 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [내시경 영어. English for endoscopists] - 終
[내시경 영어. English for endoscopists] - 終
2. 내시경 의사를 위한 영어 표현 (2021, 삼성서울병원 국제진료센터 김지운 교수님)
3. 김지운 교수의 내시경 영어 version 2025
4. 틀리기 쉬운 발음
5. 논문 쓸 때 틀리기 쉬운 표현 - Crisp scientific writing (황윤희)
7. 논문 표현의 숨은 뜻
8. FAQs
9. References
![]() 1. 발표와 토론을 위한 영어 표현
1. 발표와 토론을 위한 영어 표현
[시작]
Thank you for taking time out of your busy schedule to be here today.
I'll start with an overview of my company.
These are the main points I'll cover in my presentation.
I'll start with a little background on the project.
I'd be glad to take questions at the end of my presentation.
If you have any questions, feel free to ask them any time during the presentation.
I'll try to make complex ideas easy to understand.
There will be time for Q and A at the end.
Here is the first story.
[진행]
I'd like to briefly tell you about the current state of the job market.
Now let’s turn to the second issue, security.
That brings me to the second part of my presentation.
This table tells us that our inventory level keeps going up.
Going back to a point I made earlier...
Now you may ask 'What’s wrong with that'.
Now you may wonder why this should be a problem.
Let's consider this in more detail.
Take Google for example.
A good example of this is the success of web-based games.
Another point is that...
This is what I found out.
What I discovered was this is not true.
With that in mind...
Let me briefly explain this report.
Let me talk about the price.
Let me give you an example.
I am pleased to report that
My concern is that
The same thing can happen again.
What we need is something different; we need a different kind of s
This is the picture I want to focus on.
Now let’s take a look at Kakao page.
I was extremely excited about this result.
If you compare this to that, you can see the difference.
[강조]
I'd like to draw your attention to the fact that...
Here, I'd like to point out that there's a lot of room for improving quality.
I'll look at this in more detail later in my talk.
So, what does this mean for our industry?
Let me point out that the technology is not mature yet.
What makes this technology unique is that it is open-source.
What I'm trying to say is that...
I think we should consider buying directly from the producers.
The first point I want to make is that innovation is the key to success.
The second point I want to make is that time is not on our side.
The most important implication of this is that...
I must emphasize that consumers are turning away from junk food.
From an endoscopist's point of view...
If our findings are confirmed, then the implications must be significant.
Our sales are up by 32% but prices are down by 50%.
So, basically this is my point: if you see something impossible, make it possible.
This is the picture I want to focus on.
Now let’s take a look at Kakao page.
I was extremely excited about this result.
If you compare this to that, you can see the difference.
We have to restructure our company, that is to say, we should just focus on our core business.
[마무리]
That brings me to the end of my presentation.
I'll end with some questions for us to discuss.
Before I finish, I’d like to summarize the main points.
I'd like to close by saying one more thing.
It's been an excellent session, I think.
I would like to mention some of the principal points that have emerged from the presentations and discussions.
Let me just review what we've seen today.
I'd like to finish my presentation by showing this slide (또는 with a story).
Consider this; according to a recent survey...
[질의 응답]
I'm sorry I didn’t catch your question.
I really appreciate your input.
I take your point.
You are quite right on that point.
I'm afraid that’s outside the scope of this presentation.
Let me deal with the last question first. If I understood correctly, your question was about...
I'll come back to that question later in my presentation.
I'll have to check on that and get back to you.
I am not in a position to say anything on that.
I hope that answers your question.
I have a slightly different point of view.
Looking behind the statistics, wee see that most children are first introduced to computers in their homes and at school through games.
Apart from the weight, I really like your new product.
[인용]
Steve Jobs (1997): Apple is executing wonderfully on many of the wrong things. I've met some extraordinary people at Apple. There are a lot of great people at Apple. They are doing some of the wrong things because the plan has been wrong.
