EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [절제 변연 양성. Lateral margin positivity after ESD] - 終
[절제 변연 양성. Lateral margin positivity after ESD] - 終
2020-6-29.
1. Ratio of multiple lateral margin positivity in ESD specimen
2. Second ESD for positive lateral margin
3. Ablation treatment for positive lateral margin
4. Long-term outcomes of lateral margin positivity (SMC 장기 추적검사)
5. Lateral margin positive의 빈도, risk factor, outcome에 대한 여러 논문들
6. Scoring system에 근거한 치료방침 결정
7. 병리학적 고려 - EGC IIb의 병리학적 특징
9. Cases
10. FAQs
11. References
2023년 발표된 위암병리 가이드라인에는 아래와 같은 언급이 있습니다.
If the lateral margin is close (=<0.2cm) or is involved in the tumor, the corresponding directions should be written together.
![]() 1. [SMC experience] Ratio of multiple lateral margin positivity in ESD specimen
1. [SMC experience] Ratio of multiple lateral margin positivity in ESD specimen
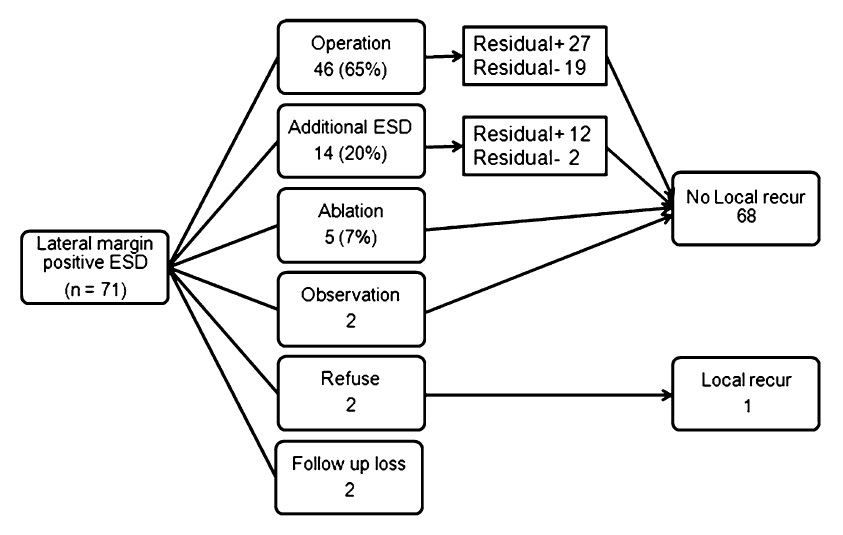
삼성서울병원에서 ESD 후 lateral margin positive였던 환자를 분석한 자료입니다. (Lee JH. Surg Endosc 2015) 많은 수고를 해 주신 이준희 선생님께 감사드립니다. 제1 저자와(이준희, Lee JH) 교신저자(이준행, Lee JH)의 initial이 같은 드문 경우입니다.^^
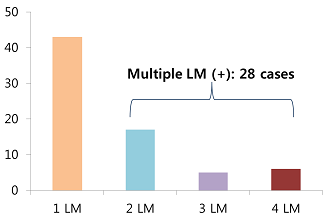
In our institution, lateral margin involvement is evaluated and reported in 4 directions. In about 14 hundred early gastric cancers treated by ESD, lateral margin involvement was documented in 5.5%. Among them, 60% were single lateral margin positive. 40% were multiple lateral margin positive.
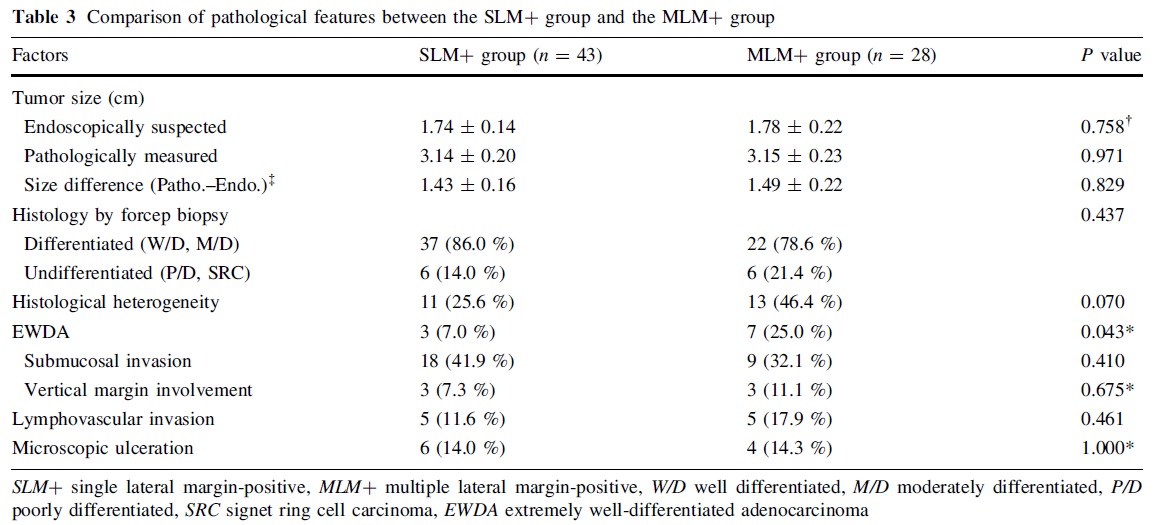
Histologic heterogeneity was seen in 25% and 46%, respectively. Extremely well differentiated adenocarcinoma was 7% and 25% in the two groups. This difference was statistically significant. Cases of technical difficulty was the same in the two groups. Surprisingly, the procedure time was shorter in the multiple lateral margin positive group. We thought that the technical aspect was not related to the number of positive lateral margin.
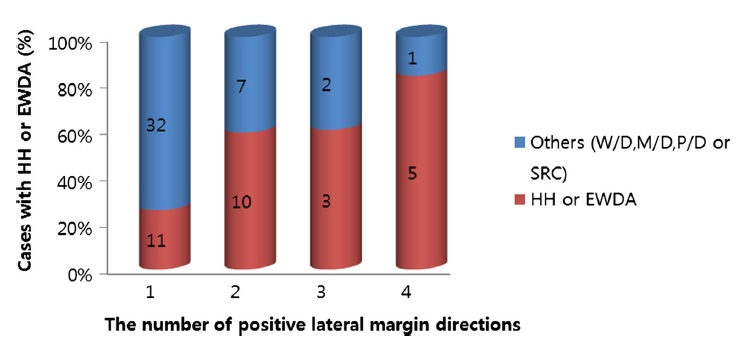
In this figure, yellow bar is the proportion of the cases with HH or EWDA. It showed that the ratio of HH or EWDA is increasing according to the number of lateral margin positive direction. And the difference was statistically significant.
결국 histologic heterogeneity 혹은 EWDA extremely well differentiated adenocarcinoma에서 multiple lateral margin involvement가 많았다는 것입니다. 가벼운 마음으로 아주 쉽게 ESD를 한 후 multiple lateral margin이 나오는 것인데 임상가로서는 상당히 당황스러운 일입니다.
치료 성적입니다. 치료를 받지 않은 환자 1명만 국소재발을 보였고 다른 환자들은 다양한 방법으로 잘 치료되었습니다.
![]() 2. [SMC experience] Second ESD for positive lateral margin
2. [SMC experience] Second ESD for positive lateral margin
삼성서울병원의 절제변연양성에 대한 second ESD의 초기 경험이 발표되었습니다. (Bae SY. GIE 2012) 최근에는 절제변연양성이 드물어서 자주 시행되지 않고 있는 시술입니다.
During the past 8 years, we performed 1,400 ESDs for early gastric cancers. The overall rate of positive lateral resection margin was 5 percent. Early additional ESD was done in 16 cases. Curative resection by early additional ESD was possible in all cases except one case. In the additional ESD pathology, residual cancers were found in 10 cases. There was no residual tumor in 3 cases. We thought that early additional ESD is quite useful in selected cases with positive resection margin.
![]() 3. [SMC experience] Ablation treatment for positive lateral margin (EndoTODAY 20121220)
3. [SMC experience] Ablation treatment for positive lateral margin (EndoTODAY 20121220)
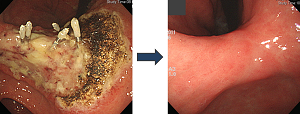
In cases with lateral margin involvement after ESD, early additional ablation treatment is another important treatment option. In this case, posterior resection margin was positive of malignancy.
Although no residual tumor was suspected in the repeat endoscopy, ablation treatment using argon plasma coagulation (APC) was done. There was no recurrence in the follow-up endoscopies for more than 4 years.
A few weeks ago, I received a question about the safety of ablation treatment of positive resection margin. The point was that we don’t know the depth of invasion of the possible residual tumor near the positive resection margin. Let’s suppose this is the tumor.
Endoscopic resection will be done like this, and one resection margin was positive. Yes, I agree. We don’t have the information about the depth of invasion of the possible residual tumor. However, we already have information of depth of invasion from most of the tumor. Usually the invasion is deepest in the middle of the tumor.
