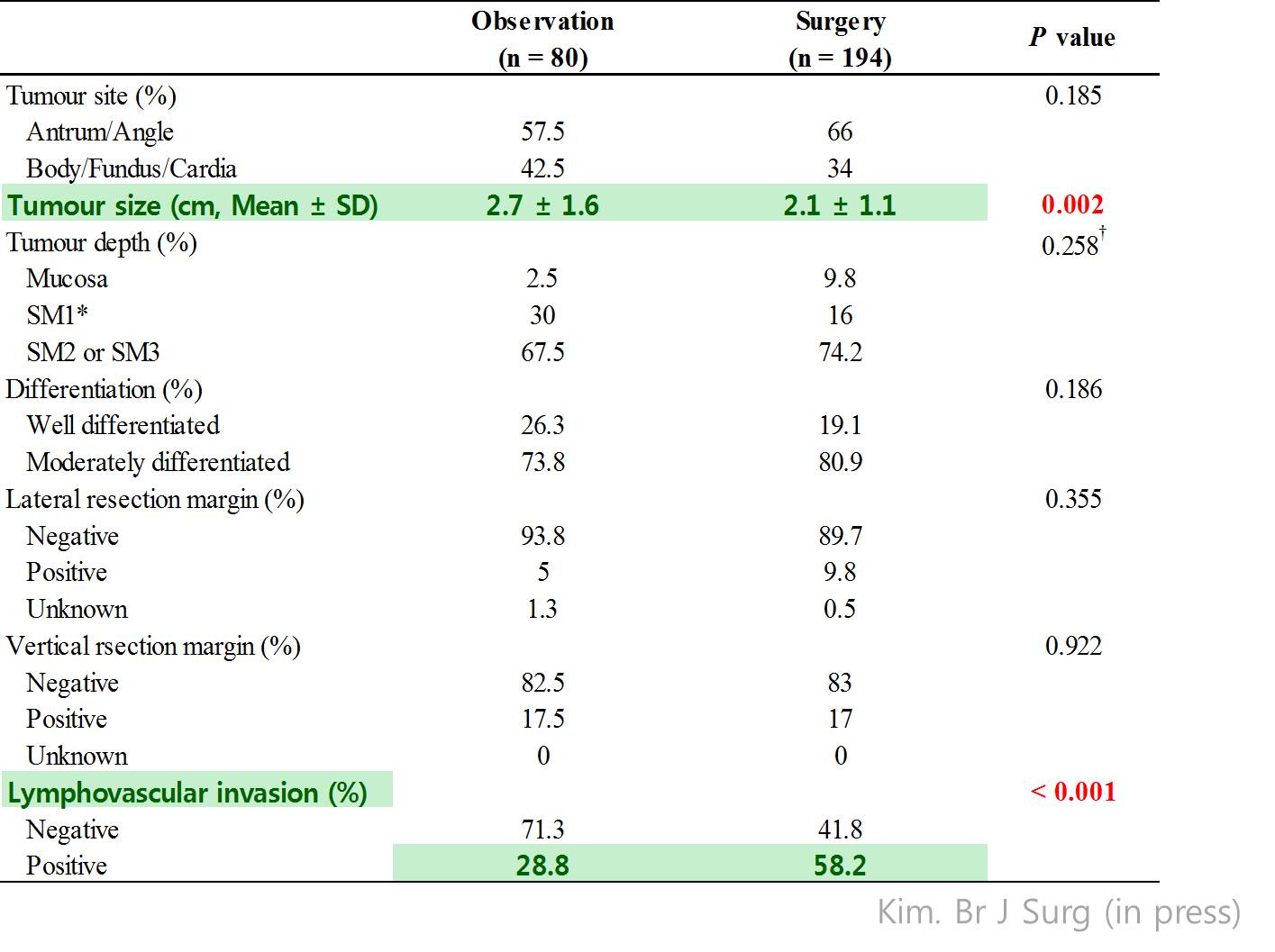
And have bigger tumor. The rate of lymphovascular invasion was higher in the surgery group.
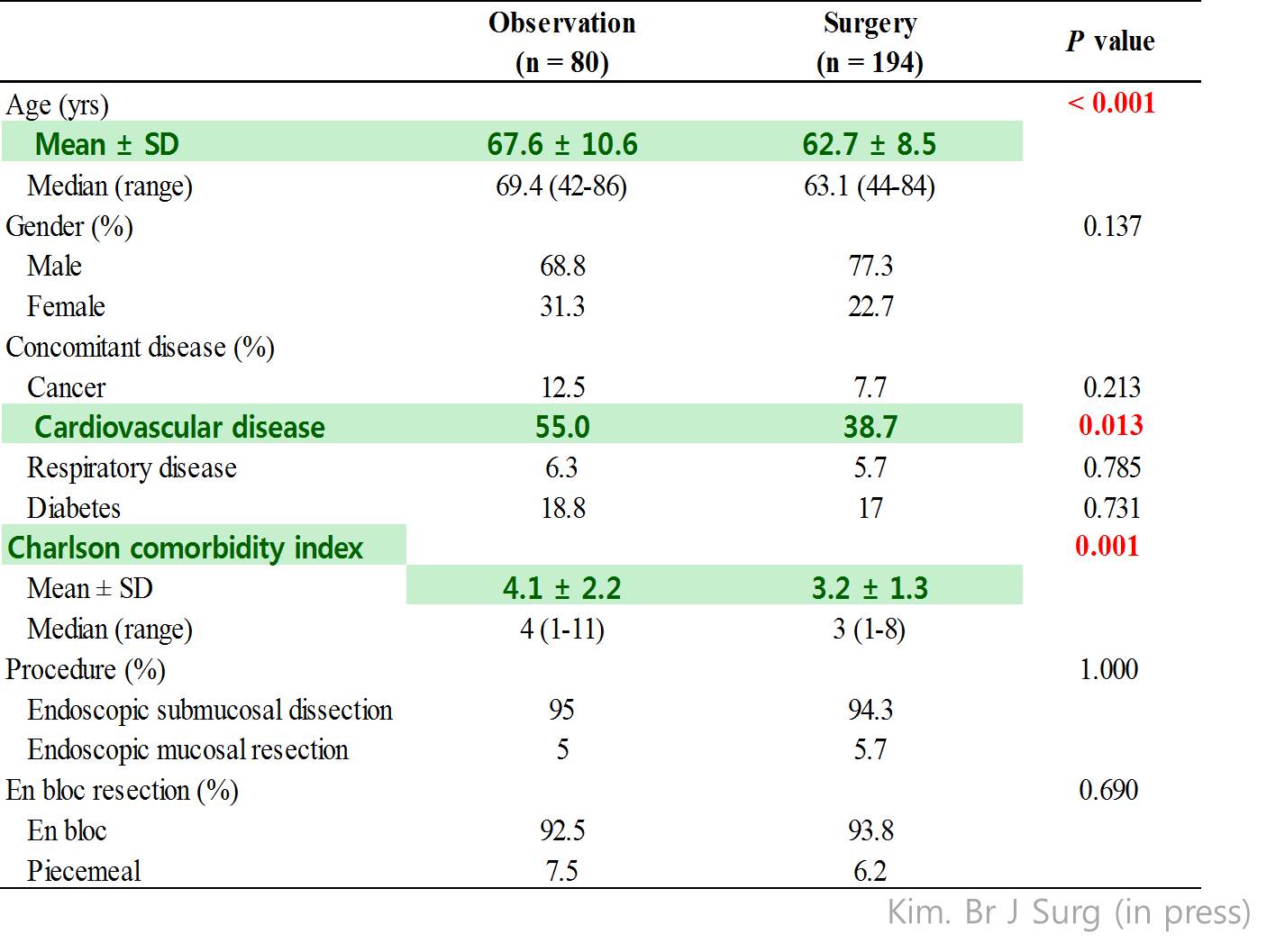
When we compared the two groups, patients in the observation group were older and have more cardiovascular diseases, and have higher Charlson comorbidity score…
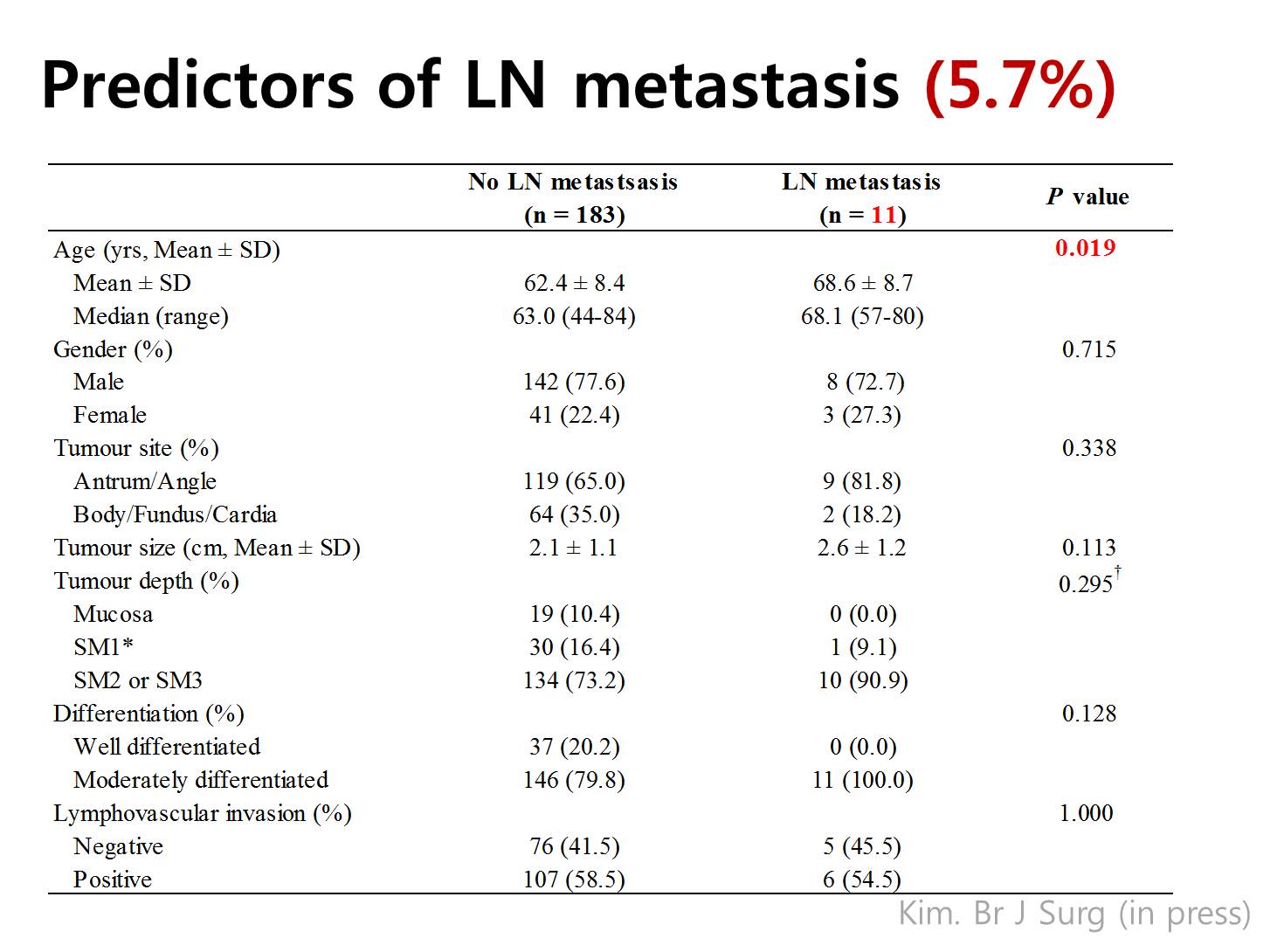
In the surgery group, 11 have lymph node metastasis, which means 5.7%. Patients with lymph node metastasis were older. To our surprise, the rate of lymph node metastasis was not different by the tumor size, depth of invasion, histological differentiation, and lymphovascular invasion in the endoscopically resected specimen. So, basically we found no predictor of lymph node metastasis in this analysis.