![]() 2. Practical English for endoscopists 내시경 의사를 위한 영어 표현
2. Practical English for endoscopists 내시경 의사를 위한 영어 표현
2021년 7월 20일 이노엔 Talkshow에서 김지운 선생님께서 내시경실 영어를 동영상과 함께 소개하셨습니다 (Subnote PDF).
1) EGD
2) Colonoscopy

3) Trouble : difficult secal intubation - holding breath and counterpressure technique
4) Trouble : Changing to supine position

5) Withdrawal

6) Polypectomy

7) 내시경 결과 영어로 설명하기
(1) Heartburn
Hey, Mr. Lee, how did you do after the endoscopy? Were you okay? Let me show your pictures from the endoscopy and explain. Hey, you have some damage from your reflux here. This is probably the cause of your having a heartburn, so we need to correct this.
There are two ways to treat this. One by medication, and one by your lifestyle changes.
We have this new acid blocker called K-cab which is available here but not yet in US. That works very well. It suppresses the acid much better than the existing ones.
And you also need to do the lifestyle modifications. Make sure you don’t lay down 2~3 hours after you eat.
Make sure you don’t overeat. Avoid your late night snacks. You also need to lose some weight.
(2). Colon polyps
김지운 교수: Okay, Mr. Lee. How did you do after the colonoscopy? Were you able to pass all the gas? Let me show you some pictures from the colonoscopy. Like I told you before, after the procedure, we found two polyps. And then we removed them completely. So you don’t have to worry about it. We sent it to the pathology, and they gave us the result of what we call tubular adenoma. These are pre-cancerous polyps. I want to emphasize that this is not cancer. This is pre-cancerous. This is something that can turn into cancer if you left it. But in any case, we removed it completely. So don’t worry.
The one on the left is sized about 1.5 cm, and one on the right is very tiny. It’s about 3~4 mm. Because you’ve got two polyps, your next colonoscopy is going to be in 3 years.
이준행 교수: Next colonoscopy in 3 years?
김지운 교수: Correct.
이준행 교수: You mean every 3 years lifelong? Or just for 3 years and that’s it?
김지운 교수: It depends on what the next colonoscopy will show. It will depend on the size of the polyp, the number of the polyp and the type of the polyp it is. And also it will depend on the cleanness of your bowel prep. Your cleansing.
이준행 교수: Okay.
김지운 교수: There are few things you can do to lessen the chance of growing polyps that can grow into cancer. Make sure you cut down your meat consumption. Make sure you exercise, lose weight, stay active. Eat a lot of food with fiber content. Fresh fruits and vegetables are always good. These are some other things that you can do for yourself to reduce the risk.
이준행 교수: So the most difficult part is the weight reduction. Is it a must? How much weight should I lose?
김지운 교수: It all depends on how committed you are in keeping your health. If you want to live long in a health manner, exercise is going to be a key component. I think it’s going to be a must.
이준행 교수: Hmm, must. Okay. So, what about drinking some alcohol? Just a little is OK?
김지운 교수: I believe in moderation in everything. So binge drinking and heavy drinking is not good for your health. Not just for your colon health, but also for your liver and other parts of your body. So I recommend conscientious and moderate drinking.
이준행 교수: Okay, moderate drinking. How much is the moderate drinking?
김지운 교수: I’ll say 1~2 drinks 1~2 times per week.
이준행 교수: Twice a week is moderate, Hmm.
김지운 교수: One glass of beer, not one glass of soju.
이준행 교수: One glass of beer. I see.