In this regard, ablation treatment (green area in the picture below) can be done quite safely.
![]() 4. [SMC experience] Long-term outcomes of lateral margin positivity
4. [SMC experience] Long-term outcomes of lateral margin positivity
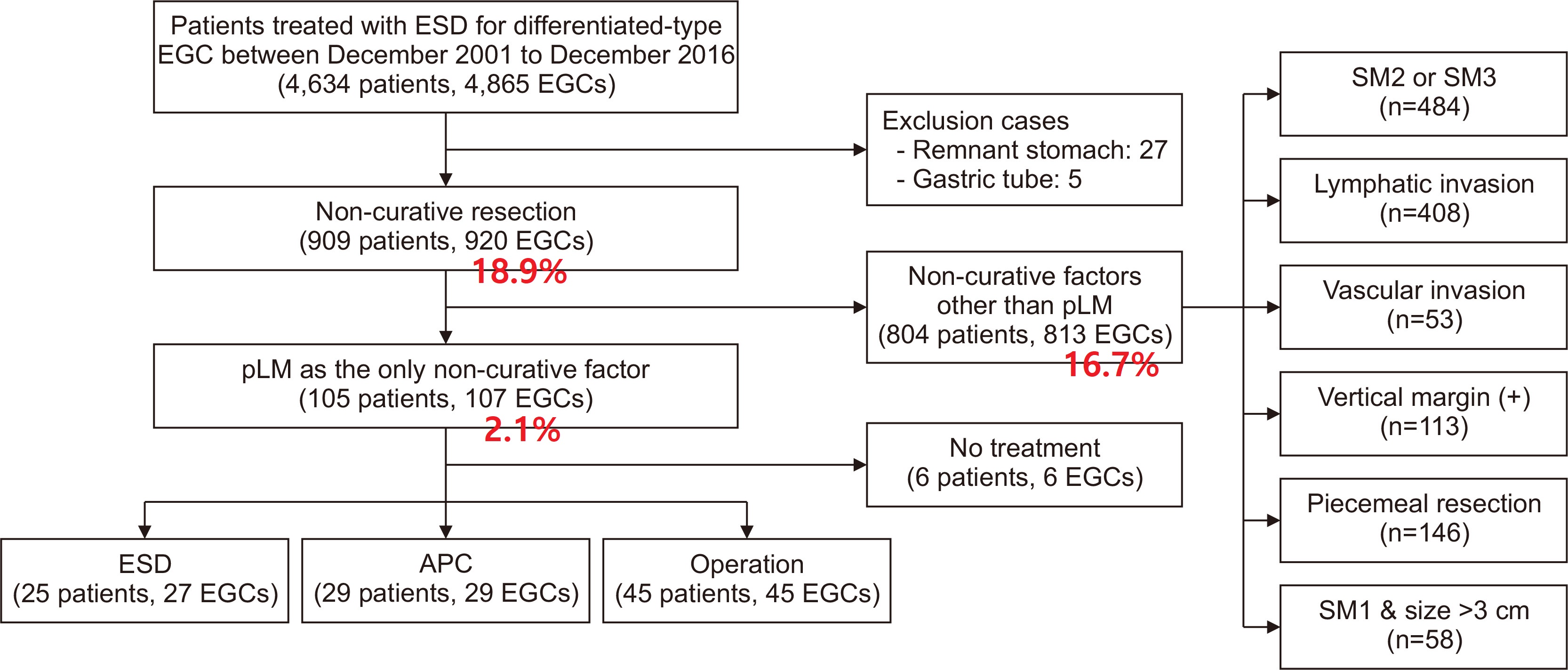
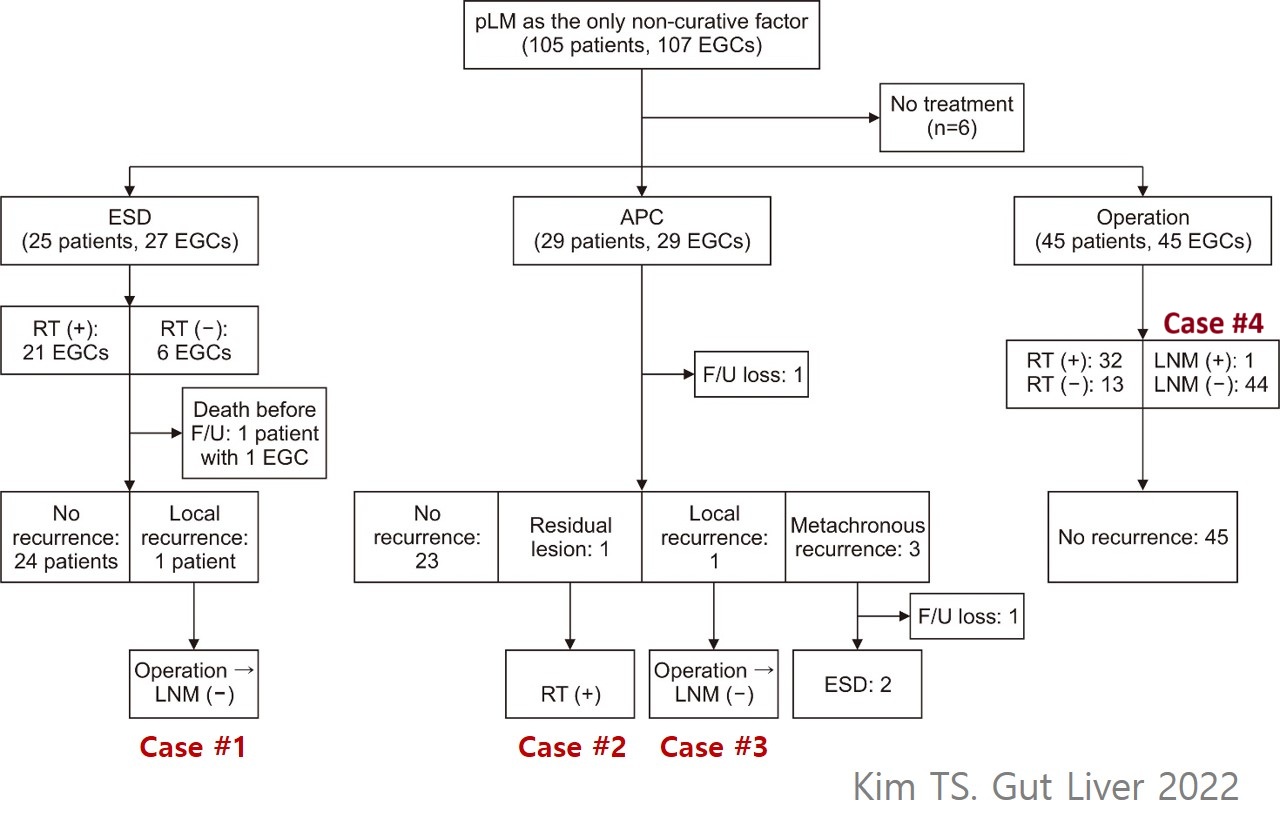
삼성서울병원의 절제변연 양성에 대한 장기 추적 결과가 발표되었습니다. (Kim TS. Gut Liver 2022)
절제변연 양성에 대한 ESD를 하였던 25명 중 1명에서, APC 을 하였던 29명 중 2명에서 recurrent/residual lesion이 발견되었습니다. 수술을 거부한 환자 한분을 제외하고 추가 치료로 모두 완치되었습니다.
