EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [고령 위암. Gastric cancer in the elderly] - 終
[고령 위암. Gastric cancer in the elderly] - 終
1. 고령 위암 역학
4. 고령 환자에서 screening endoscopy가 필요한가?
5. References
![]() 1. 고령 위암 역학
1. 고령 위암 역학
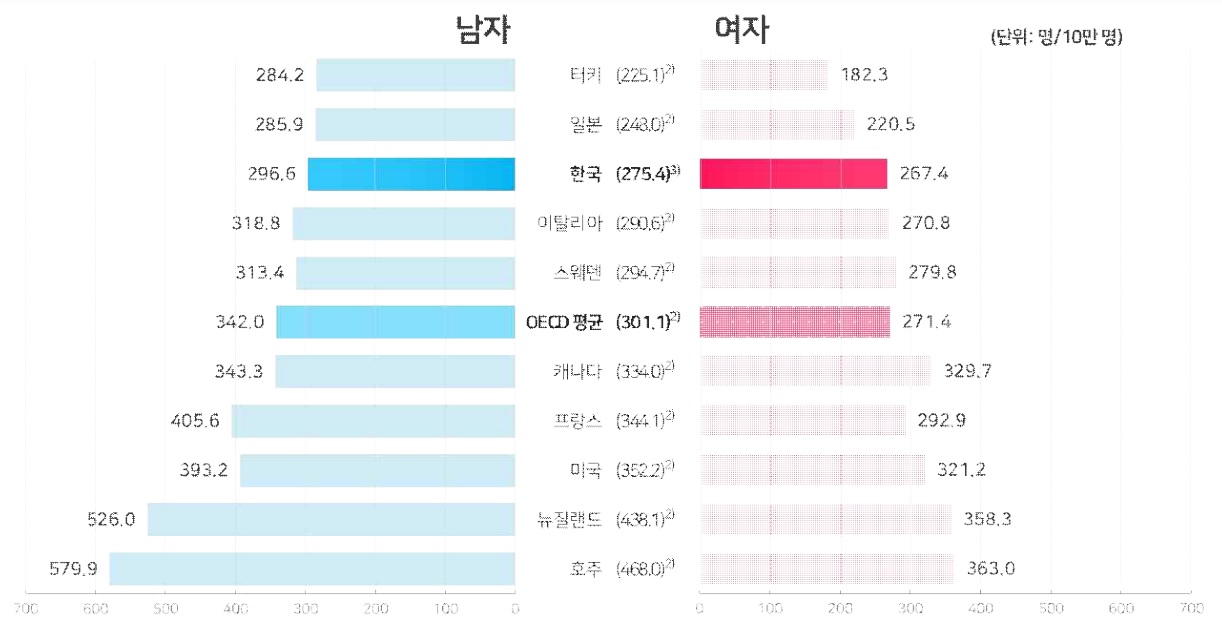
우리 나라에서는 건진과 과잉진단이 일상화되어 있으므로 무증상에서 발견되는 암이 많으므로 다른 나라에 비하여 암환자가 많을 것으로 생각하기 쉽습니다. 그러나 2019년 국가암등록통계에 따르면 세계표준인구로 보정한 우리나라 암발생률은 인구 10만 명당 275.4명으로 OECD 평균(301.1명)보다 낮은 수준이었습니다.
위암의 연령표준화발생률은 지난 8년간 4.5%정도 감소하였습니다. 5년 생존율도 꾸준히 좋아지고 있습니다. 그 결과 위암이라는 진단을 가지고 생존해 계시는 위암 유방률이 꾸준히 증가하고 있습니다. (2019년 국가암등록통계)
연령표준화 발생률
5년 생존율
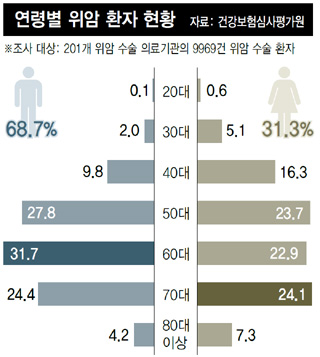
위암의 연령별 발생률을 살피면 고령에서 꾸준히 발생률이 증가합니다. 남성에서는 80대 초반이 가장 높고 여성은 좀 더 고령까지 계속 높아집니다. (2019년 국가암등록통계) 수술 환자 중 80대 이상의 비율은 약 5%입니다.