8) .Key Points in Patient Education About the Brain?Gut Axis, in Lay Language (Gastroenterology 2018;154:1249?1257)
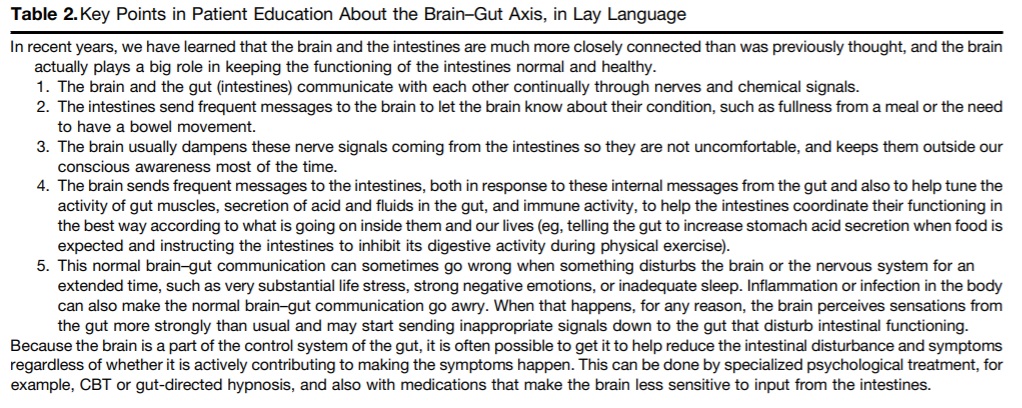
In recent years, we have learned that the brain and the intestines are much more closely connected than was previously thought, and the brain actually plays a big role in keeping the functioning of the intestines normal and healthy.
1. The brain and the gut (intestines) communicate with each other continually through nerves and chemical signals.
2. The intestines send frequent messages to the brain to let the brain know about their condition, such as fullness from a meal or the need to have a bowel movement.
3. The brain usually dampens these nerve signals coming from the intestines so they are not uncomfortable, and keeps them outside our conscious awareness most of the time.
4. The brain sends frequent messages to the intestines, both in response to these internal messages from the gut and also to help tune the activity of gut muscles, secretion of acid and fluids in the gut, and immune activity, to help the intestines coordinate their functioning in the best way according to what is going on inside them and our lives (eg, telling the gut to increase stomach acid secretion when food is expected and instructing the intestines to inhibit its digestive activity during physical exercise).
5. This normal brain?gut communication can sometimes go wrong when something disturbs the brain or the nervous system for an extended time, such as very substantial life stress, strong negative emotions, or inadequate sleep. Inflammation or infection in the body can also make the normal brain?gut communication go awry. When that happens, for any reason, the brain perceives sensations from the gut more strongly than usual and may start sending inappropriate signals down to the gut that disturb intestinal functioning.
Because the brain is a part of the control system of the gut, it is often possible to get it to help reduce the intestinal disturbance and symptoms regardless of whether it is actively contributing to making the symptoms happen. This can be done by specialized psychological treatment, for example, CBT or gut-directed hypnosis, and also with medications that make the brain less sensitive to input from the intestines.
* 참고: practical_english_endoscopist.txt (2018, 김지운 선생님)
![]() 3. 김지운 교수의 내시경 영어 version 2025
3. 김지운 교수의 내시경 영어 version 2025
1. 설명(상담)
2. 검사 대기실 입실
3. 검사실
4. 회복실
![]() 4. 틀리기 쉬운 발음
4. 틀리기 쉬운 발음
'에데마'가 아닙니다.
'에로우전'이 아닙니다.
'레전'이 아닙니다.