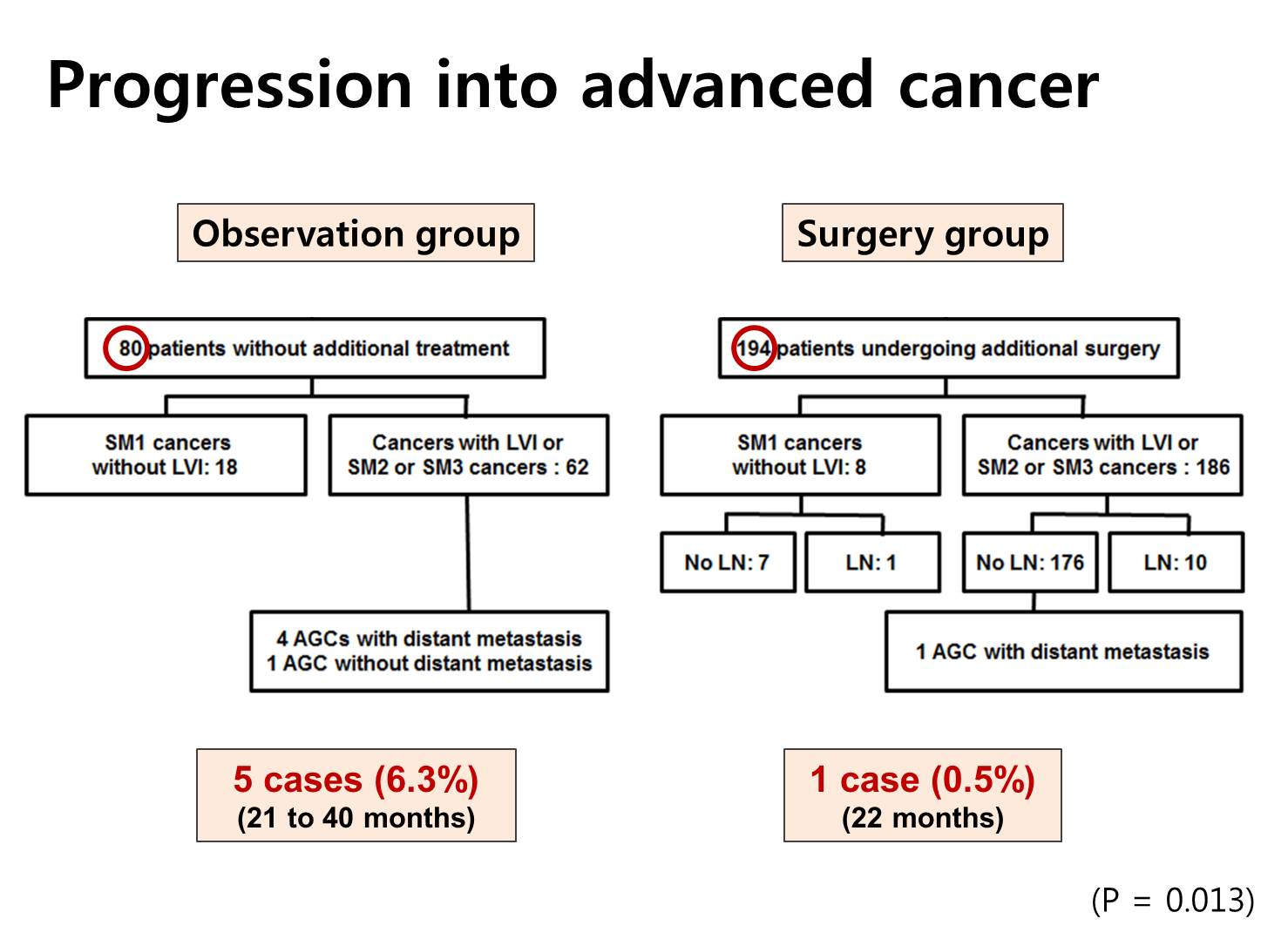
Rate of progression into the advanced cancers were different between 2 groups. Five advanced cancers were found in the observation group, and only one metastatic disease was found in the surgery group. This difference - 6.3% versus 0.5% - was statistically significant.
Oh, this is too complicated. I would skip it.
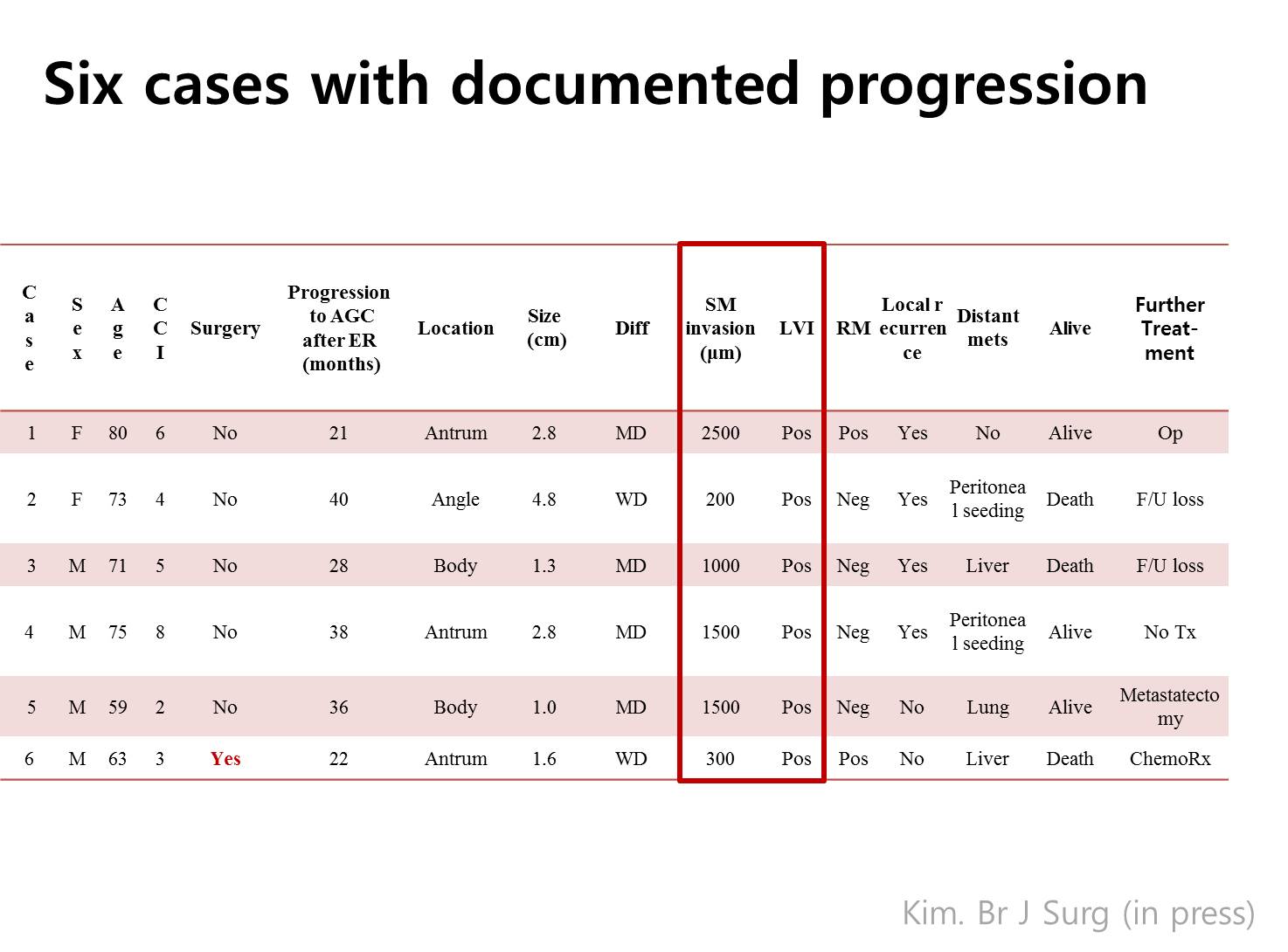
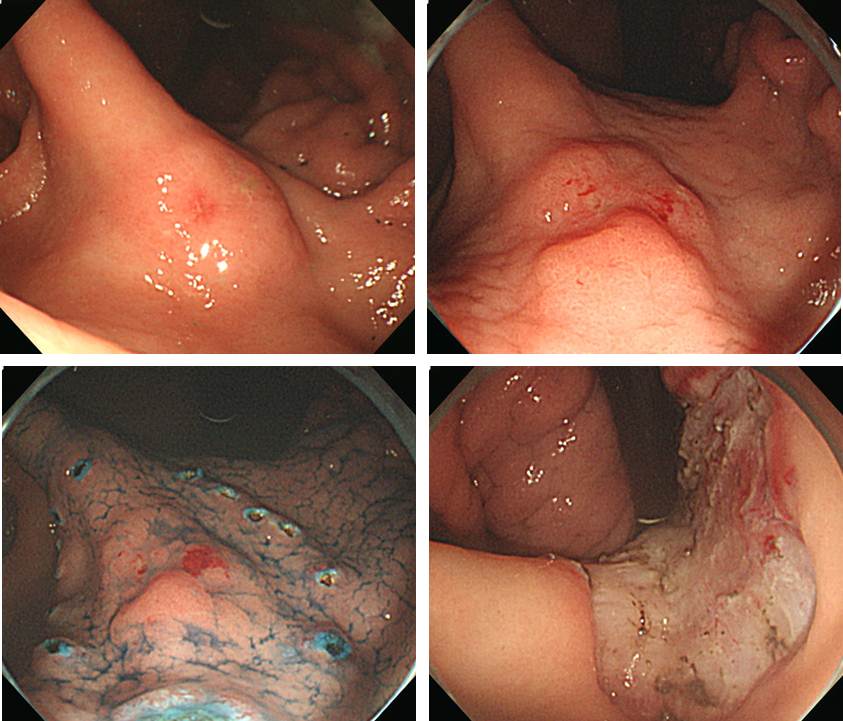