남성
여성
![]() 2. 고령 환자의 위암 수술은 안전한가?
2. 고령 환자의 위암 수술은 안전한가?
고령 환자의 위암 수술과 상대적으로 젊은 환자의 위암 수술의 성적과 합병증에 차이가 있는지 늘 궁금합니다. 과거에는 나이에 따른 차이가 없다는 연구 결과가 많았습니다. 그 중 하나를 소개합니다.
Literatures about the surgical experience are always excellent. This report from Kangbuk Samsung Hospital can be a good example. Authors divided the elderly patients into two groups - younger elderlies, who are less than 75 years old, and very elderlies, who are more than 75 years old. As you can guess, the very elderly patients have underlying diseases more often. However, the rate of curative resection is also very good in the very elderly patients - more than 90 percent.
Regarding surgery for very elderly patients, there is a concern about postoperative morbidity and mortality. However, in this series, the rate of postoperative complication and one-month mortality was not different between the two age groups.
The overall survival was slightly better in the young elderly patients, but it may be related with more advanced stages in the very elderly patients.
Actually, the overall survival for stage I, II, and IIIa did not differ significantly between the two age groups.
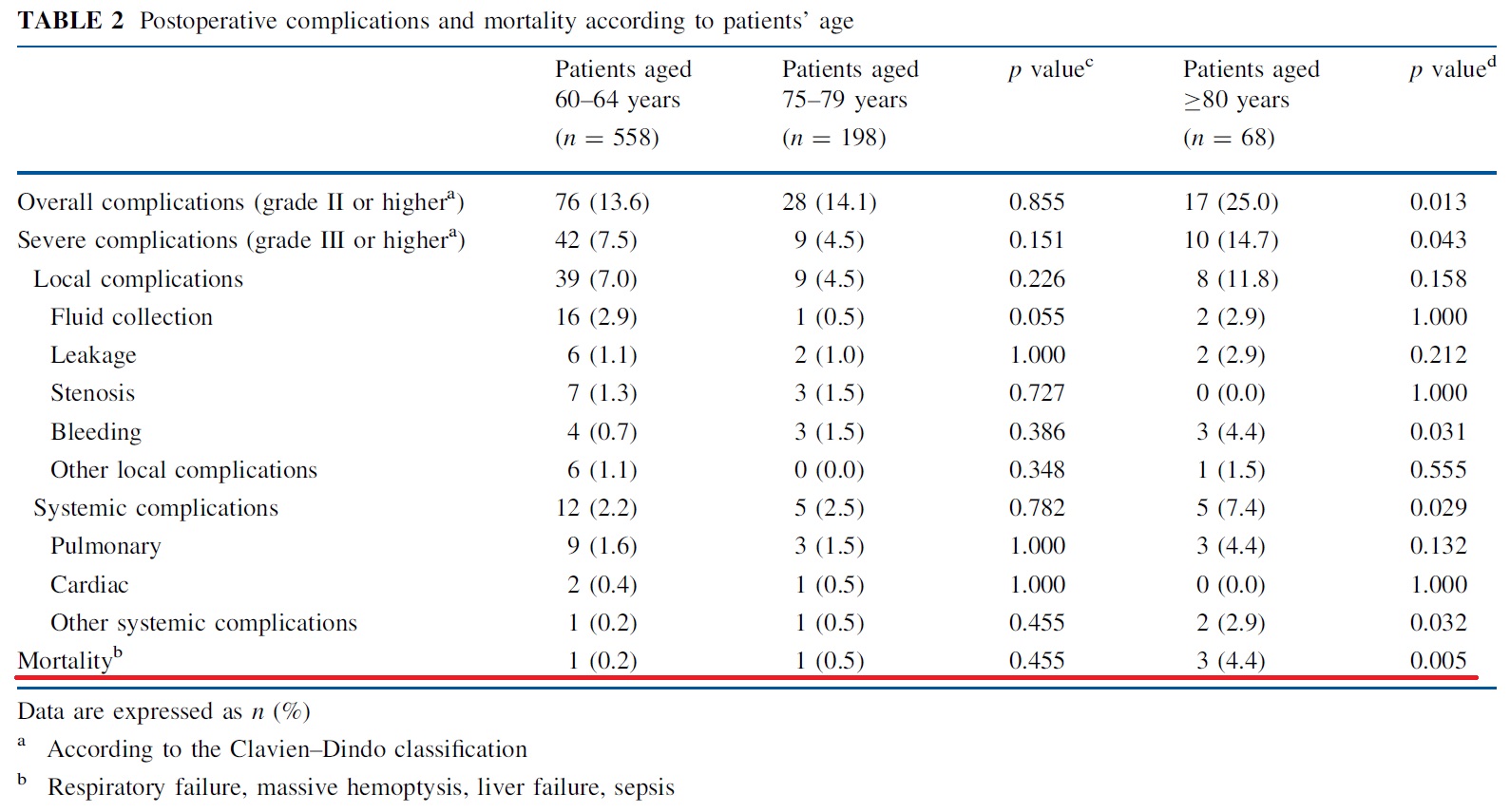
그러나 실제로 주변을 둘러보면 나이가 많을수록 위암 수술의 합병증도 많고 사망률도 높은 것 같습니다. 한 대형병원의 최근 보고(Ann Surg Oncol 2017)에 의하면, 상대적으로 젊은 환자에 비하여 초고령 환자의 위암 수술 사망률이 높다고 합니다. 80세가 넘으면 위암 수술 사망률이 4.4%였습니다. 물론 통계적으로 유의한 차이였습니다. 저는 이와 같은 솔직한 논문이 좋습니다. 임상 경험과 잘 맞으니까...
![]() 3. 고령 환자의 위암은 천천히 자라는가?
3. 고령 환자의 위암은 천천히 자라는가?
과거에는 고령 환자의 위암은 천천히 자라는 경우가 많다고 알려졌습니다.
This is a rare example of early gastric cancer without significant interval change for a long time.
그러나 최근에는 상대적으로 젊은 환자의 위암과 고령 환자의 위암의 성장 속도에 차이가 없다는 것이 정설입니다.
![]() 4. 고령 환자에서 screening endoscopy가 필요한가?
4. 고령 환자에서 screening endoscopy가 필요한가?
There are two important biases in the cancer screening. The first one is very famous, the lead time bias. I think all individuals in this hall already understand this type of bias. Even if we may detect cancers earlier, the overall survival gain is another issue due to the lead time bias.