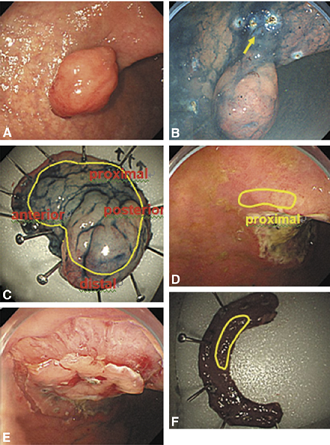
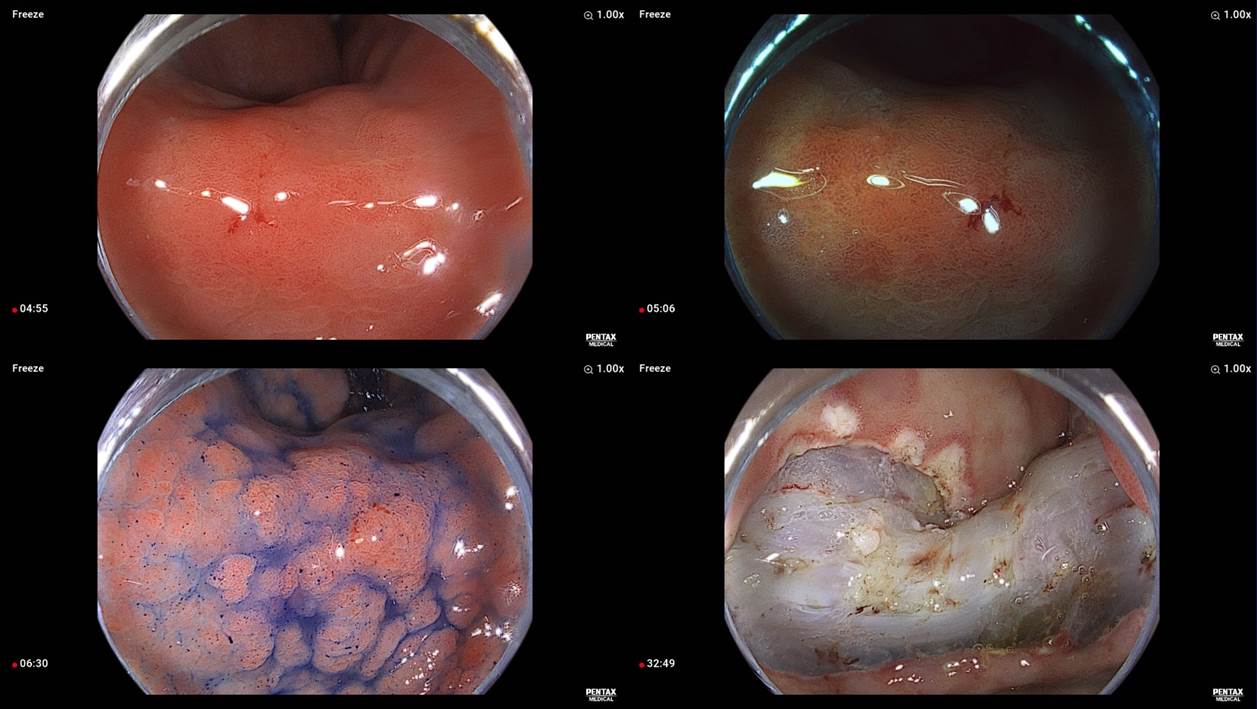
[증례 1, 2017년, 남자 58세] M/D 40mm LP암 2 lateral margins (proximal, anterior) invasion으로 ESD (8mm LP암)하였고 2년 후 국소재발로 수술 (3.1cm LP암)
첫 ESD
두번째 ESD
국소재발암 발견 시 내시경
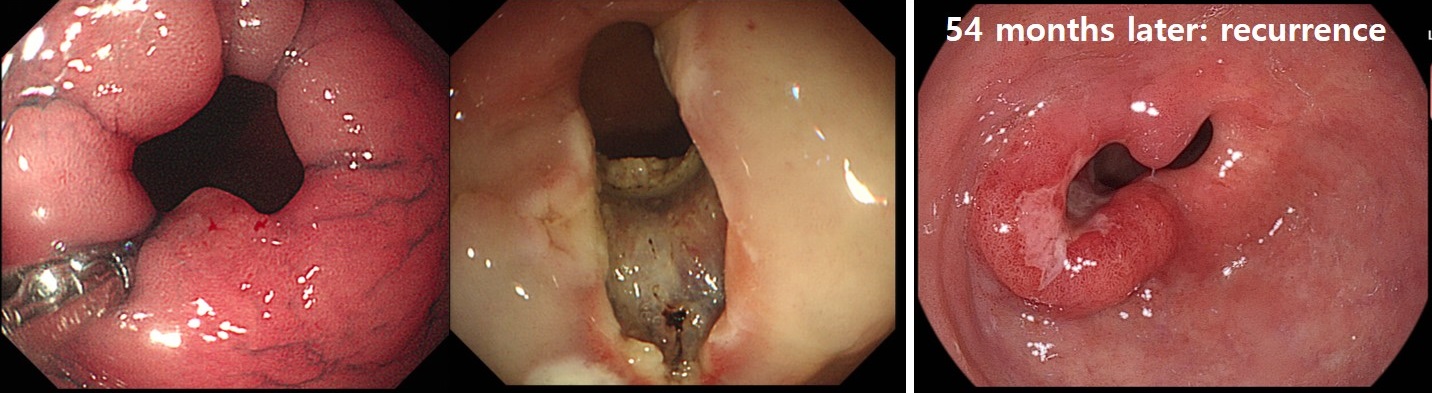
[증례 2, 2014년, 여자 80세] 날문 M/D 8mm LP암 2 lateral margin invasion. APC 시행. 54개월 후 국소 재발 발견
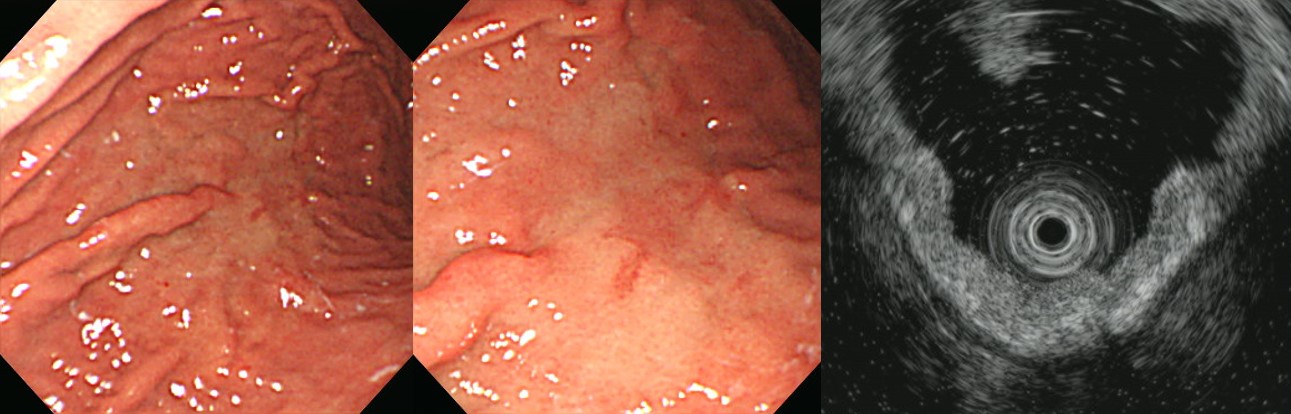
[증례 3, 2020년, 남자 75세] W/D 12mm MM암 1 laterl margin (distal) invasion으로 APC 시행. 16개월 후 국소재발로 수술 (1.5cm LP암)
ESD
APC
국소재발암 발견 시 내시경
[증례 4] Lateral margin only 였는데 수술 후 림프절 전이가 있던 증례. Expended indication이고 미분화 혼재암이었음
![]() 5. Lateral margin positive의 빈도, risk factor, outcome에 대한 여러 논문들
5. Lateral margin positive의 빈도, risk factor, outcome에 대한 여러 논문들
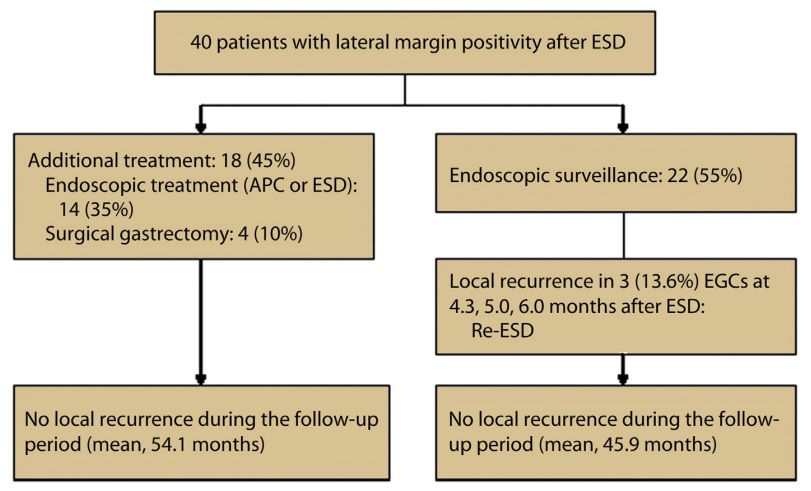
2012년 순천향대학교 부천병원 홍수진 교수님 팀에서 조기위암 내시경 치료 후 lateral margin positive 증례의 빈도와 outcome을 case series로 발표하셨습니다 (Han JP. GIE 2012). Expanded indication 환자의 비율이 높은 편이었고 따라서 lateral margin positive rate가 다소 높았습니다. 약 절반의 환자에서 일단 endoscopic surveillance 후 재발하면 적극적으로 ESD를 다시 시행하는 전략이었습니다. 효과적으로 잘 치료되었습니다.