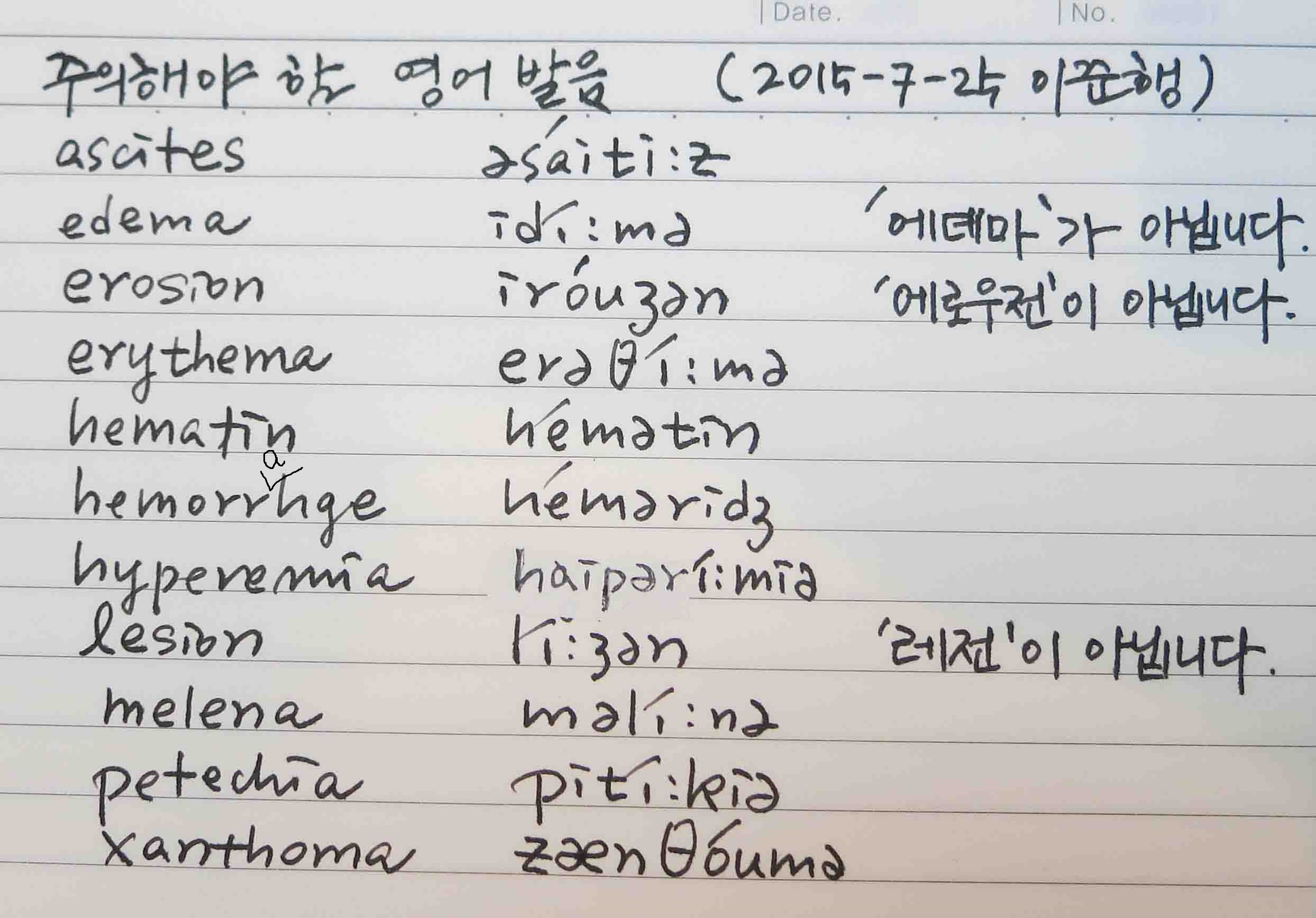
기타 틀리기 쉬운 발음
![]() 5. 논문 쓸 때 틀리기 쉬운 표현
5. 논문 쓸 때 틀리기 쉬운 표현
Crisp scientific writing (컴팩스 황윤희)
결과에는 과거 시제를 쓰고, 표와 그림에는 현재 시제를 쓴다.
P=0.01 ⇒ P = 0.05
(Fig.1) ⇒ (Fig. 1)
(Table 1.) ⇒ (Table 1)
Five patients who underwent ESD for EGC ⇒ Five patients who received ESD for EGC
Six patients were re-grouped as posttreatment BAI-EGCs.