The second bias is the length-time bias. It means cancers detected in the screening program may be less aggressive. This bias is especially important for the elderly population. If some cancers in the elderly people are very slow-growing, is there any reason that we need to find them?
Survival gain by the cancer screening is usually like this. At some age, the survival gain can be zero. After that point, screening can actually decrease the individual’s survival. We need to stop before that age. But, the problem here is that we don’t know exactly when to stop.
In terms of screening for cancers, we need to consider the life expectancy. Screening tests are usually recommended when the expected survival is longer than 10 years. In this regard, screening at the age of 80 is usually not recommended.
Do you know the Hoerr’s law? It means it is difficult to make the asymptomatic patient feel better. Regarding the screening in the elderly population, we need to ask to ourselves. We are really making the elderly people feel better, be happier by all the screening and aggressive treatment?
A few years ago, US preventive services task force recommended against routine colonoscopy for adults with ages 76 to 85.
This is one of many evidences supporting the US preventive services task force recommendations. After 75 years, screening colonoscopy showed no more benefit. Actually, screening colonoscopy after 75 years makes more and more complications. 75 is a good age for stopping screening colonoscopy.
As a box summary, I can say that more is not always better, especially in the cancer screening in the elderly. Sometimes, less may be better. We need to stop at some point.
보다 상세한 논의는 EndoTODAY 건진 위내시경을 몇 세에 중단할 것인가?를 참고하시기 바랍니다.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.