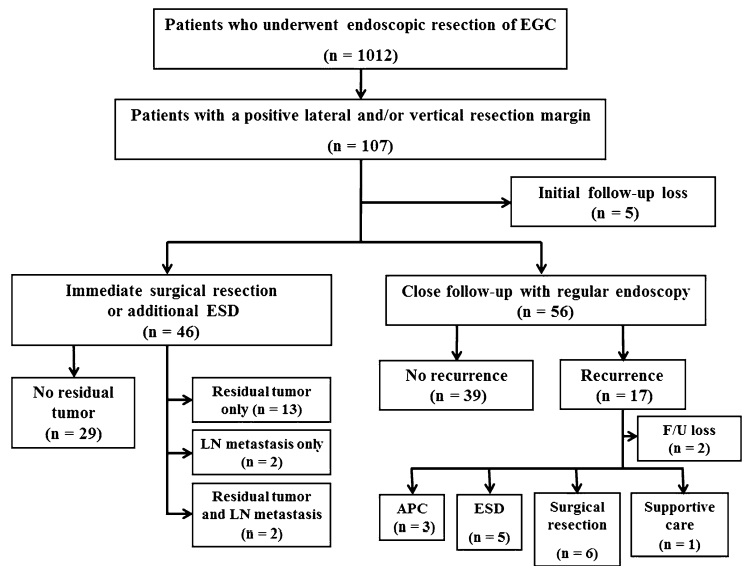
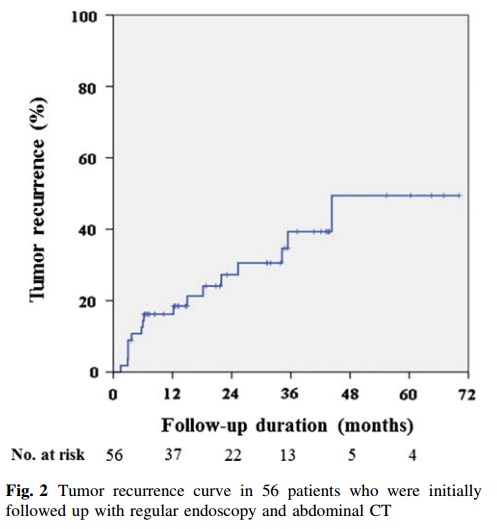
2013년 서울대학교병원 김상균 교수님 팀에서 조기위암 내시경 치료 후 resection margin positive 증례의 빈도와 outcome을 발표하였습니다 (Yoon H. Surg Endosc 2013). 아쉽게도 lateral margin positive와 deep margin positive가 섞여 있어서 다른 보고는 어려웠지만 lateral margin positive only는 5.3% (54/1,012)였습니다. 경과관찰 군에서 recurrence는 상당히 많았는데, deep margin positive 환자가 절반 이상이었기 때문에 lateral margin positive only 환자에서의 경과는 알 수 없었습니다.
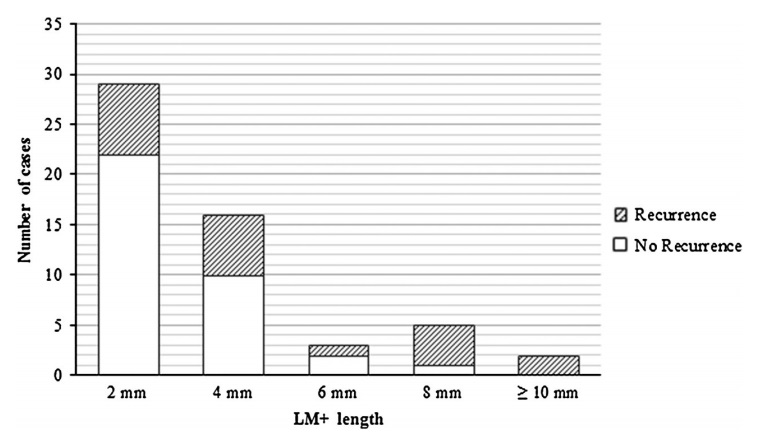
2014년 일본 동경암센터에서 경과관찰한 lateral margin positive 환자를 분석하여 6mm 이상 margin involvement가 있을 때 재발이 많다고 보고하였습니다 (Sekiguchi M. Endoscopy 2014). Enroll된 환자군을 잘 살펴볼 필요가 있어 보였습니다.
Among 3784 EGCs (3316 patients) treated by ESD between 1997 and 2010, 77 noncurative differentiated-type EGCs (75 patients) were retrospectively analyzed after meeting the following inclusion criteria: 1) the only noncurative factor was a cancer-positive lateral margin; 2) close observation was selected after the ESD; and 3) > 1 year follow-up after ESD.
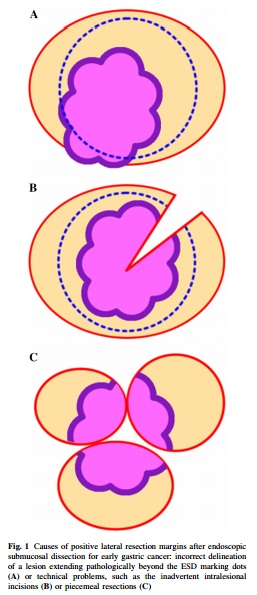
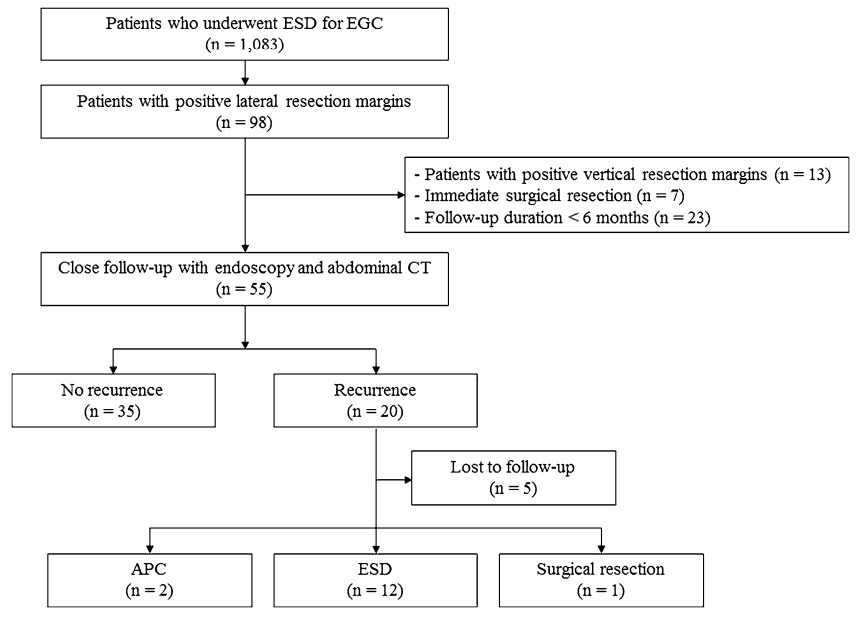
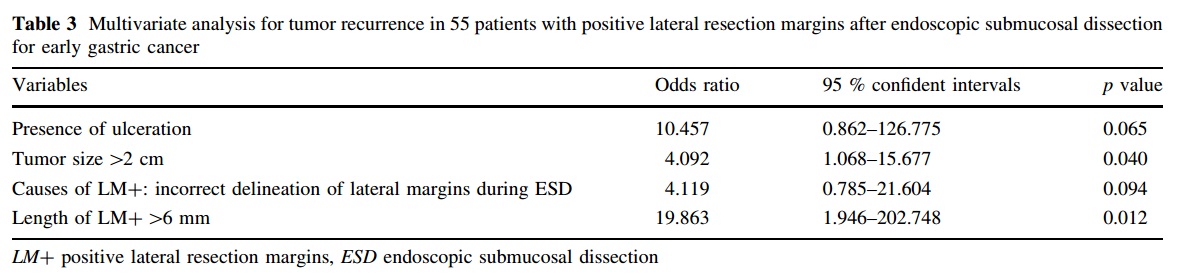
2015년 부산대병원 김광하 교수님 팀에서 조기위암 내시경치료 후 lateral margin positive에서 재발위험인자를 분석하였습니다 (Kim TK. Surg Endosc 2015). Lateral margin positive의 원인을 세가지로 나눈 점이 흥미로웠습니다.
![]() 6. Scoring system에 근거한 치료방침 결정
6. Scoring system에 근거한 치료방침 결정
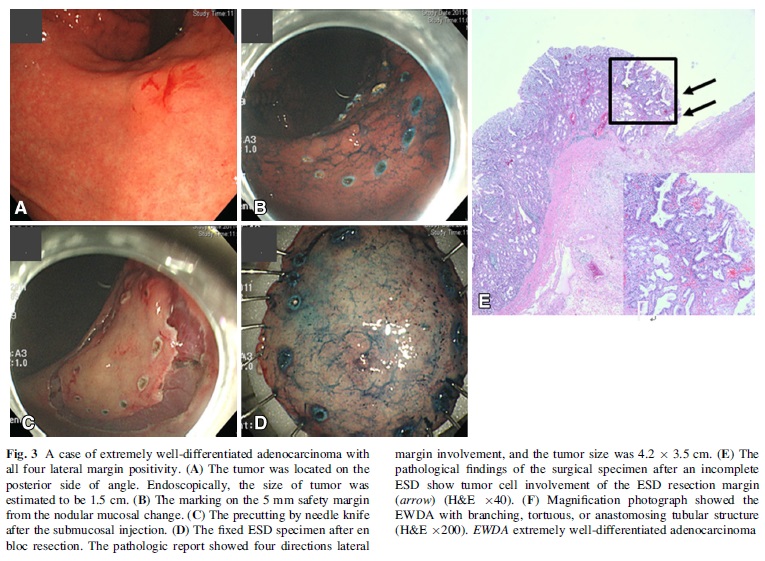
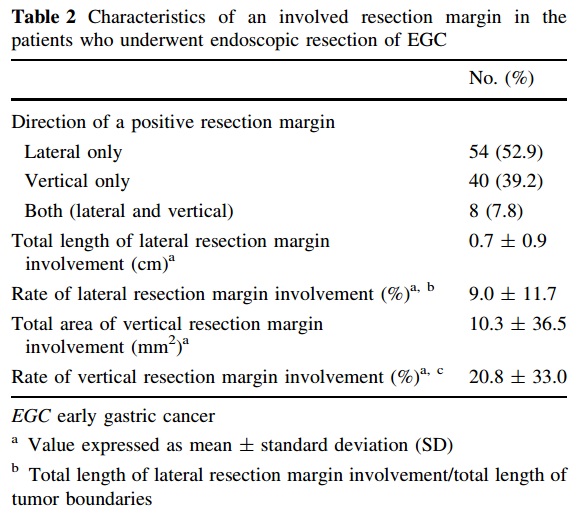
2015년 서울대학교 분당병원 박영수 교수님 팀에서 조기위암 내시경치료 후 lateral margin positive 증례에서 재발률을 분석하여 scoring system을 제안하였습니다 (Hwang JJ. Surg Endosc 2015 (Epub)). ESD가 아닌 EMR 증례가 포함되었고, lateral magin 이외의 incomplete resection 증례가 포함되었기 때문이겠지만 국소 잔류 병소나 국소 재발 빈도가 제법 높았습니다 (34.5%). Scoring system은 잘 만들어진 것 같습니다. 그러나 통상적인 병리 report form에 들어있지 않은 인자가 포함되었다는 점에서 실제적인 유용성은 다소 우려스럽습니다.