Additional surgery rate was ⇒ The rate of additional surgery was
The proportion of EGC in the entire gastric cancer is increading due to the technical development and the introduction of mass screening program. ⇒ The proportion of EGC among all gastric cancers in increasing due to technical advances...
In the real clincal practice ⇒ In real clincal practice (the 없음)
absolute indications of ESD ⇒ absolute indications for ESD
We grouped the cases twice to analyze the grouping discrepancy before and after the treatment. ⇒ We grouped the cases before and after treatment to analyze grouping discrepancies.
The most common reason of this discrepancy ⇒ the most common reason for this discrepancy
On the contray ⇒ In contrast
the change in ⇒ changes in
Table 4 shows comparison between A and B ⇒ Table 4 compares A and B
necessity of additional treatment ⇒ necessity for additional treatment
There is a controvery about ⇒ Controvery remains about
Literatures on expanded indications are heterogeneous ⇒ The literature on expanded indications is heterogeneous.
There are some limitations in the present study. ⇒ There are some limitations to the present study.
Possible - it could happen < 50%; probable - it could happen > 50%
M.D. ⇒ MD; e.g., ⇒ eg; April 16th ⇒ Apr. 16 ⇒ Apr 16
P=0.05 ⇒ P = 0.05
(Fig.1) ⇒ (Fig. 1)
Brown et al(1987) ⇒ Brown et al (1987)
4 times more ⇒ 4 fold greater
and and and and ⇒ subsequently, followed by, leading to, resulting in, consequently, finally...
![]() 6. 홍성태 저 '의학논문 매력 있게 쓰자'
6. 홍성태 저 '의학논문 매력 있게 쓰자'
2014년 8월 23일 대한의학학술지편집인협의회의 제 3회 논문작성 워크숍에서 'Table, figure 및 결과작성요령'에 대한 강의를 하였습니다. 이 자리에서 홍성태 교수님께서 쓰신 '의학논문 매력 있게 쓰자'라는 책을 받았습니다. 일부를 옮깁니다.

(104쪽) 5) 동사의 활용 - 영어는 동사 단어에 어미를 붙여서 파생한 명사가 많다. 이러한 파생명사보다는 가급적 원래 의미의 동사를 사용하는 것이 낫다.
X - Foreign body removal was carried out using a cystoscope.
O - The foreign body was removed using a cystoscope.
X - Measurement of its diameter was done using an ocular micrometer.
O - Its diameter was measured using an ocular micrometer.
(105쪽) 6) 능동태와 수동태 - 영문 원저논문에서 수동채 문장이 많이 등장한다. 가급적 능동형 문장으로 작성하는 것이 좋지만 주어가 마땅치 않거나 주어부 단어가 너무 길면 수동태로 작성하는 것이 낫다. 우리가 흔히 하는 실수가 자동사를 수동형 문장에 사용하는 것이다. 그리고 타동사 중에서도 수동형으로 사용하지 않는 것이 있는가 하면 항상 수동형으로 사용하는 단어도 있다. 자동사와 타동사 용법이 모두 있어 쓰임에 따라 의미가 달라지는 동사도 있으므로 유의해야 한다.
X - A part of the tumor mass was remained after the surgery. 자동사인데 수동형으로 잘못 사용
O - A part of the tumor mass remained after the surgery.
X - A hazardous chemical is contained by the flask. 항상 능동형 문장으로 작성하는 동사를 수동형으로 잘못 사용.
O - The flask contains a hazardous chemical.
(112쪽) 11) 콜론과 세미콜론 - 콜론(:)은 문장을 이해하기 쉽게 예를 들어 설명하는 경우 접속사 대신 흔하게 사용한다. 콜론을 찍으면 일단 그 문장은 그 자리에서 끝나고 그 뒤는 단어를 나열하거나 완전하지 않은 문장인 구로 정리된다. 세미콜론(;)은 쉼포(,)와 구분하는 큰 쉼포로 사용한다.