This is the summary of six cases with documented progression of gastric cancer. As you can see, all cases have submucosal invasion of more than 200 micrometer and all have evidence of endolymphatic invasion.
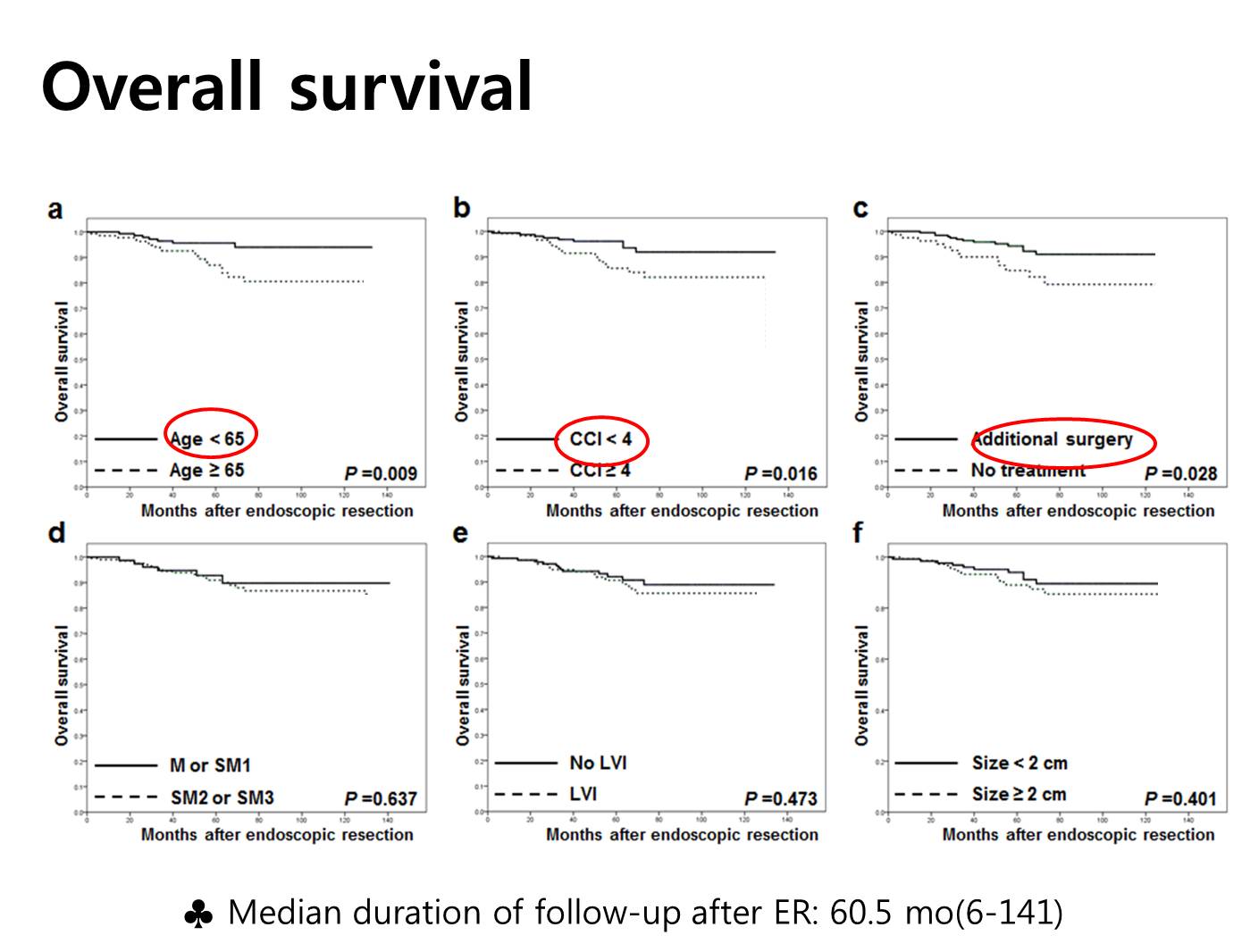
The next two slides are the main findings of this study. We compared the overall survival by some factors. As you can see in the figures, age less than 65, low Charlson score, and additional surgery were related with longer survival.