Eighty-two patients (84 lesions) with LRM+ after EMR (n = 45) or ESD (n = 39) were enrolled. Forty patients underwent additional gastrectomy or ESD, and 44 were closely observed. The residual/recurrent tumor rate was 34.5 % (29 of 84 lesions). Univariate analysis found that the residual/recurrent tumor was associated with the endoscopic resection type (EMR), undifferentiated histology, number of involved directions, rate of lateral resection margin involvement and the total length (mm) of the lateral resection margin involved by the tumor. In multivariate logistic regression analysis, undifferentiated histology and rate (%) were independent risk factors.
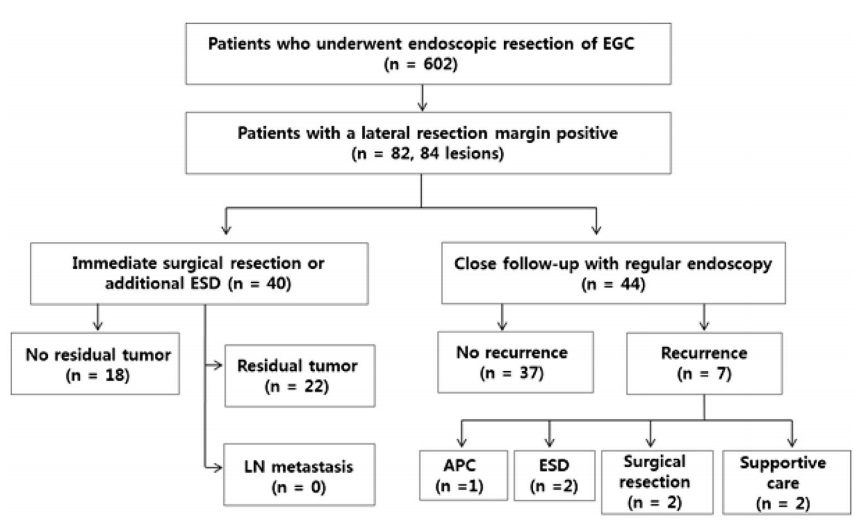
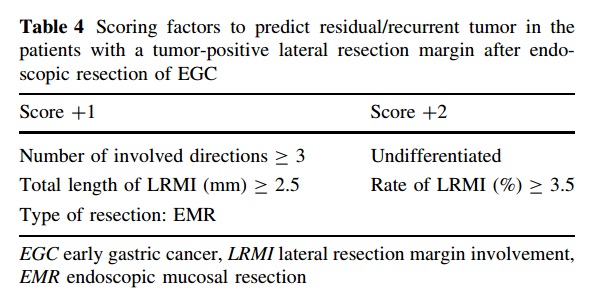
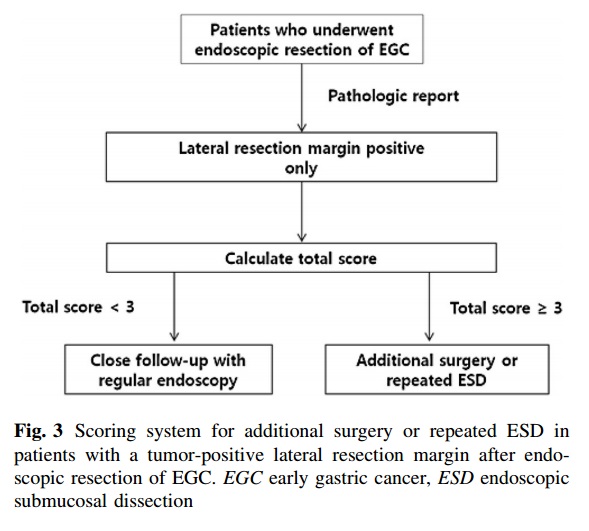
Figure 3에서 'lateral resection margin positive only'의 only를 주의해서 보시기 바랍니다. SM invasion이나 lymphatic invasion과 같은 risk of lymph node involvement 증례는 scoring system 적용 대상이 아닙니다. 수술을 권해야 하므로.
![]() 7. 병리학적 고려
7. 병리학적 고려
1) EGC IIb 면을 구성하는 암의 조직학적 특징 (위와 장 2010년 1월호 25쪽)
[참고] EGC IIb 면의 macro 소견은 위소구 명료화, 위소구 불명료화/소실, 위소구 조대화 (粗大化), Insel 모양 과립, 광택감 소실 등이다. Insel이란 섬 혹은 모래톱(shoal)을 의미하는 독일어로, IIc 함요내의 과립상 융기를 나타내는 용어이다. Insel은 미분화형 선암의 IIc 함요에서 관찰되는 빈도가 높고, IIc 함요내의 암침윤이 적은 부분이 상대적으로 융기함으로써 형성되는 일이 많다. IIb형 암에서도 Insel과 같은 과립상 융기가 관찰될 수 있다.
[참고] 포복형샘암종(crawling-type adenocarcinomas)은 종양세포의 핵이 저등급의 이형성을 보이고 불규칙하게 분지 혹은 융합되는 구조가 조직학적 특징인 종양으로 WHO 5판 분류에서 정식 아형으로 분류되어 있지는 않다. 이 암종은 핵의 이형성이 심하지 않고 내강 혹은 틈새 형태를 이루는 구조적 특성으로 인해 예전에는 고분화 샘암종으로 간주되었으나, 크기가 큰 포복형샘암종은 분화가 점막하층 이상으로 침윤을 보이는 경우 저응집암종 성분이 동반되는 경우가 많으며, 림프절 전이가 흔하여 다른 아형에 비해 예후가 안 좋을 수 있다는 것이 밝혀지고 있다. (위암 병리 소견의 이해 김백희, 이성학. 헬리코박터학회지 종설, 2023)
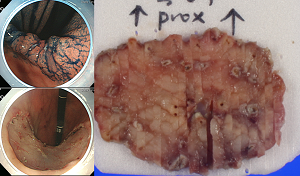
![]() 8. 전벽과 후벽의 방향 표시
8. 전벽과 후벽의 방향 표시
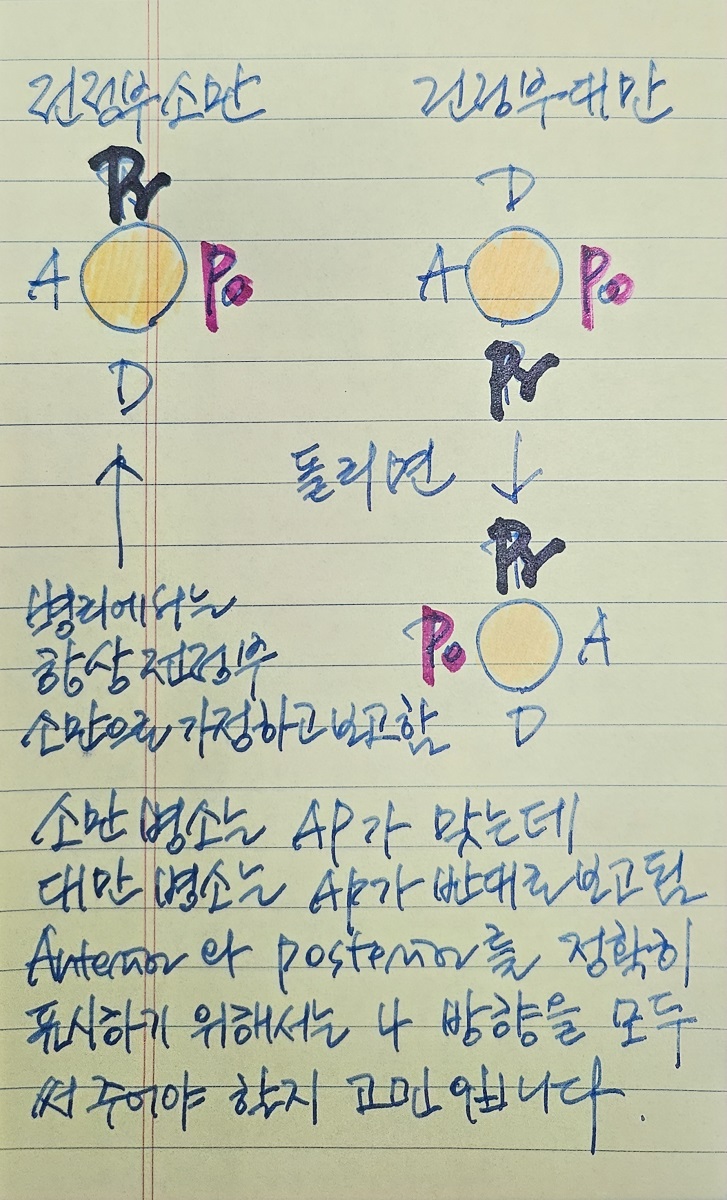
2025년 7월 18일 병리세미나에서 ESD specimen의 방향표시에 대한 검토가 있었습니다. 병리과에서는 proximal의 3시간 전을 전벽으로 표시하고 있습니다. 전정부 소만의 병소에 대해서는 이러한 표시가 적절하지만 전정후 대만의 병소에 대해서는 전벽과 후벽이 반대로 표시되는 오류가 발생하는 방식입니다. 내시경 의사들이 좀 더 정교한 표식을 해 드려야 할지 고민입니다. Resection margin 양성에 대해서 second ESD를 할 경우에는 방향이 매우 중요합니다. Circumferential ablation을 하는 경우라면 그 중요성이 상대적으로 덜합니다.