예 - The findings of body weight 5 weeks after the experiment by groups were as follows: control, 57 g; test group 1, 117 g; test group 2 131 g.
(127쪽) 전문가 심사
Article: PARINT-D-11-0000
General Comment: This manuscipt is an original article that studied serum IgG reaction to ...
Overall quality of writing scientific manuscript requires professional language editing. There are grammatical mistakes in the text.
Specific Comments:
(146쪽) 실제로 저자됨 위반(authorship abuse)이 발생하기도 한다. 명예저자(공짜저자, gift author, honorary author)는 전혀 연구나 논문작성에 기여함이 없이 공저자로 무임승차하는 경우를 말한다. 공동연구를 특징으로 하는 의학분야에서 아주 흔한 유형으로, 윗사람을 모시거나 영향력이 큰 사람을 정치적인 목적으로 공저자로 영입하는 행위도 실제로 발생한다. 유령저자(ghost author)는 연구에 실제로 열심히 참여하여 저자로 의당 참여할 사람이 저자에서 배제되는 경우를 말한다. 명예저자가 저자됨에서 부당한 참여라면 유령저자는 부당한 배제에 해당한다. 유령저자 유형은 실제로 많이 발생하지는 않지만 그 여파가 훨씬 심각할 수 있어 이러한 일이 생기지 않도록 주의해야 한다. 국내에서 유령저자 사건으로 인해 연구책임자가 형사처벌을 받은 사례가 있다. 그 외 잘 아는 연구자끼리 서로 저자됨을 교환하는 교환저자(swap author), 유명한 사람을 일방적으로 끼워넣는 도용저자(theft author) 등 다양한 유형의 저자됨 위반유형이 있다.
![]() 7. 어떤 사람이 논문 표현의 숨은 뜻을 설명하는 흥미로운 자료를 보았습니다. 일부를 소개합니다.
7. 어떤 사람이 논문 표현의 숨은 뜻을 설명하는 흥미로운 자료를 보았습니다. 일부를 소개합니다.
It has long been known... 원전을 찾아보지 않았다.
While it has not been possible to provide definite answers to the questions... 실험은 실패했지만 그래도 논문을 내야겠다.
Three of the samples were chosen for detailed study... 나머지 샘플은 해석 불가능했다.
These results will be in a subsequent report... 연구비 제대로 받으면 언젠가 쓸 생각이다.
It is believed that ... 나는 그렇게 생각한다.
It is generally believed that ... 나 말고도 몇 명 더 그렇게 생각한다.
Correct within an order of magnitude ... 틀렸다.
A statistically oriented projection of the significance of these findings ... 적당히 때려 맞춰보면
A careful analysis of obtainable data... 맥주를 엎지르는 바람에 데이터를 적는 노트 3장을 날려먹었다.
It is hoped that this study will stimulate further investigation in this field... 저는 그만 둘래요.
In my experience ... 한 번
In case after case... 두 번
In a series of cases ... 세 번
![]() [FAQs]
[FAQs]
[2021-9-9. 이준행 질문]
Impression 혹은 진단명을 쓸 때 compatible, consistent, probably 등등의 용어에 있어서 어느 것이 더 강력한지 ... 대강 몇 % 정도 의심될 때 사용하는 것인지 기준이나 가이드라인 같은 것이 있는지 궁금합니다.
[2021-9-9. 김지운 교수님 답변]
교수님,
진단적 확신의 강도는 세 단어를 보았을때 대중적인 기준이나 가이드라인은 없고 개인차가 있을 것 같습니다.
굳이 따지자면 제 기준은 Consistent > Compatible 이라고 생각되며 두개의 단어 모두 "80-90%" 이상의 확신이 있으면 쓸거 같고 Probable/probably 는 50% 이상의 상황에서 쓸 것 같습니다. 50% 미만의 상황에서는 possible/possibly 를 쓸 것 같습니다.