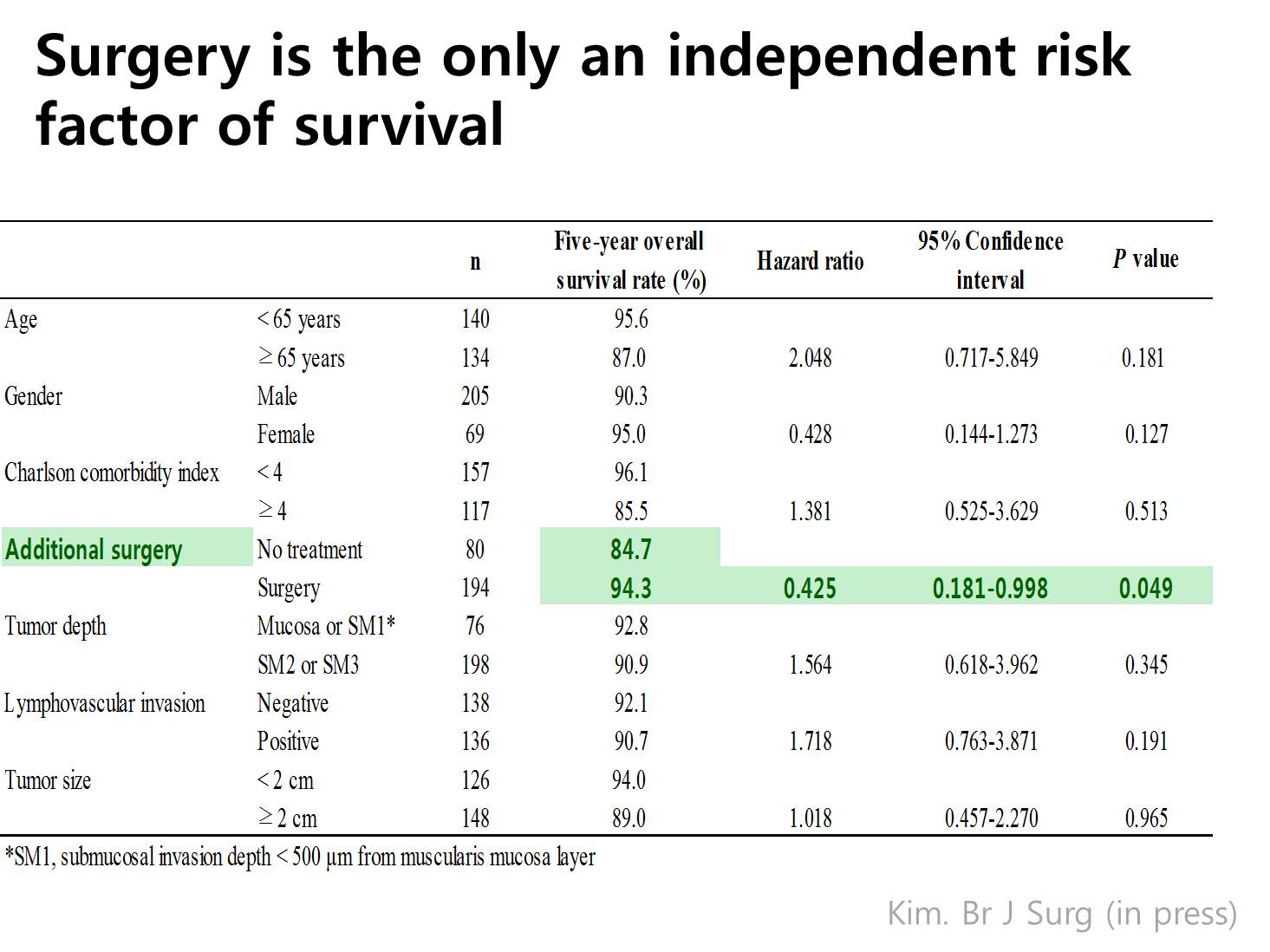
In the Cox proportional hazard model, additional surgery was the only significant independent factor related to the longer survival. So surgery was beneficial for patients with non-curative resection after ESD.
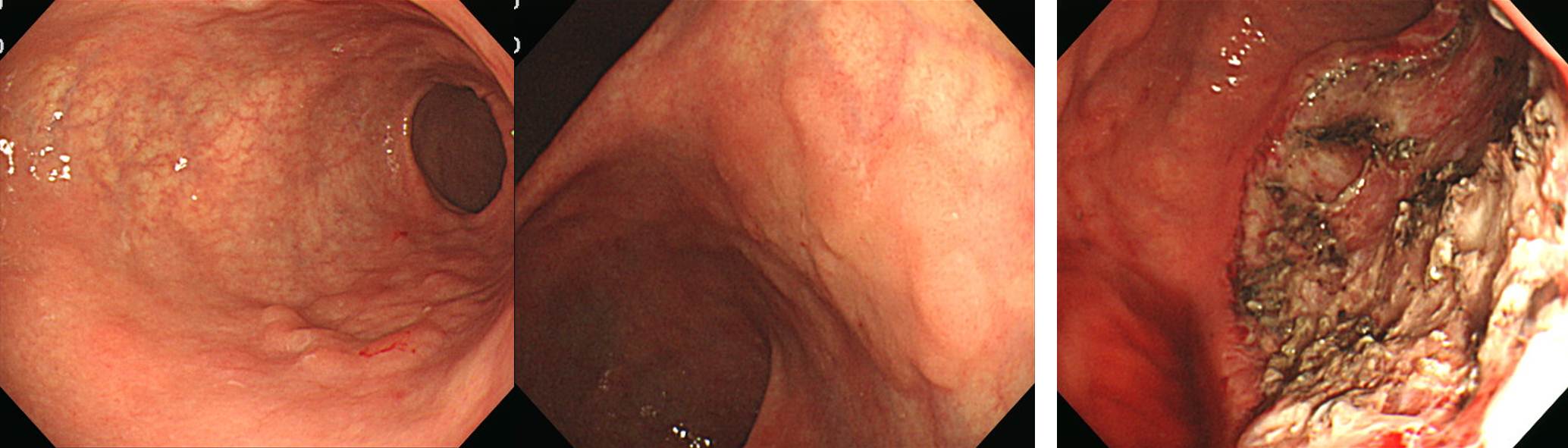
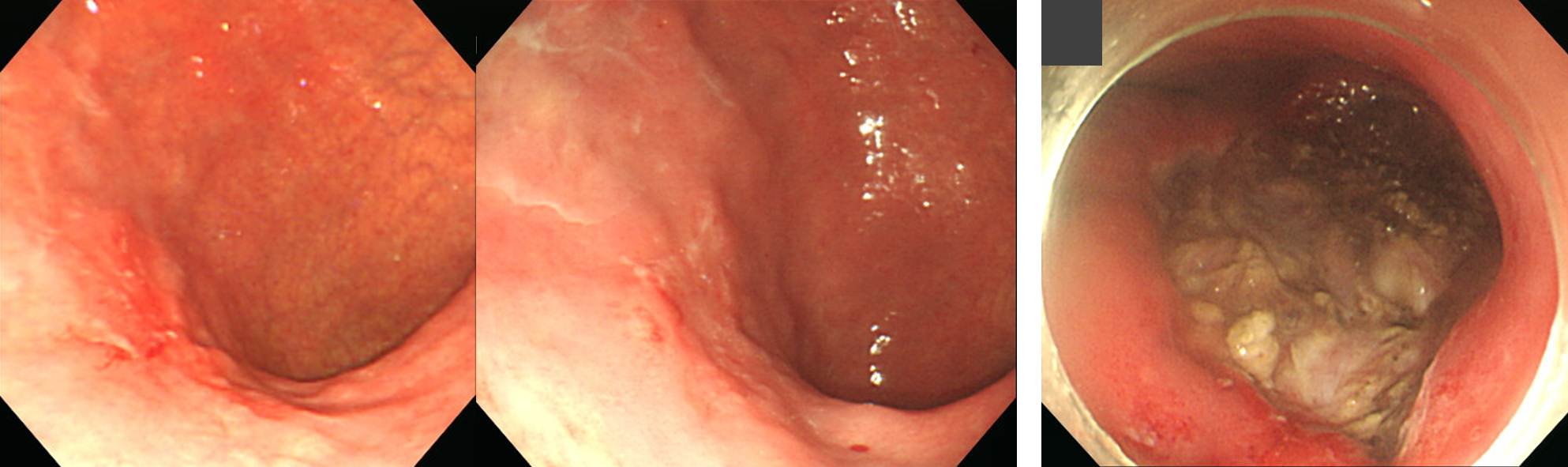
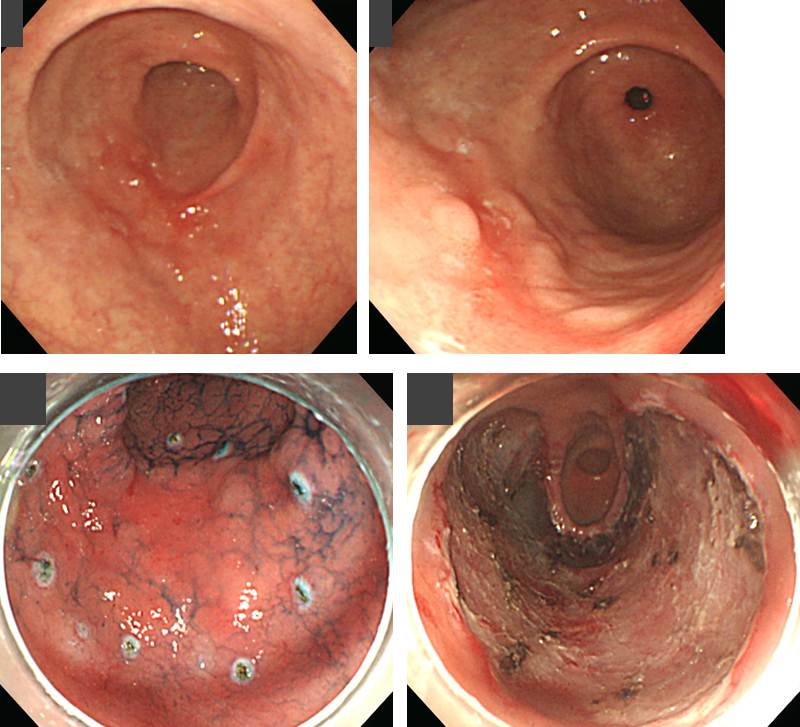
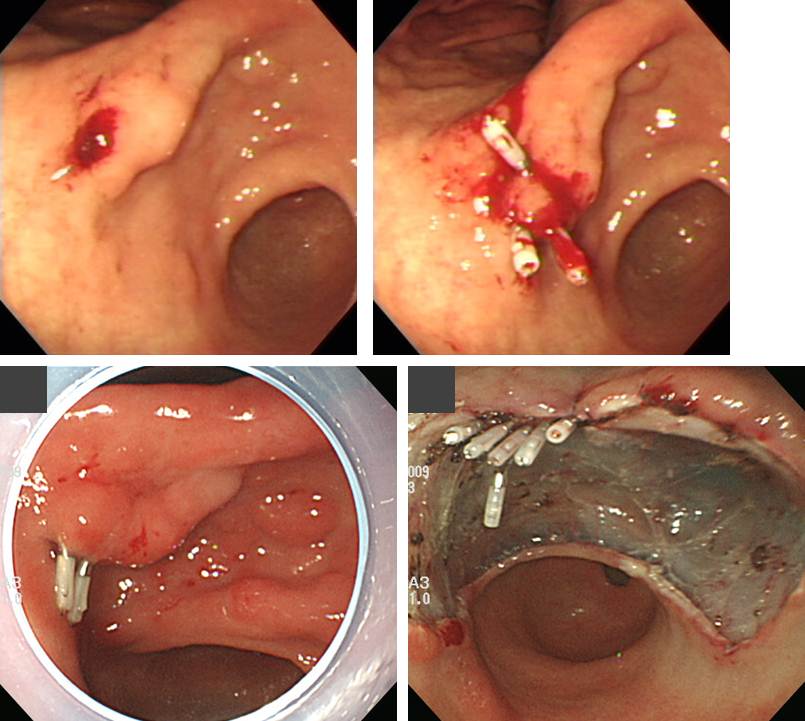
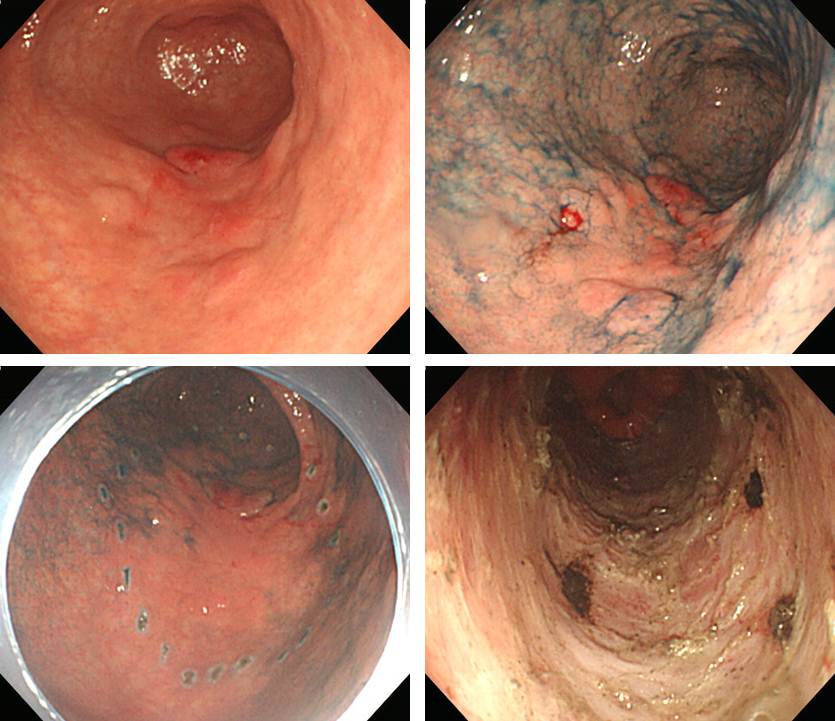
![]() Lymph node metastsis (+) cases in rescue surgery for non-curative endoscopic resection of EGC
Lymph node metastsis (+) cases in rescue surgery for non-curative endoscopic resection of EGC

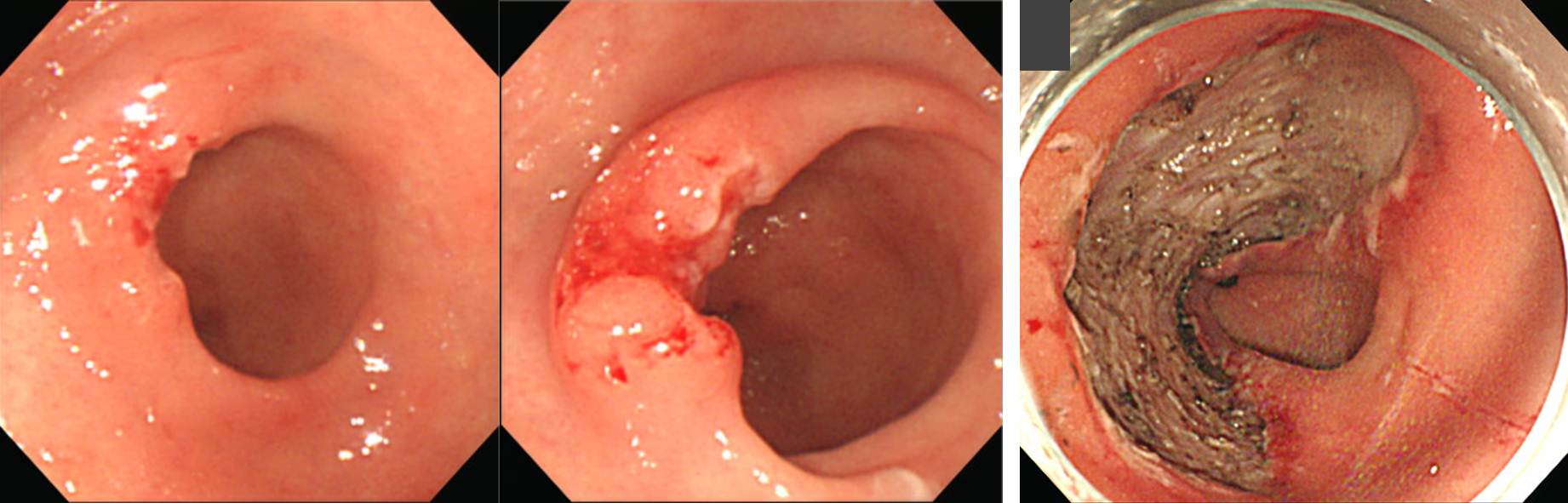
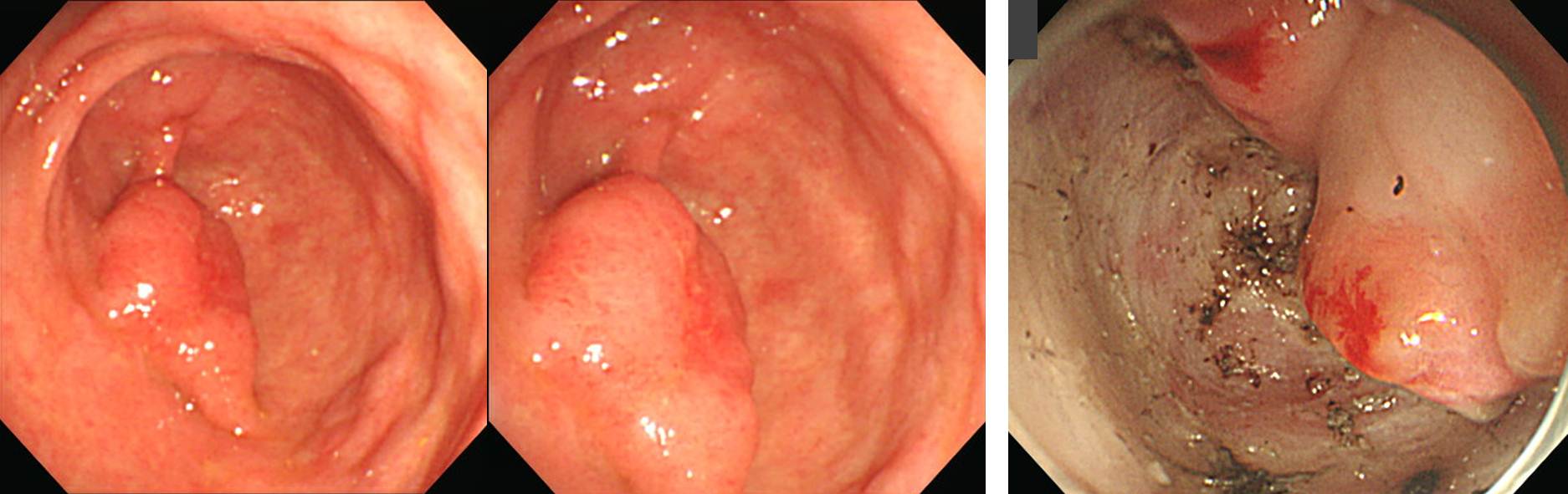
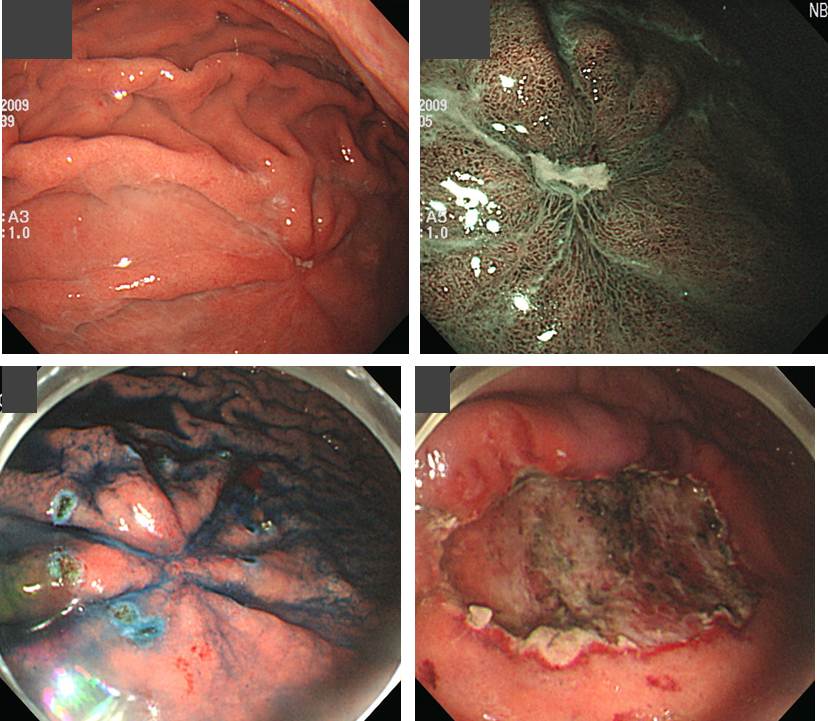
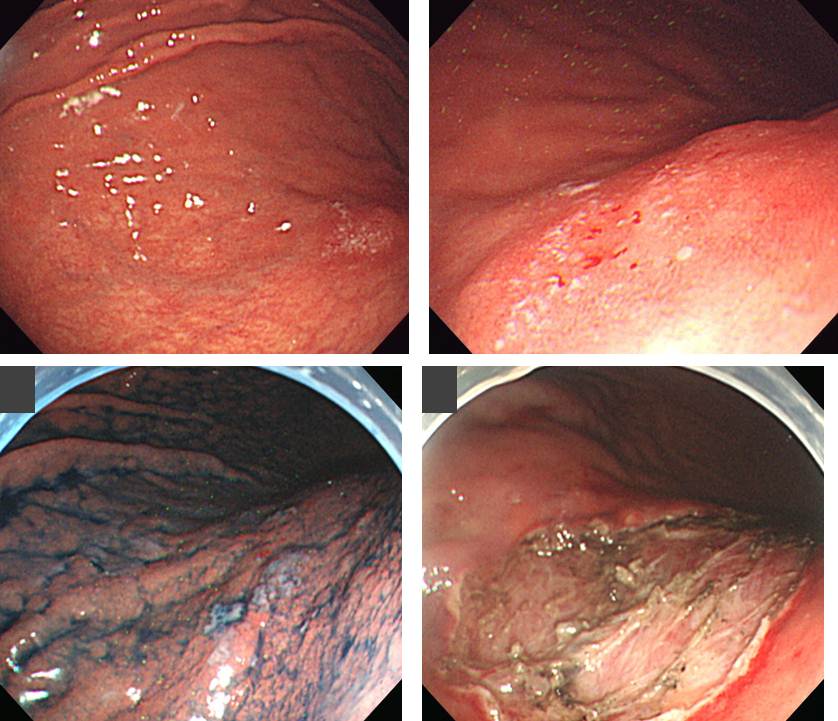
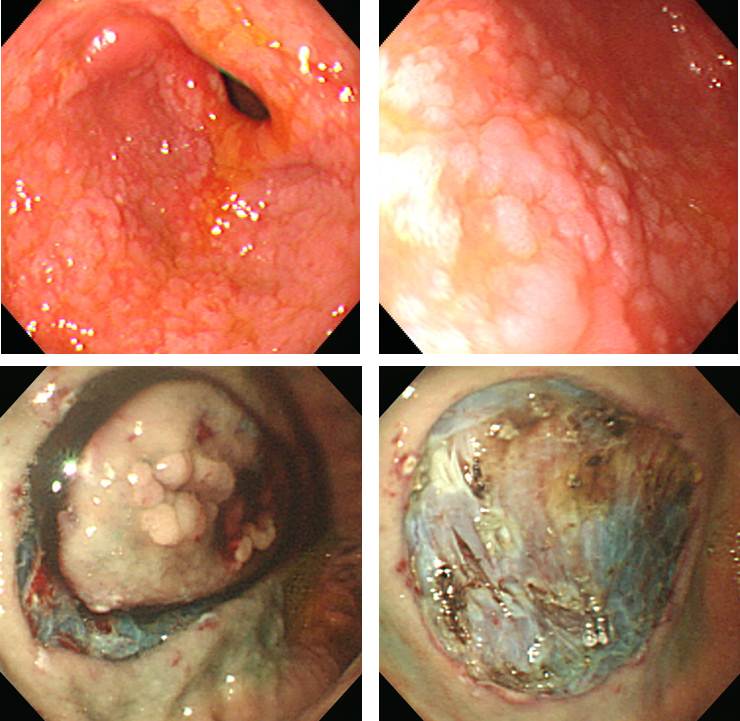
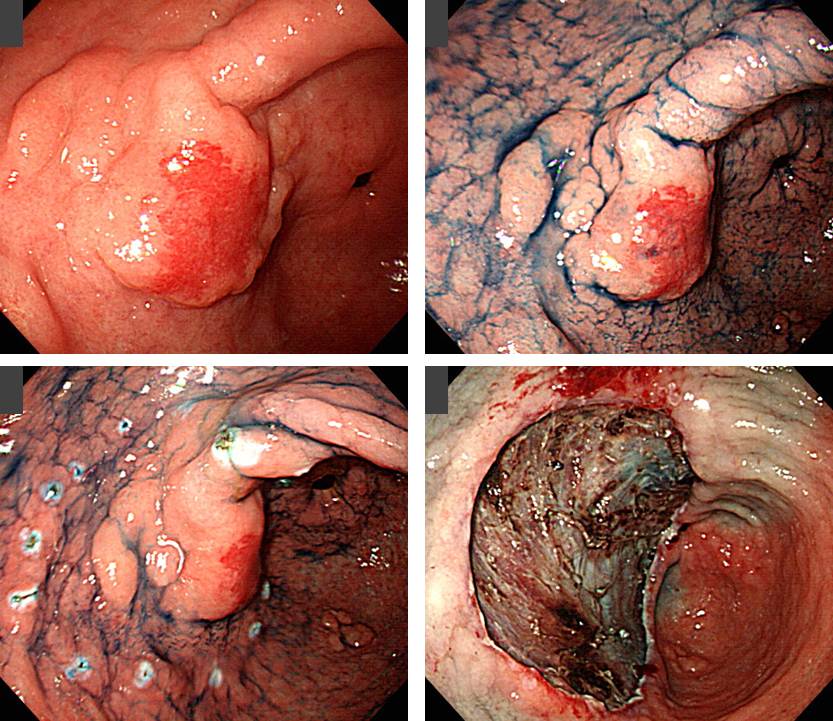
![]() Local residual tumor (+) cases in rescue surgery for non-curative endoscopic resection of EGC
Local residual tumor (+) cases in rescue surgery for non-curative endoscopic resection of EGC
This is the summary of the breakfast session. Pretreatment diagnostic group data need to be provided. Survival data with rate of follow-up loss is required. We can learn from failure cases. Let’s look at the dark side of the moon. Endoscopic pictures can give a lot of information
Thank you for your attention.
![]() © 더불어 바른 내시경 연구소 소장 이준행
© 더불어 바른 내시경 연구소 소장 이준행