![]() [Cases]
[Cases]
갈수록 태산이라는 말이 있습니다. 진단 및 치료의 매 단계마다 예상하였던 결과 중 가장 좋지 않은 것으로 나왔고 우여곡절이 있었지만 결국 happy ending으로 마무리된 경우입니다. (EndoTODAY 위암 769)
조직검사에서 용종으로 나왔으나 제거하는 것이 좋겠다는 의견을 듣고 오신 환자입니다. 내시경 재검을 시행하였는데 외부에서 용종으로 나왔던 위각 후벽은 chronic inflammation으로 나왔으나, 위각부에서 약간 융기된 부위가 보이면서 중앙이 발적되어 시행한 조직검사에서 atypical regenerating glnads within erosion background, suggestive of Tubular adenocarcinoma, well differentiated (WHYX type)이 나왔습니다.
左: 외부 첫 내시경. 右: 의뢰 후 재검 (위각 조직검사에서 암 의심)
매우 모호한 상황이었지만 조직검사 결과 의거 ESD를 시행하였습니다. 환자에게는 아래와 같이 설명하였습니다.
외부 조직검사에서 치료가 꼭 필요하지는 않는 과형성 용종으로 나왔으나 모양이 다소 이상하여 치료여부를 상담한 바 있고 재검 후 결정하기로 하였습니다. 과거 조직검사에서 나온 곳은 그냥 염증성인데... 조금 떨어진 곳에서 혹시 암일수도 있다(Atypical regenerating glands within erosion background, suggestive of of TUBULAR ADENOCARCINOMA, WELL DIFFERENTIATED) 는 병이 발견되었습니다. 확진은 아니지만 70% 정도 의심될 때 사용하는 표현입니다.
일단 시술에 필요한 검사를 하고 잠시 입원하여 내시경 절제술을 하여 전체에 대한 최종 병리결과를 확인하는 것이 좋겠습니다. 정말로 암이라면 수술이 필요한 경우가 15% 정도 있기 때문에 더욱 그러합니다.
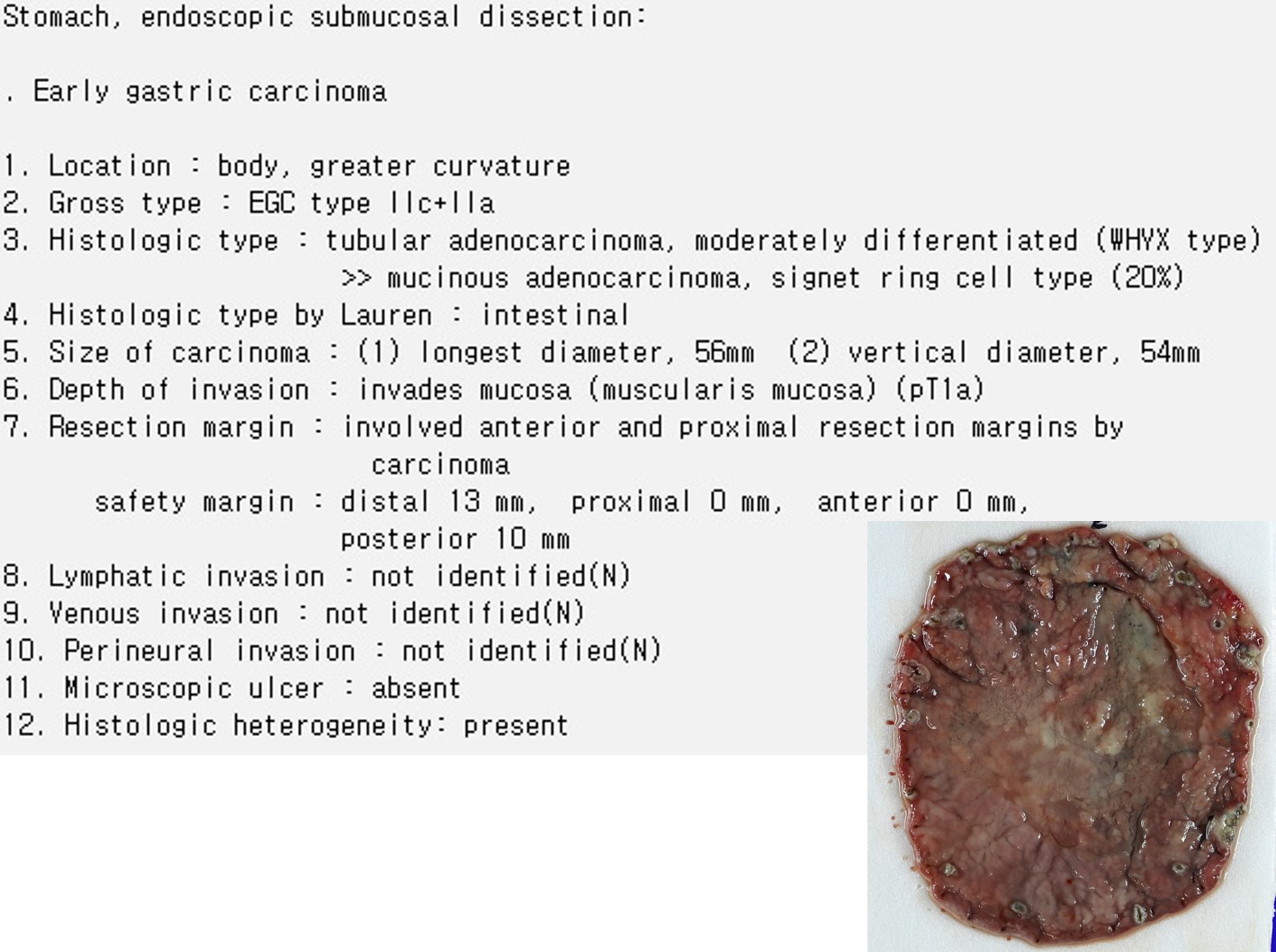
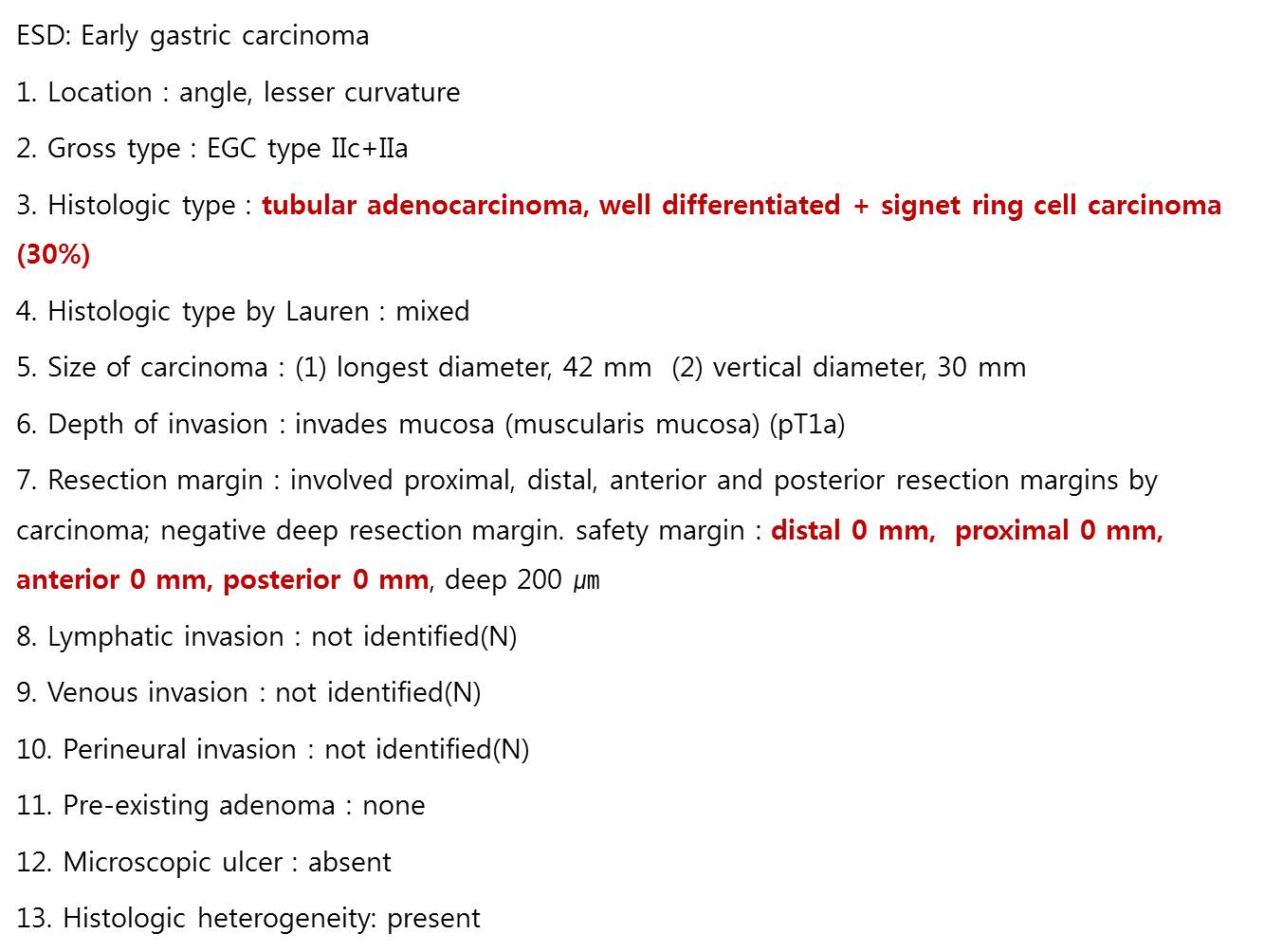
ESD 병리 결과는 아래와 같았습니다. 추정보다 컸고 게다가 all resection margin positive였습니다. Histological heterogeneity는 multiple resection margin positive의 중요한 원인입니다 (EndoTODAY 20121124). 수술을 권하였습니다.
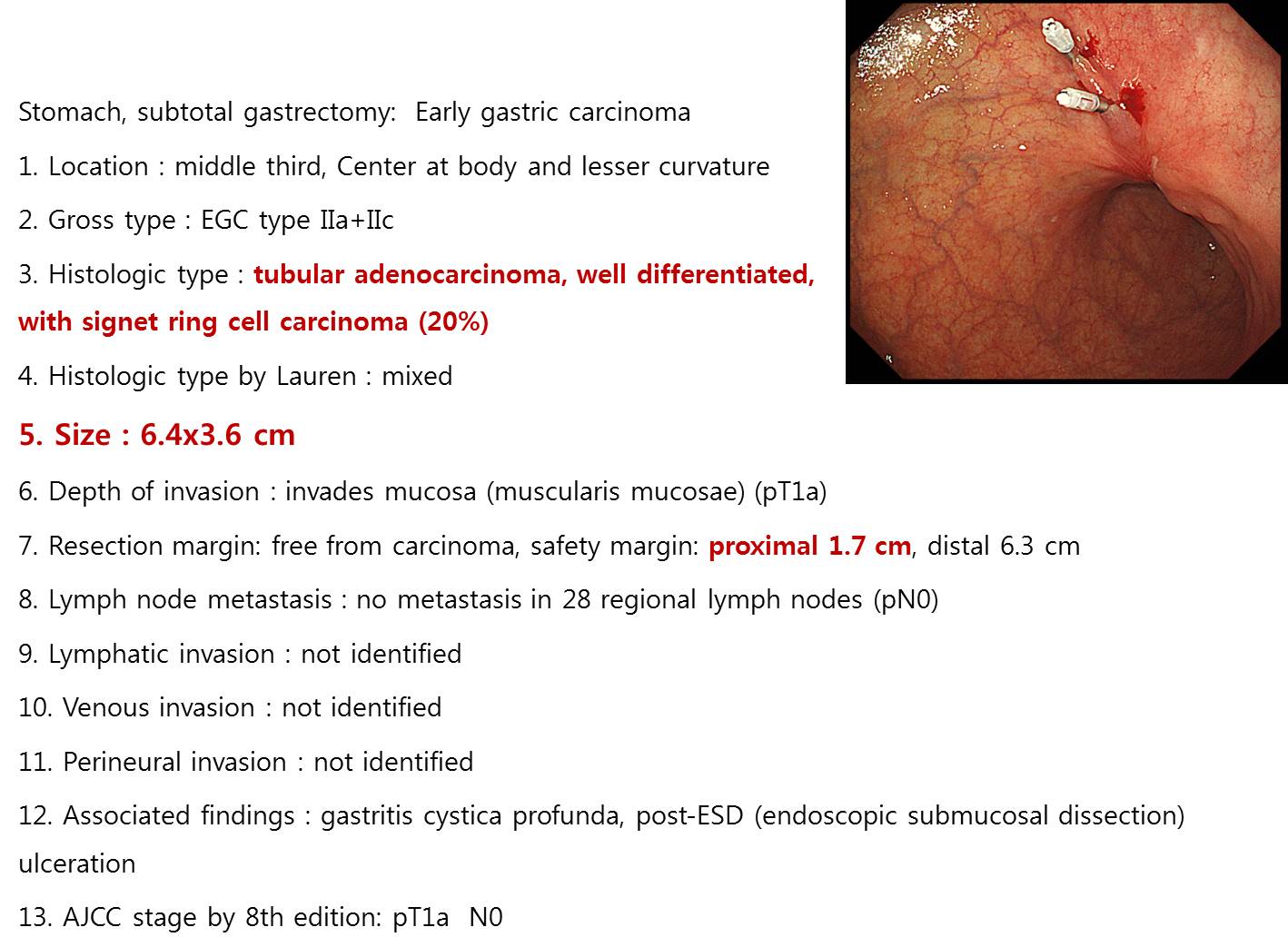
수술 전 clipping을 하였는데 병소의 경계가 명확하지 않았습니다. 수술 후 최종 병리결과는 더욱 놀라웠습니다. Residual tumor가 6.4cm라는 것이었습니다.
우여곡절이 있었지만 결국 제법 크지만 경계가 명확하지 않았던 조기위암이 수술로 잘 치료된 것으로 결론지었습니다.
[more cases]
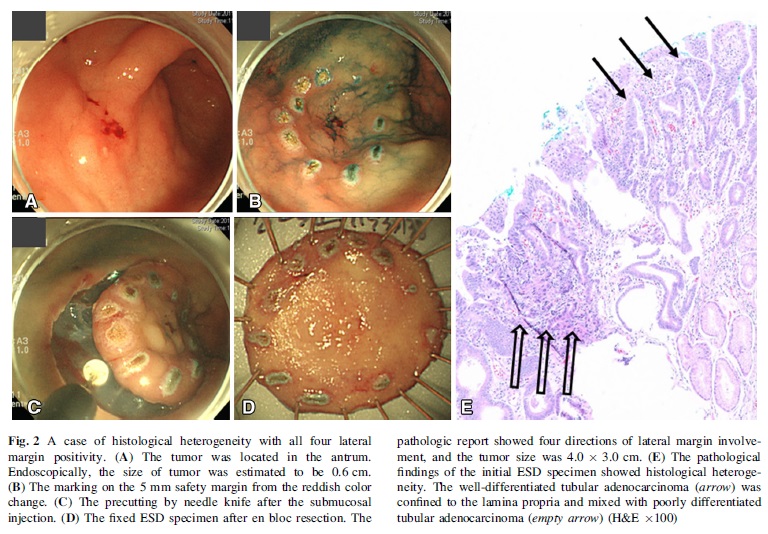
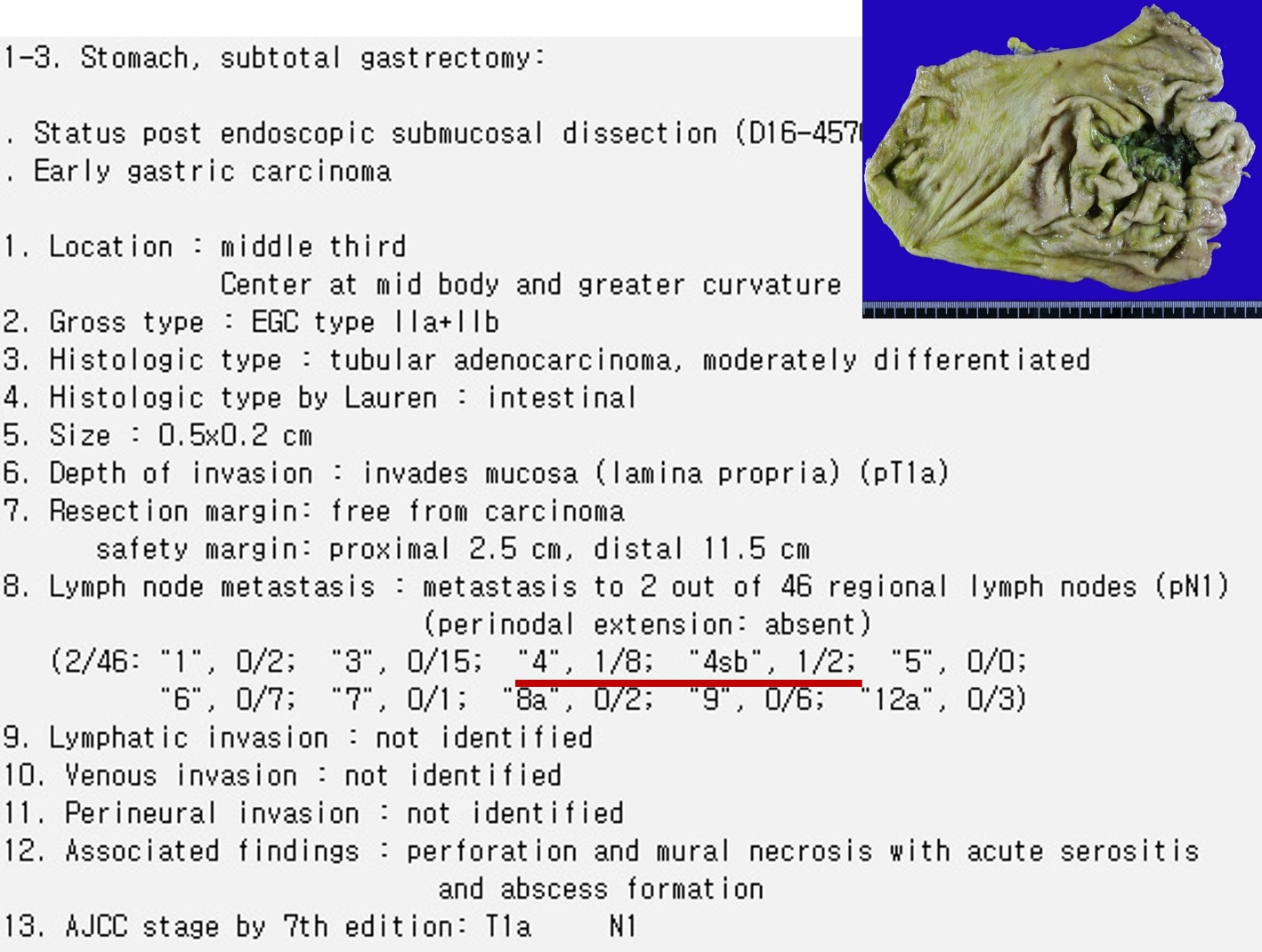
위전정부 소만의 조기위암으로 ESD 시행 후 미분화위암(PD 65% + SRC 35%)이고 lateral margin positive (4곳 중 3곳)로 나와 의뢰된 환자입니다. 첫 조직검사의 결과가 무엇이었는지는 알 수 없었습니다. 수술(subtotal gastrectomy 후 resection margin positive로 total gastrectomy)을 시행하였습니다. 10cm 이상의 점막암(EGC IIb, muscularis mucosae까지 침윤, 첫 수술의 병소 크기는 12cm, 두번째 수술의 병소 크기는 3 cm)이었고 림프절 전이는 없었습니다.
Learning point (1) : 미분화형 위암의 경계판정은 매우 어렵습니다.
Learning point (2): 간혹 10cm가 넘는 조기위암 (점막암)도 있습니다.
2015년 환자. 여자.
[시술 후 외래에서 결과 확인 시 설명한 내용]
내시경 시술 후 최종 병리결과를 확인하기 위한 외래 방문입니다. 비교적 작은 조기위암으로 판단되어 85% 정도의 초기성공률 (내시경치료만으로 일차 치료가 끝나는 비율)을 예측하는 상황에서 내시경치료를 하였는데, 아쉽게도 그 85%에 들지 못하고 수술이 필요한 15%에 해당 하는 결과가 나왔습니다. 내시경으로 절제한 표본에 대한 최종 병리결과에서 세포형, 깊이, 범위, 림프관/혈관에 모두 문제가 없어야 하는데 아쉽게도 문제가 있는 것으로 나왔습니다. 깊지는 않는데 크기가 눈으로 보기보다 커서 절제한 표본의 4방향의 절제여분이 있어야 하는 데 한 방향만 절제 여분이 있고 나머지 방향은 절제변연에 암이 침범되어 있다고 나왔습니다. 즉 수술이 필요한 것으로 나왔습니다. 이런 분들이 약 15%정도 됩니다.
과거에 저희가 이와 같은 경우를 분석한 바 있습니다 (https://www.ncbi.nlm.nih.gov/pubmed/25673346). 사전에 예측하기 어려운 드문 형태의 세포형에서 이처럼 절제변연 양성으로 수술을 권하게 되는 경우가 많았습니다. 환자분도 그에 해당하는 것으로 나왔습니다. WHYX type이라고 합니다. 이 때문에 사전에 병소의 경계가 불분명하였고 절제변연 양성이 나온 것입니다.
병리결과에 문제가 없을 때 재발률이 5% 정도인데 반하여, 현재의 재발 위험은 10-20% 이상입니다. 만약 재발하면 절반 이상은 완치의 기회가 없습니다. 따라서 수술이 경과관찰보다 유리한 상황입니다. 물론 수술은 수술입니다. 전신마취에 따른 위험, 통증, 수술의 합병증, 수술 후 삶의 질 저하 등의 어려운 점이 있지만 그래도 재발위험을 더 많이 고려해야 한다고 판단됩니다. 현재 암이 남아있다는 증거가 있어 수술을 권하는 것은 아닙니다. 단지 재발위험이 높기 때문입니다. 수술을 해보면 눈에 보일 정도의 암이 남아있는 경우는 10-20% 정도입니다. 이러한 내용을 모두 종합하여 판단할 때 수술을 권하고 싶습니다.
외과 의뢰를 하겠습니다. 구체적인 수술 방법은 외과의사와 상의하시기 바랍니다. 일단 내시경 치료한 인공 궤양이 있으므로 당분간 위산분비억제제 복용은 필요합니다. 약은 충분하신지요?
두 달 후로 잡혀있는 내시경 검사는 취소하겠습니다.
계획: 외과 의뢰 (위체부 소만의 경계가 불분명한 조기위암에 대한 ESD를 시행하였으나 세포형이 WHYX이고 resection margin이 3 방향 involvement를 보여 수술적 치료를 위하여 의뢰드립니다.)
The rate of pathological non-curative resection of EGC by ESD is about 10-20%. In additional surgery for non-curative resection cases, local residual tumor is found in 5-10%, and lymph node metastasis is also found in 5-10%. In this case of histological heterogeneity, lateral margin was involved. Surgery was done and 1.2cm x 0.3cm sized residual tumor in lamina propria was found. (EndoTODAY 위암 650)
![]() [FAQ]
[FAQ]
[2015-11-24. 애독자 편지]
언제나 EndoTODAY를 통해 정리해주시고 공부시켜 주셔서 감사합니다~ 저희도 이번 내시경 학회 때 lateral margin만 positive인 non-curative resection 환자들을 review 해서 발표할 예정입니다.^^
Lateral margin만 positive인 경우 re-ESD가 이미 정립된 치료로 학회 등에서 언급되는 경우가 많은데, only lateral margin만 양성인 non-curative resection을 focusing한 solid한 결과가 생각보다 없었습니다. 그래서, 발표 슬라이드에도 'only' lateral margin positive로 only에 빨간색으로 강조하라고 발표자에게 말하였는데, 선생님께서 only 강조를 말씀해주셔서 읽으면서 많이 웃었습니다.^^;;
솔직히 수술이 필요한 경우도 있지 않을까 해서 분석을 해본 것이었습니다. 좀 더 long-term FU data가 필요하기는 하지만, 내시경 치료로 충분한 결과가 나오긴 했습니다 (APC한 한 예에서 distant recurrence가 발생하여 완전한 치료 개념에서 re-ESD가 좀 더 낫지 않을까 조심스럽게 생각해보았습니다)
[2015-11-24. 이준행 답변]
선생님의 발표가 기대됩니다. 꼭 참석하겠습니다.
가장 흥미로운 부분은 APC 후 distant recurrence를 한 환자입니다. 사실 저희 병원에서는 re-ESD 혹은 APC 혹은 observation 후 재발한 환자는 한 명도 없었거든요. 조금 애매하다 싶으면 전부 수술을 보낸 결과 같습니다만.....
발표 슬라이드를 다 만드셨겠지만... APC 후 distant recurrence를 보인 환자의 내시경 사진과 병리사진을 상세히 보여주면 크게 도움이 될 것 같습니다.
![]() [References]
[References]
1) EndoTODAY 위암 425 - 미분화 혼재암 ESD 후 다발성 절제변연 양성 증례
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.