These endoscopic findings are consistent with (indicative of) early gastric cancer. (Endocopic findings have all the components of typical findings.)
These endoscopic findngs are compatible with early gastric cancer. (Endoscopic findings have almost all the components of typical findings.)
These endoscopic findings are probably those of a benign gastric ulcer. 약간 awkward 합니다. (Endoscopic findings have many typical findings (or most important finding), but really need histopathology results.)
Early gastric cancer is a possibility with these endoscopic findings.
도움 되셨으면 좋겠습니다.
[2024-11-2] JDDW. 미국에서 일하는 일본인 교수의 강의 중
위 강의에서 미국인들과 소통이 잘 안 되는, 즉 발음이 어려운 단어로 amylase, hematemesis, diverticulum, hematochezia가 제시되었습니다. 일본식으로 발음하면 미국 사람들이 절대로 알아듣지 못한다고 합니다. 우리나라 방식으로 발음하면 전달이 잘 되는 것들이었습니다. 일본인이 어려워하는 발음과 우리에게 어려운 발음은 조금 다릅니다. 여하튼 naver에서 발음을 찾아 3번씩 반복해서 연습하였습니다. 혹시나 내 발음을 미국인들이 알아듯지 못하면 곤란하니까.
![]() [References]
[References]
2) practical_english_endoscopist.txt (2018, 삼성서울병원 국제진료센터 김지운 교수님)
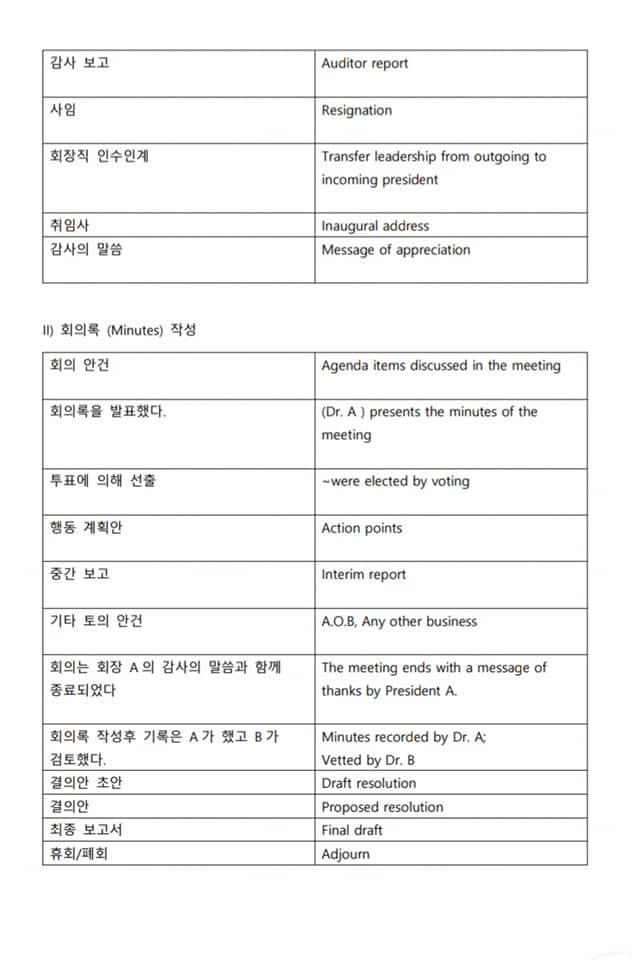
3) 박효진 교수님께서 Facebook에 올린 회의 영어
4) 내시경실 영어 동영상 (2021, collaboration with Inno. N): 위내시경, 대장내시경, Touble 1, Touble 2, Withdrawal, Polypectomy
5) PET 판독에서 사용하는 표현: consistent with: >90%, probable/probably: 75-90%, possible/possibly: 50-75%, equivocal: 50%, unlikely: <25%
6) 부서 명칭 영문화 version 1 (2025) PDF
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng