 EndoTODAY ���ð� ����
EndoTODAY ���ð� ����
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Achalasia & POEM. �ĵ��̿ϺҴ���] - ��
[Achalasia & POEM. �ĵ��̿ϺҴ���] - ��
2024�� 8�� 18�� KSGE ���ð� ���̳� �赵�� ������ ���� log-in �
1. Symptoms - (1) GERD�� ���ε� �� �ֽ��ϴ�. (2) High index of suspicion�� �ʿ��մϴ�.
2. Endoscopic diagnosis of achalasia
3. Manometric and other diagnostic tools of achalasia
7. Cases
8. FAQs
9. References
![]() 1. Achalasia �� ���� - (1) GERD�� ���ε� �� �ֽ��ϴ�. (2) High index of suspicion�� �ʿ��մϴ�.
1. Achalasia �� ���� - (1) GERD�� ���ε� �� �ֽ��ϴ�. (2) High index of suspicion�� �ʿ��մϴ�.
���ڸ����� ū ����� �� �մϴ�. 2014�� 12�� 5�� ���ѻ��������︮�ڹ��� �߰��м���ȸ �� ����Ļ縦 �ϸ鼭 �� ������ �̷� ���� �̾߱⸦ ���������ϴ�. ���� �����⸦ ���Ͽ� �ణ�� ���� ���� �� ��������. �����Բ����� �ֱٿ� ������ �������� ���ʸ� �Ұ��� �ּ̽��ϴ�.
�������� "achalasia�� GERD�� ���ε� �� �ִ�"�� ���� �����ϼ̽��ϴ�. �� �������� ���� �Ⱓ refractory GERD�� �������� �ſ� ���� �˻�� ��Ⱓ�� ġ�Ḧ ������ ȣ���� ������ ȯ�ڿ����ϴ�. �쿬�� esophagography�� ����µ� �������� bird beak�� achalasia �Ұ��� �߰ߵǾ����ϴ�. ȯ�ڴ� dysphagia�� ȣ������ �ʾҴµ��� esophagography�� �������� achalasia �Ұ��̾����ϴ�. POEM(peroral endoscopic myotomy)���� ġ���Ͽ��� refractory GERD�� ���εǾ��� ������ �Ϻ��� ���������ϴ�. ���� dysphagia�� ȣ������ �ʾҴ� ȯ�ڰ� POEM�� �ް� �� �� �ڽ��� ���� ������ dysphagia������ �ڴʰ� ���Ҵٰ� �մϴ�.^^ "��~~~ ������ �̷��� ���� �Ѿ ���� �ֱ���..."
�����ǵ��� ���� ���� UpToDate�� �̷� ����� �ֽ��ϴ�.
Patients with achalasia may develop heartburn as a result of fermentation of retained food in the esophagus. (��ũ)
Achalasia has an insidious onset and disease progression is gradual. Patients typically experience symptoms for years prior to seeking medical attention. In one series of 87 consecutive patients with newly diagnosed achalasia, the mean duration of symptoms was 4.7 years prior to the diagnosis. The delay in diagnosis was mainly due to misinterpretation of typical clinical features rather than atypical findings. Many patients are treated for other disorders such as gastroesophageal reflux disease before the diagnosis of achalasia is made. (��ũ)
�ణ ������ ���������� Gut���� �Ǹ� Scotland �ڷῡ���� achalasia ȯ�ڰ� ��Ⱓ GERD�� ���εǾ� ġ��� ��찡 ���ٴ� ���� ���ɴϴ� (Howard 1992)
With the increasing availability of manometry, patients with achalasia are often referred at an early stage when they lack the classic features of established disease. A prospective five year study of the presenting features of untreated achalasia referred to our department was undertaken. Twenty men and 18 women presented throughout adult life, with a mean age at the time of diagnosis of 44 years (range 17 to 76 years). The presenting symptoms were dysphagia: for solids (100%) and for liquids (97%), chest pain (74%), and weight loss (60%). Endoscopy was reported as normal in 15 patients and achalasia was suggested in only 21 of 33 barium examinations. Fourteen had been treated for gastrooesophageal reflux but none had been misdiagnosed as having cardiac or psychiatric disease. The annual incidence of achalasia in the Lothian region is 0.8/100,000 of population. Persistent dysphagia is the cardinal symptom of achalasia which presents throughout adult life. Nevertheless, recent onset achalasia is often misdiagnosed as gastrooesophageal reflux disease. Because endoscopy is frequently normal and the diagnosis is often not made by radiology, manometric investigation is necessary if the condition is to be recognised and treated at an early stage.
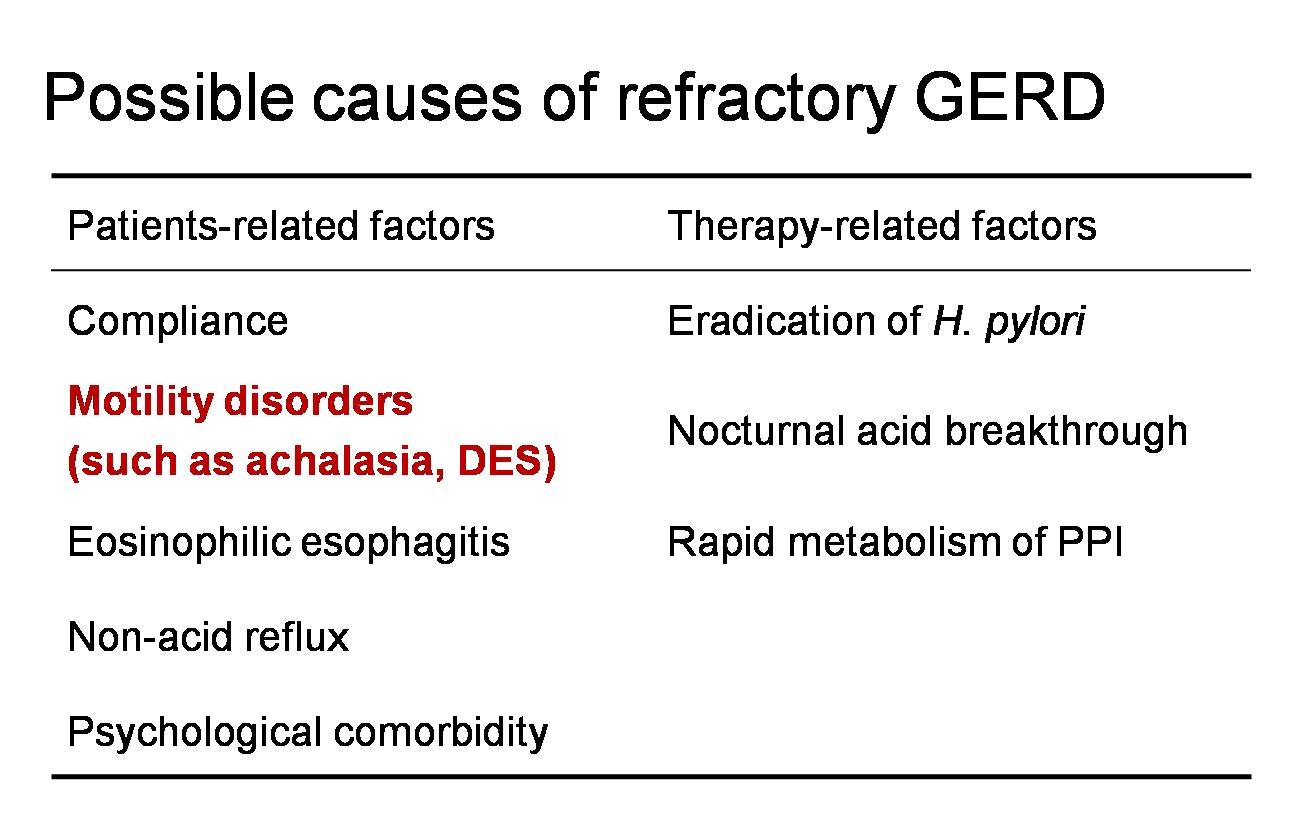
���� refractory GERD�� ���� ���ǿ��� ���� ����ϴ� ǥ�Դϴ�. Motility disease�� �߿��ϰ� ����ϰ� �ֽ��ϴ�. Ư�� achalasia�� refractory GERD�� �������ܿ� ���ٴ� ���� �߿��մϴ�. GERD�� ���� ������ achalasia�� ���� ������ ���� �ٸ��ϴ�. Achalasia�� ��� ȯ�� �����δ� �� �Ծ��ٰ� ���������� �þ �ĵ��� ������ ��ü�� �����Դϴ�. ȯ�ڰ� �㿡 ����� ���� ���� �� ���� ������ ������ ���մϴ�. ���� ���� achalasia�� ���������.
�������� achalasia�� POEM ġ�Ḧ ���� ���� ȯ���Դϴ�. ���� ���ŷ��� ���� ������ �ĵ������� ���ܹް� ġ����� ������ �־����ϴ�. ���� ȿ���� ����������.
Achalasia�� ���ܿ��� ���� ����� �����մϴ�. ���ð濡�� �ǽɵ� ���� �ְ� ������ ���ɰ˻縦 �� �� �ֽ��ϴ�. ���� esophagography�� ���� �������̰� �����մϴ�.
Refractory GERD ȯ�ڿ��� achalasia�� �����ϱ� ���Ͽ� esophagography�� �غ��� ����? Fancy�ϰ� ���� �˻翡 �ռ� �����ǰ� ���������� ������ ������ esophagography�� ���մϴ�.
![]() 2. Endoscopic findings of achalasia
2. Endoscopic findings of achalasia
Endoscopy is usually the first examination for various upper GI symptoms. Symptoms of achalasia may be vague, especially for the first couple of years. If achalasia is endoscopically suspected based on following findings, it really helps the patients.
| Endoscopic findings of achalasia | |
|
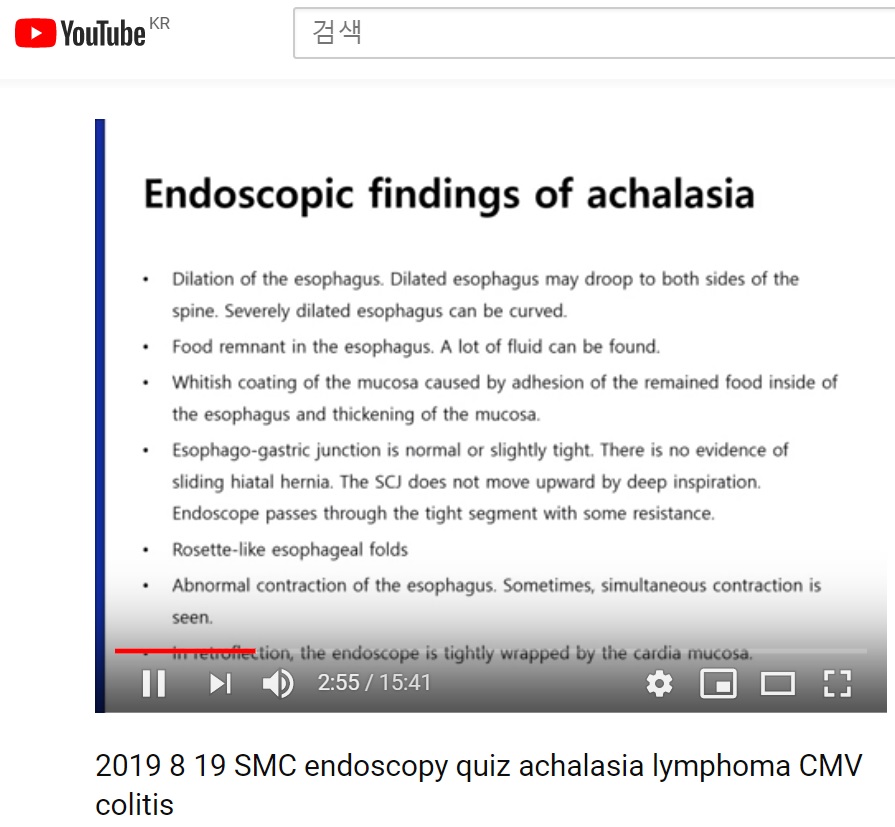

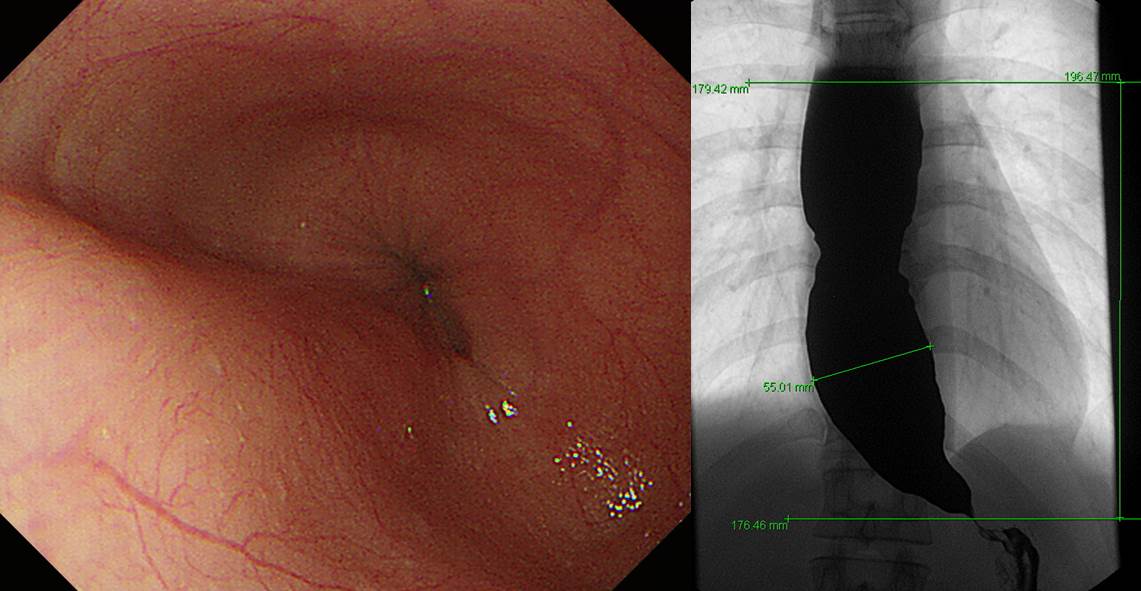
�ĵ��� ũ�� Ȯ��Ǿ� ��������� spine�� Ƣ��� ���Դϴ�. "Dilated esophagus may droop to both sides of the spine."��� ǥ���Ǵ� �����Դϴ�.
Chest CT ��ٰ� �쿬�� �߰�. �ڼ��� �����غ��� dysphagia�� ���� ������ �־��ٰ� ��.
Achalasia�� �ʹ� ���Ͽ� ��� ���� ȣ������ ���Ͽ� intubation���� ����
���Ĺ��� ���κ� ������ �� ���ð��� �Ͽ��� �� ������ �ĵ��� ���Ĺ��� �����ְ� �ĵ��� �ſ� Ȯ��Ǿ� ������ GE junction�� �ణ tight�Ͽ���. �ĵ��� ũ�� curved �Ǿ� ����.
�������� ���� ������ �����Ͻ� ���Դϴ�. GE juction ����� �� ���װ��� �������� ������~~ �ĵ�ü�ΰ� �о��� �ִ� ����̸� �ĵ��� ������ ���� ��ü�� ���� �־����ϴ�.
5�Ⱓ ��ģ ������ �־��� ���� ü���� ������ ���Դϴ�. ���� ���ð� �� ������ �ĵ������� ���� �� �ִٰ� �մϴ�. ����, ���ð� ������ �ڼ��� ���� EG junction�� tight �ϰ� �Ϻνĵ��� �þ ����Դϴ�. �ĵ� ������ �ִ� ������� �� ���� �Ұ��� ���̸� achalasia�� �ǽ��� �� �־�� �մϴ�.
Type II achalasia������ POEM���� ġ���Ͽ��� ������ ������ ȣ���� �־���
40�� ����. ���ð濡���� ���ٸ� clue�� ã�� �������� �쿬�� ������ PET���� �ĵ��� �þ �ִ� ���� �߰��Ͽ� �ڴʰ� achalasia�� ���ܵǾ���. ���ð� ������ �ٽ� ���� achalasia�� �ǽ��ؾ� �ϴ� ��Ȳ��. (2017)
40�� ���� (2017)
Hiatal hernia�� ������ achalasia
Achalasia�� ���Ͽ� ȯ�ڰ� ����� �� �ֽ��ϴ�. 80�� �������� aspiration pneumonia�� �Կ��ϼ̴µ� �ſ� ���� achalasia�� Ȯ�εǾ����ϴ�. Aspiration pneumonia�� ���������� ��ȯ�ڽǿ��� �ΰ�ȣ������� ����� ���� ���� ����� ���Դϴ�. (2018��)

���Ĺ��� �����ϰ� ������ �Ұ�
�Ϻ� �����糢 ������ Minami ���� 2015�� �������� �ű�ϴ� (Minami. PLos One. 2015)). Minami ���� ���ź��� �˷��� �ĵ��̿ϺҴ����� ���ð� �Ұ��� �����ϸ鼭 "Pinstripe Pattern"�̶�� ������ '���ð� �� longitudinal wrinkcle'�� �Ұ��Ͽ����ϴ�. POEM�� �ϸ� pinstripe pattern�� �������ٰ� �մϴ�. Pinstripe pattern�� kappa ���� 0.61�� food/liquid remnant �Ұ��� 0.69 �� ����߽��ϴ�.
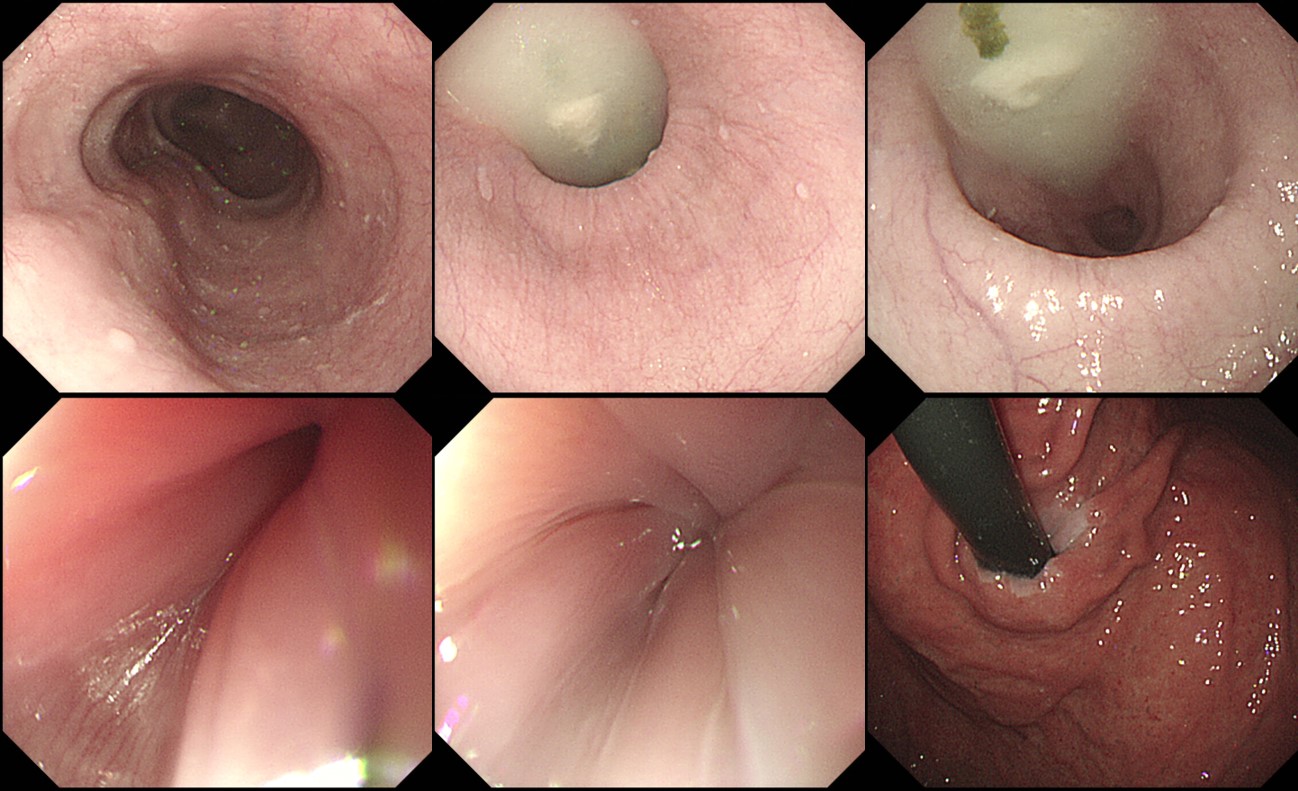
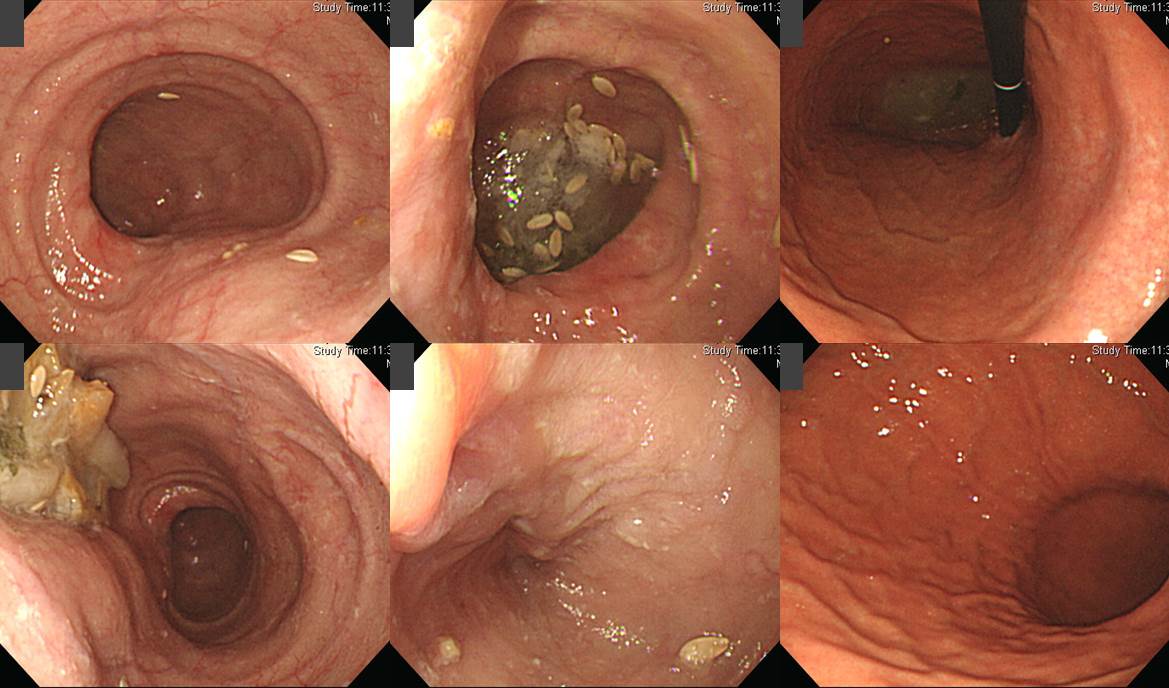
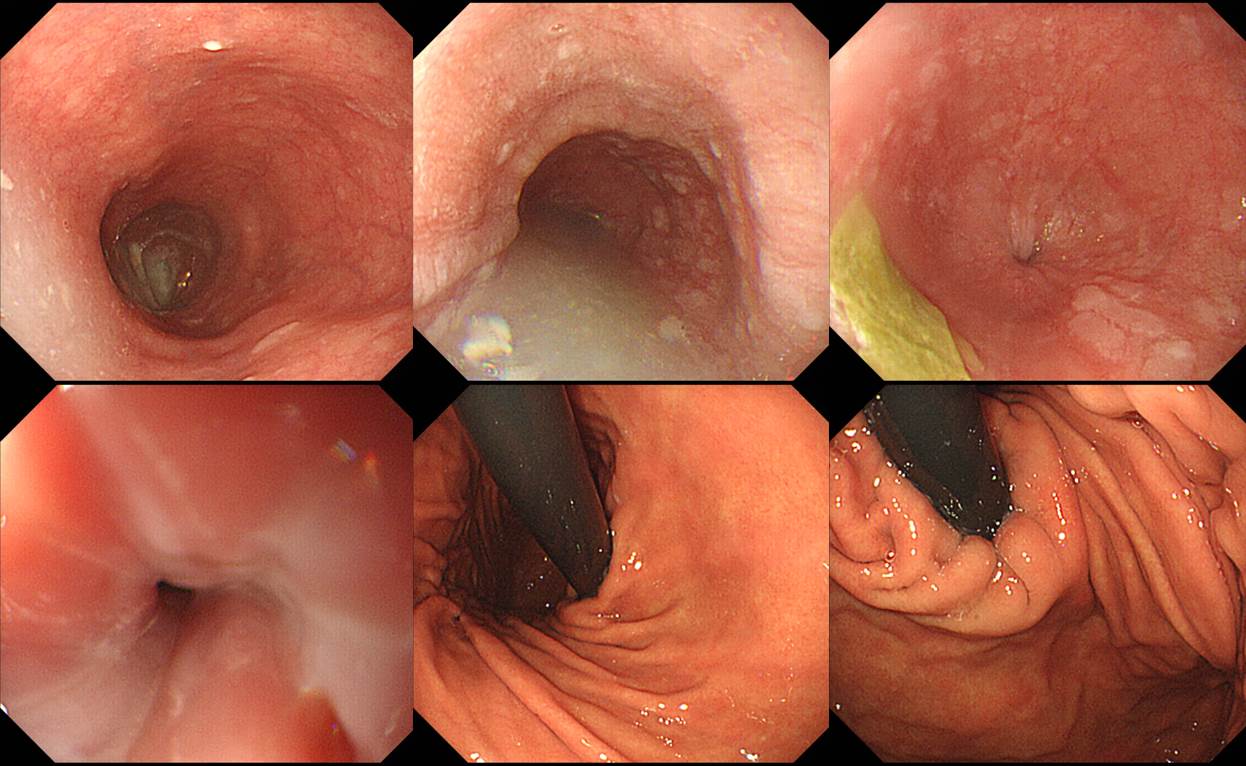
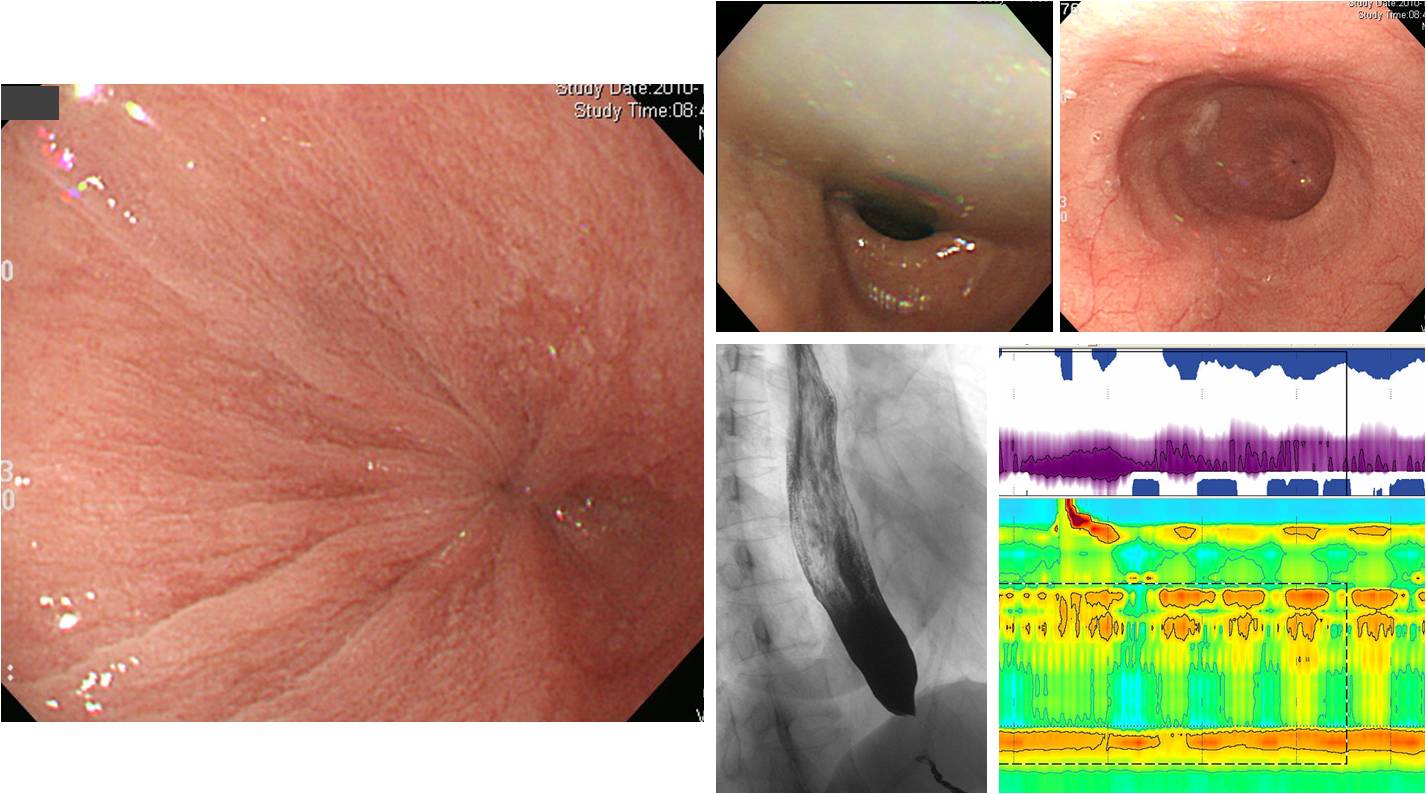
Typical findings of primary esophageal achalasia. (a) Dilation of the esophagus. Dilated esophagus drooped to both sides of the spine. (b) Food remnant in the esophagus. (c) Whitish coating of the mucosa caused by adhesion of the remained food inside of the esophagus and thickening of the mucosa. (d) Functional stenosis of the esophago-gastric junction. Endoscope passes through the tight segment with some resistance. (e) Abnormal contraction of the esophagus. Simultaneous contraction is clearly observed.
Pinstripe pattern (PSP). (a) Minute superficial wrinkle was observed on the mucosal surface. (b) Indigocarmine spraying made the superficial structure clearer. (c) Magnifying observation after indigocarmine spraying. Slight gap was observed between each longitudinal line. (d) NBI Image with magnification. The gap observed by magnifying chromoendoscopy was also identified via NBI magnification. Each superficial microvessel was substantially transparent at the gaps between stripes.
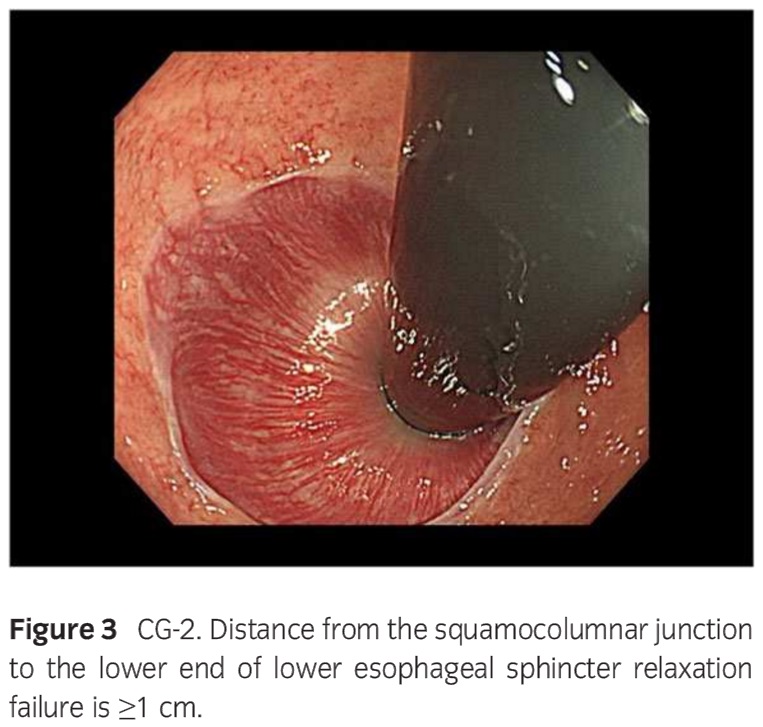
Showa ������ Gomi ���� Champagne glass sign�� �����Ͽ����ϴ� (Gomi K. Digest Endosc 2016). "CG-0 was seen in 73 patients (28.0%), whereas the CGsign was seen in 186 patients (71.3%), of whom 170 (65.1%) wereCG-1 and 16 (6.1%) were CG-2."
Different types of champagne glass (CG) sign. LESRF, lower esophageal sphincter relaxation failure; SCJ, squamocolumnarjunction.
![]() 3. Manometric and other diagnostic tools of achalasia
3. Manometric and other diagnostic tools of achalasia
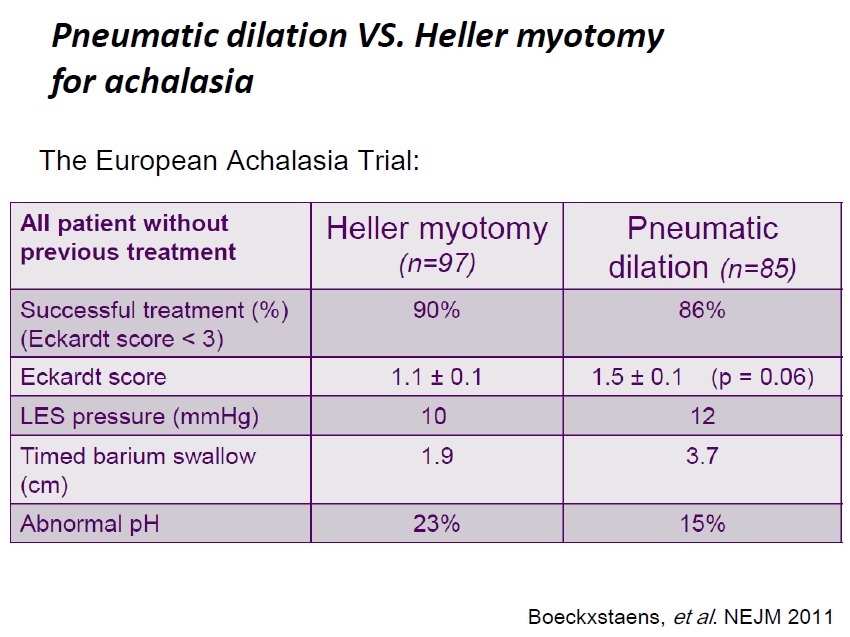
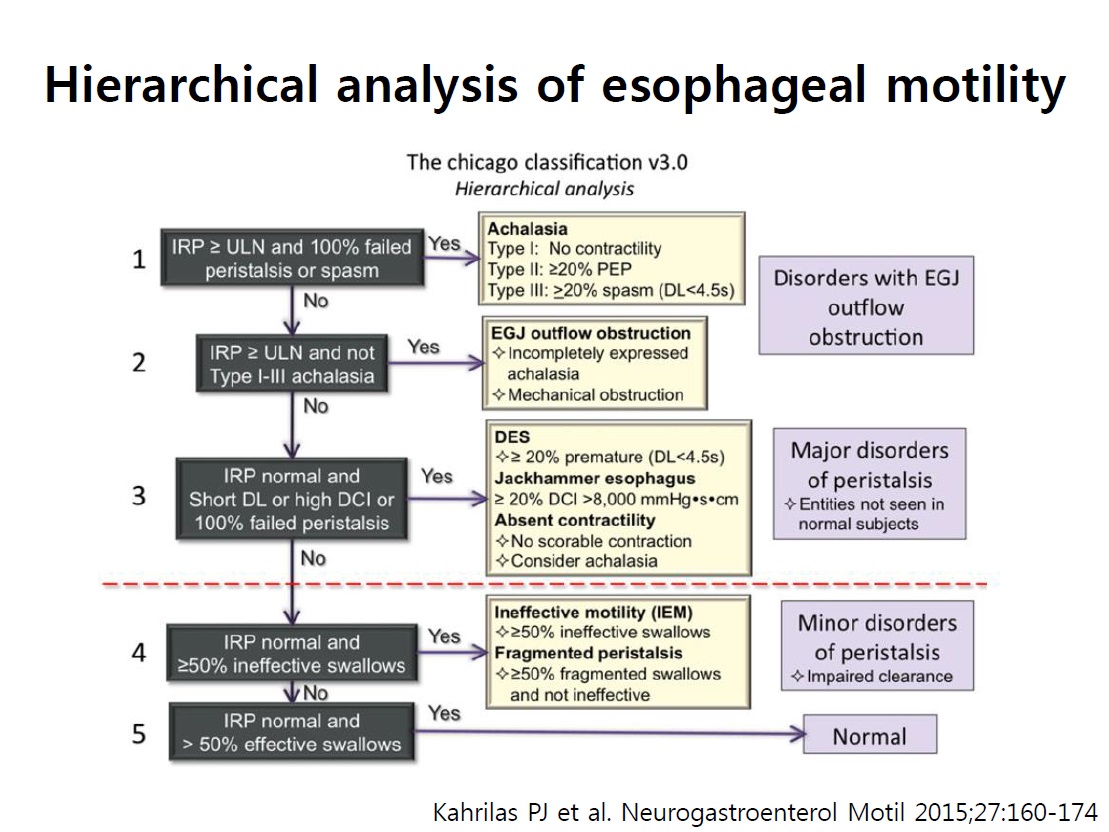
Achalasia�� ���ϴ� fancy�� ����� ������ �ټ� �������� �� �ִ� barium swallow�� �ణ ������ timed barium swallow���� ������ �����մϴ�. Pneumatic dilation�� Heller myotomy�� ���� �Ʒ� ���������� �ֿ� �����ǥ�� �ϳ��� ���ǰ� �ֽ��ϴ�.
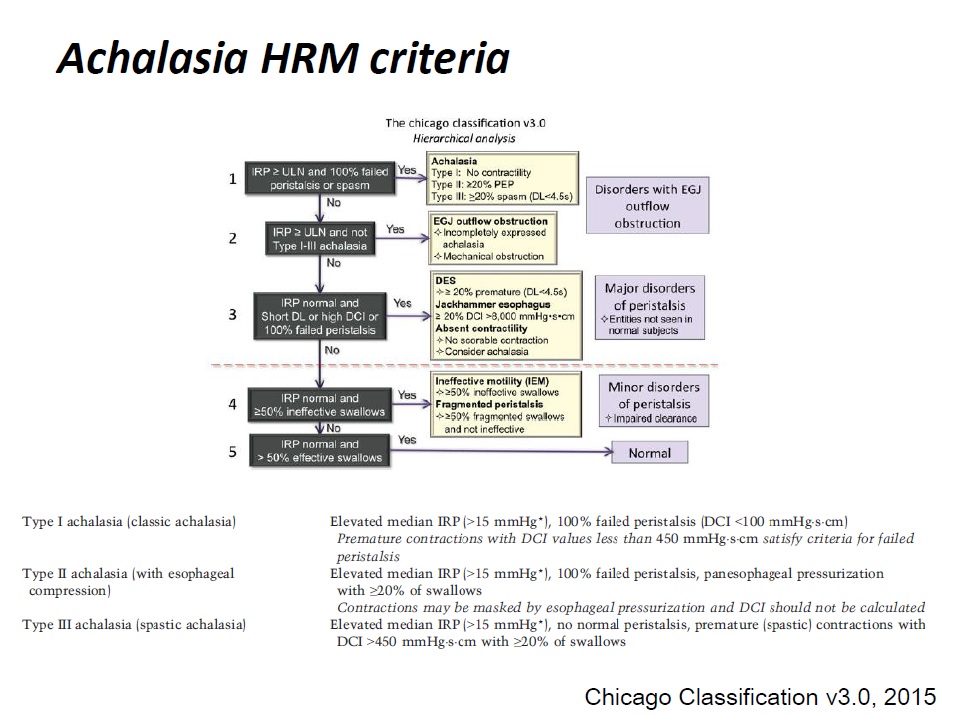
Chicago version 3.0 PDF 2.9M
PPT PDF 2.6M ���ο� (��ȣ ����)
![]() 4. Structures of EGJ
4. Structures of EGJ
[Microvasculature of the esophagus and gastroesophageal junction] (World J Gastrointest Endosc 2016) - PDF
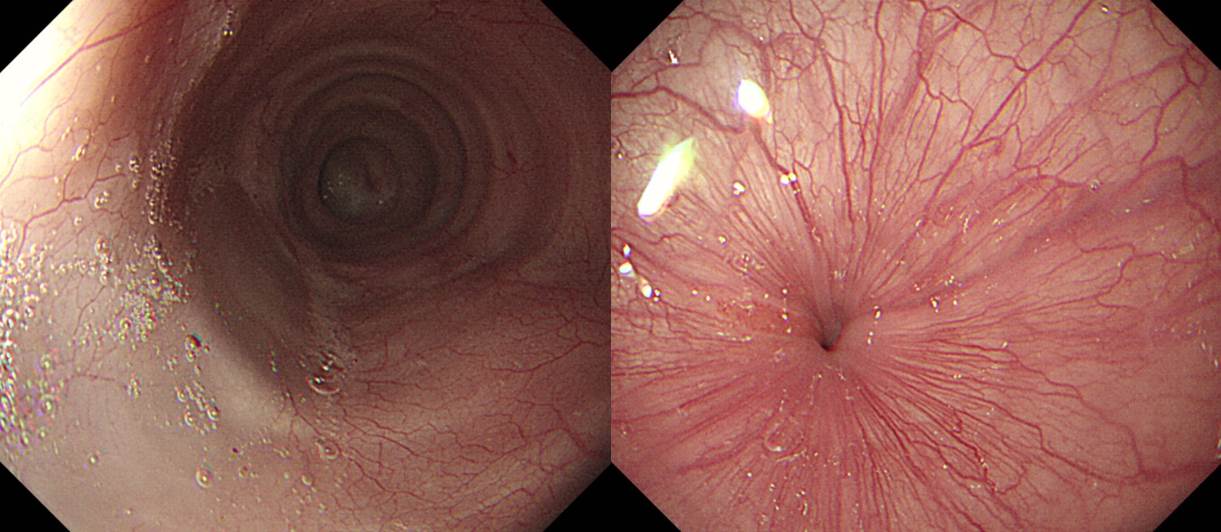
Mucosal vessels. A and C: Endoscopic images during per-oral endoscopic myotomy procedure (high magnification images); after unintentional removal of the epithelium (white layer), top half of epithelium was peeled off, and IPCLs were exposed. IPCLs appear as regularly-arranged, red dots (A: White light) or dark green spots (C: NBI); B: A schematic representation of the vascular network of esophageal mucosa: a: Branching vessels; b: SECN (Sub-epithelial capillary network); c: IPCL (Intrapapillary capillary loop)
A: Perforating vessels from the outer esophagus to the submucosal vessel; image captured during tunnelization in POEM (bottom side muscle layer, left side submucosal lifting); B: Submucosal drainage vessel (mucosal layer lifted on during ESD). These veins can become esophageal varices in portal hypertension; C: Submucosal vessels connecting the drainage veins to the mucosal branching vessels (in the lamina propria); D: Spindle veins immediately below the GEJ (in left side of the image, in blue, the submucosa and in the right side the muscle); E and F: branching vessels (seen from inside the submucosal tunnel). G: palisade vessels.
High magnifying narrow band imaging image of normal esophageal mucosa (luminal side). A: Soft pressure of the endoscope distal attachment (��hood��) onto the mucosal surface demonstrates SECN, hard pressure onto the mucosa compresses horizontal vessels, allowing clear observation of IPCLs; B: In the circle the SECN located at the top layer of lamina propria mucosae, just beneath the epithelium. The black arrows indicate the branching vessels into the lower lamina propria; white arrows indicate the IPCL located in the epithelial papilla, which is a projection of lamina propria mucosae into the epithelium.
The figure shows the histology of a non-pathologic esophageal specimen. The vessels�� wall has been colored by CD34, showing superficially the IPCLs (upper part of the lamina propria, arising the epithelium) and the SECN; deeply in the lamina propria the branching vessels. In the sumucosal layer also the drainage veins are evident. The table summarizes the vascular system observed and its own esophageal layer according to the different endoscopic procedure performed.
In the center a scheme of the submucosal view at the gastro-esophageal junction during per-oral endoscopic myotomy. At the muscle side (left endoscopic image) the spindle vein are clearly visible; at the mucosal side (seen on its backside, right endoscopic image) the palisade vessel are recognized. High magnification images.
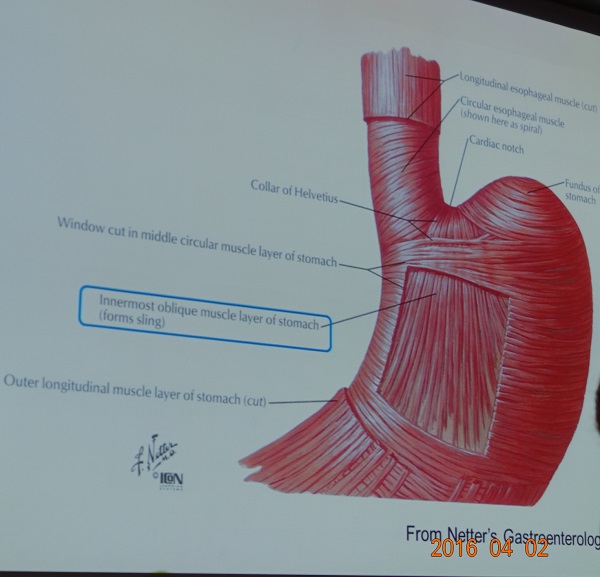
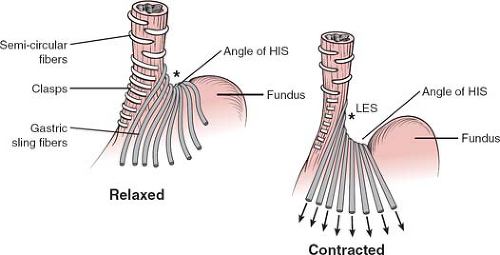
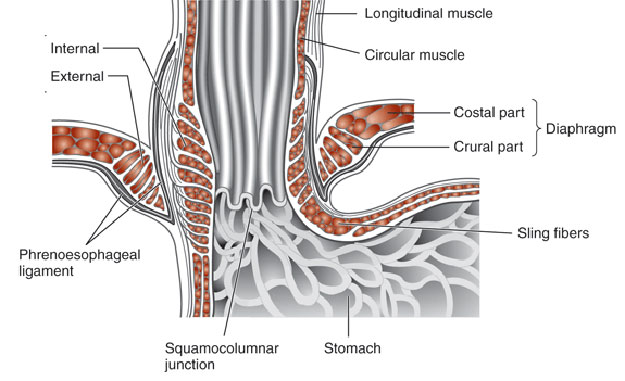
[Intrinsic components]
Semicircular claps fibers centered along the lesser curve (3 o'clock)
Oblique slin fibers centered along the posterolateral wall (7 o'clock) wraing around the anterioa (11 o'clock) and posterior (5 o'clock) walls.
[Extrinsic components]
Crural diaphragm & phrenoesophageal ligament that fasten the esophagus to the diaphragm
![]() 5. Lectures on POEM
5. Lectures on POEM
![]() 1) 2014-12-7. The role of POEM (���ѻ��������︮�ڹ�����ȸ �߰��м���ȸ Ư��. �ƻ꺴�� ���ƿ�)
1) 2014-12-7. The role of POEM (���ѻ��������︮�ڹ�����ȸ �߰��м���ȸ Ư��. �ƻ꺴�� ���ƿ�)
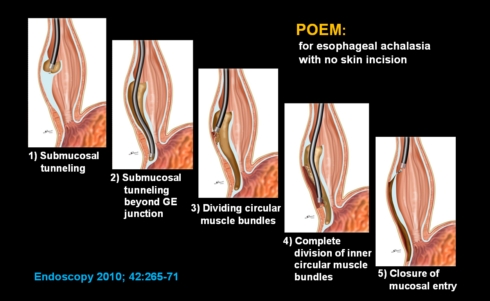
Related image from the Internet�Ϻ��� Dr. Inoue�� ������ POEM (peroral endoscopic myotomy for achalasia)�� achalasia���� ���� ���� ����ǰ� �ֽ��ϴ�. 2010�� Endoscopy���� �Ǹ� Dr. Inoue ������ ���� �ο�ǰ� �ֽ��ϴ�. Dr. Inoue�� �� 300�� ������ ������ �ִٰ� �մϴ�. �߱� �������� PH. Zhou �ڻ�� 2000�� �̻���, �ε��� A. Maydeo �������� 600�� �̻��� �����ߴٰ� �մϴ�. ���ƿ� �������� Learning curve�� 20�� ������ �Ǵ� �� ���ٰ� �Ͻʴϴ�.
Classic achalasia�̰� �ĵ� ü�ο� �̻��� ������ ª�� �߶� ������ �ĵ� ü�ο� spasm�� ������ ���� ��ο������� LES �Ϲ���� ��� �߶��־�� �մϴ�.
Inoue �� TT knife�� ���濡�� ���Ϲ����� 2�� �������� �ڸ��� ���� �����ϴµ�, ���ƿ� �������� hook knife�� �̿��Ͽ� �Ʒ����� ���� �ڸ��� ����� ��ȣ�Ѵٰ� �մϴ�.
POEM �� ������ ������ ���������� esophagography�� delayed emptying, manometry�� �̻�Ұ� ���� ũ�� �������� �ʴ� ��찡 ���ٰ� �մϴ�. Subjective�� ������ objective�� ������ ���̰� �����ϴ� �ְ����� ������ �߿���ؾ� �Ѵٰ� �����˴ϴ�.
Achalasia�ε� POEM�� ������� ȯ�ڰ� ���������� tracheobronchial remnant�� ���ܵ� �Ҿ�ȯ�ڸ� �Ұ��Ͽ� �ּ̽��ϴ�. Congenital anomaly�� �ϳ��ε� segmental resection���� �� ġ��Ǿ��ٰ� �մϴ�.
������ ���� �� �Ʒ��� ���� ����� ���� �λ����̾����ϴ�.
"1995�� �������� ���ð�ġ�Ḧ ó�� ������ �� ȯ�ڰ� �����ϴ� ������ ���Ͽ� achalasia ȯ�ڰ� POEM �� �����ϴ� ������ 100��� �˴ϴ�. ȯ�� ���忡�� �ѹ� ġ�� �� ���� ���� ���� �������� �ü��� POEM�Դϴ�. ȯ�ڵ��� �ſ� �����մϴ�."
![]() 2) 2015-5-8. Recent advances in the diagnosis of achalasia (���հ��Ǵ� ����)
2) 2015-5-8. Recent advances in the diagnosis of achalasia (���հ��Ǵ� ����)
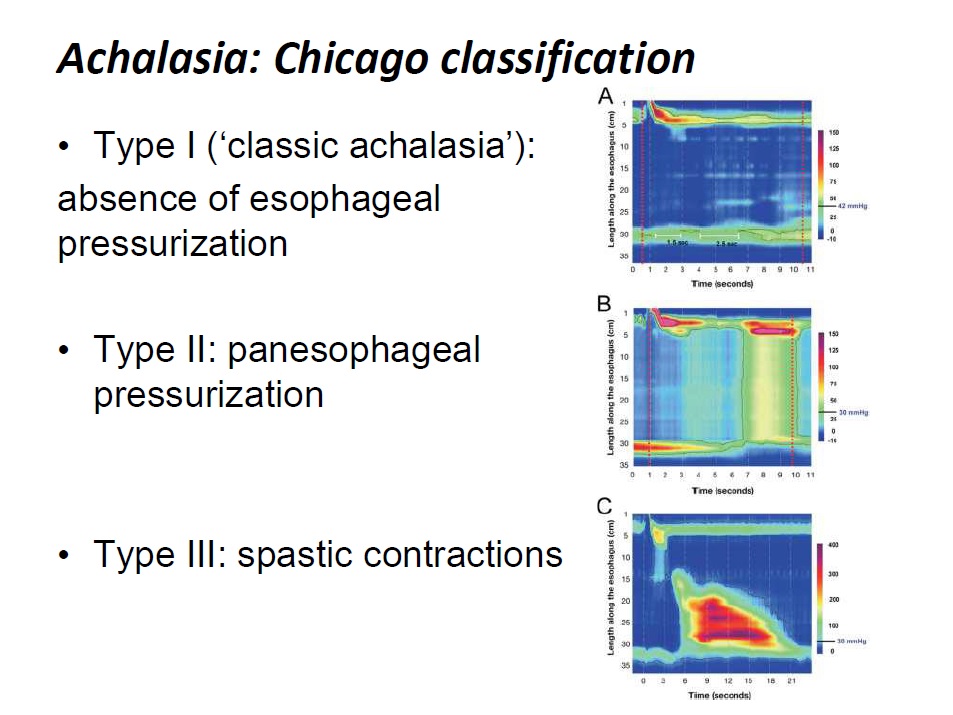
Vigorous achalasia�� ġ��ȿ���� �����ϱ� ��������ϴ�. Heterogenous�� group�̾��� �����Դϴ�. High resoluation manometry�� vigorous achalasia�� type II�� type III�� �������ݴϴ�. �ĵ� ü���� pressurization�� �����ִ� type II�� ���İ� ���� ���Դϴ�. �Ϻνĵ��� spasm�� ���̴� type III�� ȯ�� ���� ������ ���Ĵ� ���� ���� �����Դϴ�.
NOTES�κ��� ���ߵ� submucosal tunnel technique�� �پ��ϰ� ��ȭ�ϰ� �ֽ��ϴ�. ���� ���� �ǿ�ȭ�� ���� POEM�Դϴ�.
POEM�� ���� �ֱ� ����Դϴ�. ��� ȯ�� ���� ������ type III������ ȿ���� �ִٴ� ���� �����ְ� �ֽ��ϴ�.
![]() 3) POEM in China
3) POEM in China
2015�� 3��ȣ Gut and Liver�� �߱��� Quan-Lin Lin�� Ping-Hong Zhou ������ POEM�� ���� ��̷ο� ���並 �Ǿ����ϴ� (Perspective on POEM for achalasia: Zhonshan experience).
POEM �ü��� ������ �̱� �ػ罺�� �ð� Galveston�� Pasricha ������ 2007�� ���������� ���Ͽ� �����Ͽ����ϴ� ��ũ). �̱� ������� ������� �����ϴ� ���� �����ϴ� ���̿� �Ϻ��� Inoue ������ ���ʿ��� �������� ���� �˷Ƚ��ϴ� (��ũ). �̸� �� �߱��� Quan-Lin Lin�� Ping-Hong Zhou ������ �ܱⰣ�� �ſ� ���� �ü��� �������� ���� �ְ� �밡�� �Ǿ����ϴ�. �̹� ���並 ���� 1,300���� �ߴٰ� �մϴ�. �� ���� POEM�� ���� �̻��� �� ���Ϳ��� �ߴٰ� �ڶ��ϰ� �ֽ��ϴ�. ���� ���������Դϴ�. �߱��� Ư�� �ü��� Ư�� �ǻ翡�� �о��ִ� ������ �ֽ��ϴ�. �ݹ� n-���� ���� �ְ��� �˴ϴ�.
���� (1) posterior wall incision, (2) full-thickness myotome, (3) a push-and-pull technique for myotome, (4) water-jet assisted POEM�̶�� 4������ ��Ư�� ������� �����Ͽ����ϴ�. �̸� ���Ͽ� �ſ� ���� �ӵ��� �ڶ��ϰ� �ֽ��ϴ�. �� �� �ü��� �� ���� �ִµ� ���� ���İ��� �����ϴ�. ���õ��� ���� �ְ��Դϴ�. �̹� ���信�� ��̷ο��� ���� �� ���� �ű�ϴ�.
- Relative indication: other hypertensive motor disorders (diffuse esophageal spasm, nutcracker esophagus, jackhammer esophagus)
- We routinely divide muscle fibers over a minimum length of 6 to 8 cm in the esophagus and at least 2 cm onto the cardia.
- Posterior myotomy in the 5- to 6-o��clock position also achieves myotomy from the luminal side without disturbing the acute angle of His, which is located at the 8-o��clock position: this is important to prevent reflux.
- A clear separation of circular (to be completely dissected) and longitudinal (to be left) muscular layers cannot be found any more at the EGJ and stomach.
- Full-thickness myotomy significantly reduced the procedure time but did not increase the procedure-related adverse events or clinical reflux complications.
- A Sengstaken-Blakemore tube is particularly effective for providing compressive hemostasis to staunch post-POEM bleeding.
![]() 4) Achalasia & POEM (2015�� 8�� 29�� ���� motility symposium)
4) Achalasia & POEM (2015�� 8�� 29�� ���� motility symposium)
1) ������ ������ ���� �߿���
2) Hitomi Minami (Nagasaki University) ������ ���� �߿���
![]() 5) 2015-10-31. ��1ȸ ���ĵ�������ȯ��������ȸ �м���ȸ. POEM - �������б� ������
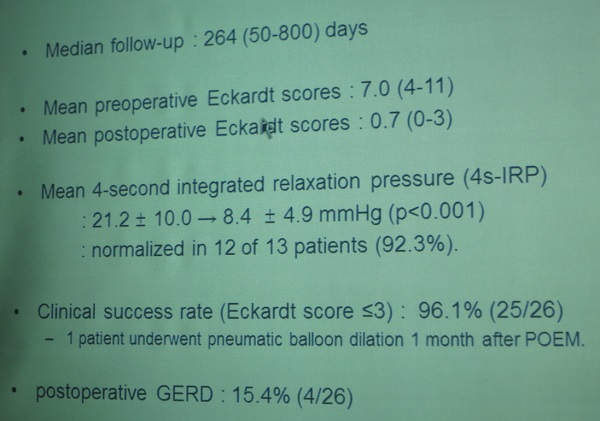
5) 2015-10-31. ��1ȸ ���ĵ�������ȯ��������ȸ �м���ȸ. POEM - �������б� ������
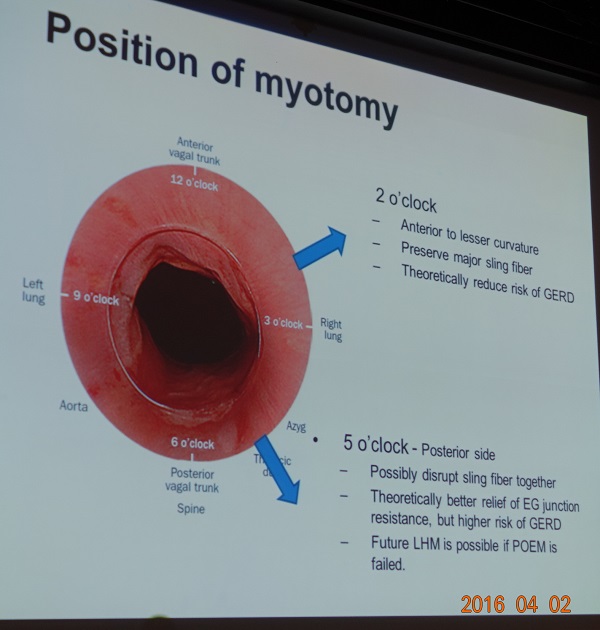
Anterior vs Posterior myotomy
- Anterior myotomy: continuing toward the lesser curve of the stomach potentially avoides damage to the sling collar muscle, which is major component of the angle of His → to minimize post-procedure reflux (Angle of His�� �����ȴٴ� �ǹ�)
- Posterior myotomy: better relief of dysphagia because of sling fibers but at the expense of mild reflux (Angle of His�� �������ٴ� �ǹ�)2015�� 8������ �������б�(����+����)������ POEM 22���� �����Ͽ��ٰ� �մϴ�. ������ �ſ� ���ҽ��ϴ�.
Patel ���� �м��� ���� �ֱٱ����� �ڷ��Դϴ� (Patel K. Dis Esophagus 2015). �� ������ �� ���� ������.
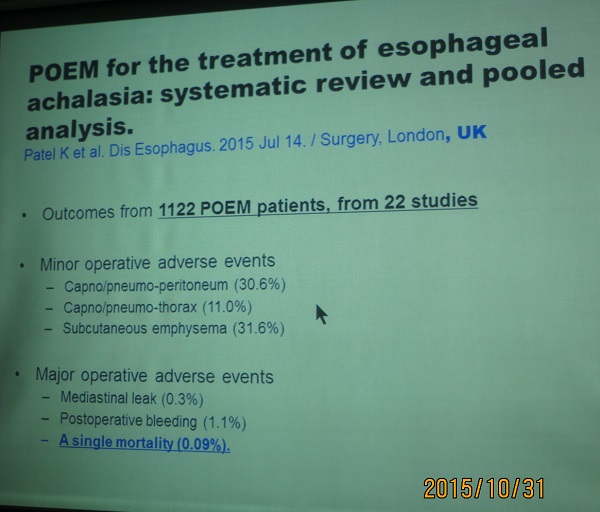
Minor operative adverse events included capno/pneumo-peritoneum (30.6%), capno/pneumo-thorax (11.0%) and subcutaneous emphysema (31.6%). Major operative adverse events included mediastinal leak (0.3%), postoperative bleeding (1.1%) and a single mortality (0.09%). There was an improvement in lower esophageal sphincter pressure and timed barium esophagram column height of 66% and 80% post-POEM, respectively. Symptom improvement was demonstrated with a pre- and post-POEM Eckardt score �� standard deviation of 6.8 �� 1.0 and 1.2 �� 0.6, respectively. Pre- and post-POEM endoscopy showed esophagitis in 0% and 19% of patients, respectively.
![]() 6) 2016-4-2. APNM2016. Options for achalasia (������ ������)
6) 2016-4-2. APNM2016. Options for achalasia (������ ������)
[������ ��] Anterior approach�� posterior approach �� ��� ������ ������ ������ ���ҽ��ϴ�. Endoscopy�� 2020�� 4���� �Ǹ� meta-analysis(PMID: 31958861)�� ����� �ű�ϴ�. "Anterior and posterior myotomy in POEM seem cparable to each other in terms of clinical success, GERD and adverse events. The total proceture time with posterior myotomy seems to be shorter than with anterior myotomy."
���������� myotomy ��ġ�� ���Ͽ� ���� �����ϼ̽��ϴ�. 2�� ������ sling fiber�� �����ǹǷ� POEM �� GERD�� �� ���ϰ�, 5�� ������ sling fiber�� disrupt�ǹǷ� EG junction relief�� �� �����ϴ�. �ֱٿ��� ��κ��� �ü��ڰ� 5�� ����(posterior approach)�� ��ȣ�մϴ�. Ȥ�ڴ� 5�� �������� �ü��ϴ��� ���ɽ����� �ü��ϸ� sling fiber�� �츱 �� �ִٰ� �մϴ�. ���ð��� �ڿ������� ��� ���� �����ϱ� ���� ���� �ڸ��� �װ��� �밭 5�� �����Դϴ�.
�Ϻ��� Dr. Inoue�� ���ſ��� 2�� ������ ��ȣ�ϴٰ� �ֱٿ��� 5�� �������� �ü��ϰ� �ִٰ� �մϴ�. Dr Inoue�� �ֱ� review���� �ش� �κ��� �ű�ϴ� (Bechara R, Inoue H. Gastrointest Endosc 2016 - Epub).
The techniques used to perform a selective myotomy vary depending on the position of the mucosal incision as well as endoscopic orientation. When the muscle layer is in the 12 o��clock and the mucosa at 6 o��clock position (generally for anterior myotomy), acute tip angulation is required to hook the circular muscle layer. In contrast, when the muscle is kept in the 6 o��clock position (generally for posterior myotomy, which is our current practice), much less tip angulation is required and there is less "fling" of the knife.
Dr. Fass�� �̱������� POEM �� GERD�� �ξ� ���ϰ�, stricture�� ���� ���Ѵٰ� �ڸ�Ʈ �ϼ̽��ϴ�. .
Dr. Fass�� EG junction outflow obstruction�� POEM�� �������� �Ǵ��� �����Ͽ���, ���������� possible future indication�� �� ������, ���� �� ��ȯ�� �� ���� ���ϰ� botox�� ġ��Ǵ� ��찡 ���� ���� �ü����� �ʴٰ� ���ϼ̽��ϴ�.
![]() 7) 2016-6-26. Achalasia and POEM symposium at IDEN2016
7) 2016-6-26. Achalasia and POEM symposium at IDEN2016
(1) Evaluation of achalasia (���Ŵ��б� �ڹ���)
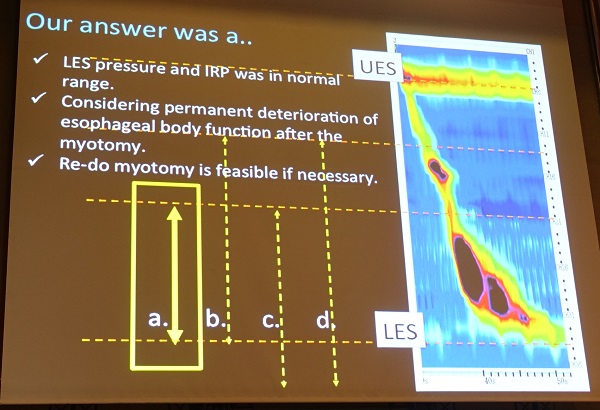
Achalasia�� high resolution manometry �Ұ��� �������� �Ʒ��� ���� subtype���� ���� �� �ֽ��ϴ�. �̷��� subgroup�� ���� ���̰� �Ұ߿� ���̰� �ִٰ� �մϴ�. �� achalasia�� pathogenetically heterogeneous group�� ���Դϴ�.
FLIP�� GE junction�� ����� �����ִ� ����ε� Carlson DA ���� ���ο� ���α��� �̿��Ͽ� FLIP topography plot�� �����ִ� ����� �����Ͽ����ϴ� (Carlson DA. Gastroenterology 2015).
* ����: EndoTODAY FLIP
(2) Early experience of POEM in Korea (��õ�� ���б� ȫ����)
ȫ���� �������� 2012�� 8�� 8�� ù POEM �ü��� �Ͽ����ϴ�. ȫ�������� �ֱٿ��� HybridKnife T type (ERBE, Germany)�� �ַ� ����Ѵٰ� �մϴ�. (������ comment: ������ ��� �� ������...) Myotomy ������ ���ſ��� 1-2�ø� ����Ͽ����� �ֱٿ��� 4-5�ø� ����Ѵٰ� �մϴ�.
(3) POEM in Japan (Hitomi Minami. Nagasaki University, Japan)
�ü� ���� bleeding�� ���ϸ� �þ߸� ���� �� �����Ƿ� �����ؾ� �մϴ�. Pneumoperitoneum�� ���ϸ� ���⸦ �� �־�� �ϴ� ��찡 �����Ƿ� ���θ� �� �� �� �ֵ��� �ؾ� �մϴ� ("direct visualizaion).
Jackhammer esophagus ȯ�ڿ��� myotomy�� ���̸� ���ϴ� �Ϳ� ���Ͽ� ���� �����Ͽ����ϴ�. LES function�� ���� ���� ���Ͽ����ϴ�.
Minor mucosal injury 2.8% (true perforation�� �ƴϰ� touch�� ���� burning)
Minami �������� 3 ���� clinical questions�� �����ϰ� �ǰ��� �ּ̽��ϴ�.
3 clinical questions (1) Does previous interventions affect feasibility and safety of POEM?
A. Severe fibrosis and anatomical change due to previous interventions could complicate the procedure. However, it is still feasible. (Onimaru M, Inoue H. J Am Coll Surg 2013;217:598-605, Vigneswaran Y. J Gastrointest Surg 2014)
(2) How long do we have to cut the muscle?
A. Still inconclusive. If the abnormal contraction of the esophageal body was only a secondary change, myotomy should not be too long in order to avoid dysfunction of the esophageal body.
(3) Which is better? Anterior? Posterior?
A. Longer observation with more cases is awaited. Multicenter RCT is now ongoing.
���ֿ� ����Բ����� simultaneous bilateral POEM�� ���Ͽ� �����ϼ̴µ� Minami �������� �ü� ������ ���ٰ� ���ϼ̽��ϴ�.
![]() 8) 2016-7-25 �Ͽ����ð汳�� �����ȭ������ȸ �ξ�� ������ ����
8) 2016-7-25 �Ͽ����ð汳�� �����ȭ������ȸ �ξ�� ������ ����
Pneumatic dilatation�� �ô�� ���� POEM�� �ô밡 �Խ��ϴ�.
![]() 9) 2016-11-4. JDDW POEM and beyond (Haruhiro Inoue)
9) 2016-11-4. JDDW POEM and beyond (Haruhiro Inoue)
Vigorous achalasia������ myotomy�� ��� �� �ʿ䰡 �ֽ��ϴ�. Inoue �������� 23 cm myotomy�� �����Ͽ��� ���ʸ� �����־����ϴ�. �����δ� �̷� �� myotomy�� �� �� ���� ������ �� myotomy�� �� �� �ִٴ� ���� ���ð� ġ���� ���� �� �ϳ��Դϴ�.
Jackhammer esophagus������ �� myotomy�� �ʿ��մϴ�. ���ݱ��� 1000������ POEM �� 5������ Jackhammer esophagus�� �־��ٰ� �մϴ�. Jackhammer esophagus���� body myotomy�� �Բ� LES myotomy�� �ʿ������� ���� �Ҹ�Ȯ�մϴ�. Inoue ������ ù Jackhammer esophagus ȯ�ڿ��� body myotomy�� �ߴµ� 3�� �� achalasia�� ���Ͽ� �ٽ� POEM�� �߽��ϴ�. �� ���ķδ� body myotomy�� LES myotomy�� �Բ� �ϰ� �ִٴµ� GERD�� ���ϴ� ���� ������� �մϴ� .
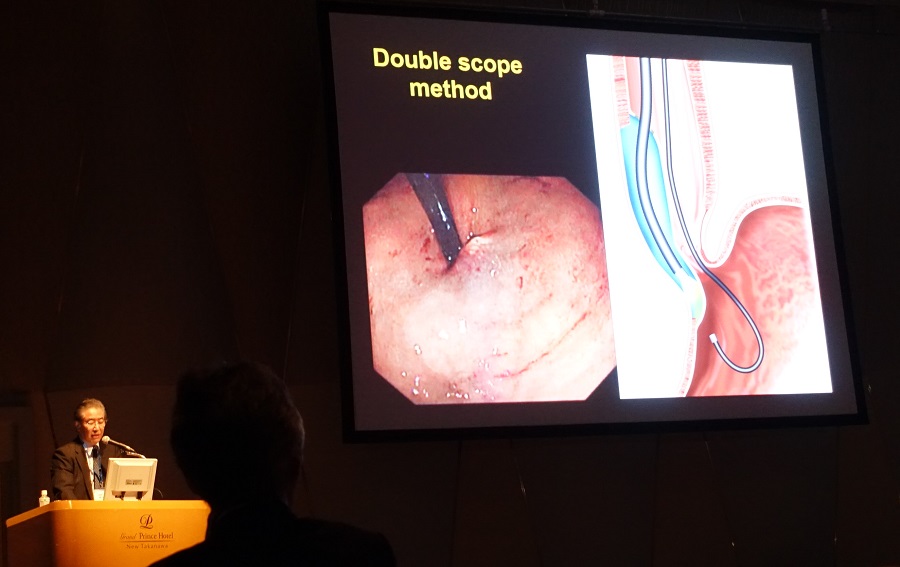
Inoue �������� two endoscopy method�� ���� ����Ѵٰ� �մϴ�.
POET (Peroral endoscopic tumor resection): aberrant pancreas in the esophagus ġ�� ���� �����־����ϴ�. �������� �ѹ� �ݺ����� ������ ����� ȯ�ڰ� �ĵ��� pancreatic duct opening�� �־����ϴ�. POEM�� ����� ������� ġ���ߴٰ� �մϴ�.
Inoue �������� laparoscopic Heller myotomy�� �������� �� �̻� ���ٰ� ���ϸ鼭 historical �ü��� �Ǿ��ٰ� ����Ͽ����ϴ�.
Anterior myotomy�� ������ ������ �� ������ big perforating artery�� �ִ� ȯ�ڰ� �ִ��� ���Դϴ�.
Lateral myotomy�� ���� �ʽ��ϴ�. �ĵ��� lateral ������ ��� ��� �����̹Ƿ� �������� ���Ͽ� POEM �� ū diverticulum�� ���� �� �ֱ� �����Դϴ�.
![]() 10) 2017-6-4. Third space endoscopy for submucosal tumor - from POEM to POET. Haruhiro Inoue (Showa U, Tokyo, Korea)
10) 2017-6-4. Third space endoscopy for submucosal tumor - from POEM to POET. Haruhiro Inoue (Showa U, Tokyo, Korea)
Diffuse esophageal spasm ���ʴ� LES myotomy�� ���� �ʰ� esophageal body�� ��� myotomy�� �� �ְ� �ֽ��ϴ�.
Gastric POEM G-POEM�� very simple procedure�Դϴ�. Entry site�� myotomy site�� �ſ� ������ �����Դϴ� (�� ������ ����Ҵµ�.... myotomy�� ���̰� 2cm�� ª�� ������ submucosal tunnel�� ª�Ƶ� �ǰ� �ü��� ����� �ʴٰ� �մϴ�). Duodenal muscle�� �ſ� thin�Ͽ� �������� ������ myotomy�� ���� �ʽ��ϴ�.
POET (peroral endoscopic tumor resection) - endoscopic submucosal tumorectomy�� POEM ����ϰ� �ü��ϴ� ���Դϴ�.
Full layer resection in the esophagus (ectopic pancreas�� repeated mediastinitis�� �����״� ���)��� ����� ������ �ü��� �Ұ��ϼ̽��ϴ�.
Preservation of the mucosa intact is the most important.
Hook knife�� ����� ���ʰ� �־ ������ �ߴµ���... ������ triangle knife�� ��������� �ſ� ��ٷο� ���, fine�� �ü��� �ؾ��ϴ� ��쿡�� hook knife�� ����ϱ �Ѵٰ� �մϴ�.
[������ comment] IDEN 2017 Inoue ������ ������ �����鼭 ������ �η������ϴ�. 2008�� 9�� 8�� ���� ���� ���� POEM �ü� ����� ���������� �����ּ̽��ϴ�. ���� technique�� ���� ������ ����̾����ϴ�. �Դٰ� ���� ���� POEM �ü� ȯ�ڸ� 2017�� 5�� �ٽ� ���� �Բ� ���� ������ �ڶ������� �Ұ��ϼ̽��ϴ�. ���ϱ� ù �ü� 8�� �� �ٽ� �� ȯ�ڸ� ���� �ѵ����ϼ̴� ����Դϴ�. �� ���� ���ϴ� ȯ�ڰ� POEM �ü� �� 20kg�� �þ��ٰ� �����ߴٴ� ���Դϴ�. �� �η����ϱ�. ���� ����ϴٰ� �����մϴ�.
���� ���� POEM �ü� ���
���� ���� POEM �ü� ȯ���� �ü� �� �� ���� ��ȭ�� Eckerdt score
���� ���� POEM ȯ���� �ü� 8�� �� ���
![]() 11) [2017-6-17. ����������� motility symposium] New & Evolving techniques (����: �ָ���, ���ƿ�)
11) [2017-6-17. ����������� motility symposium] New & Evolving techniques (����: �ָ���, ���ƿ�)
1) Endoscopic treatment for esophageal motor disorders. Young Hoon Youn (Yonsei Univ)
(1)Heller myotomy: Open���ٴ� laparoscopic�� ����, thoracoscopic���� laparoscopic�� ����, full ���� partial�� �����ϴ�.
(2) POEM
- ESD�� �� general anesthesia, positive pressure ventilation, CO2 insufflator, IV antibiotics�� �ʿ��մϴ�.
- �����ϸ� deep tunneling�� �ؾ� �մϴ�. (1) ��¥�� myotomy�� �� ���̹Ƿ� �Ϻ� �ջ��� �Ǿ ����� �����ϴ�. (2) Muscle�� �β����� õ���� �� ������ �ʽ��ϴ�. (3) Mucosal flap�� ��ȣ�ϴ� ���� �ξ� �� �߿��ϱ� �����Դϴ�.(4) ������ ���� �ʱ� ���Ͽ� muscle fiber�� ���� �������� ������ ��ƾ� �ϱ� �����Դϴ�.
- POEM �� peristalsis�� ���ƿ��� ȯ�ڰ� �ֽ��ϴ�. Type III, ���� �Ⱓ�� 1�� ���Ϸ� ª���� ���� POEM �� peristalsis�� ���ƿ��� ��찡 �����ϴ�. (���ƿ� ������ comment: Type III���� ȣ���Ǿ� ���̴� ���� POEM�� ���Ͽ� ����� contractility�� �������Ƿ� ��ǰ�� �����鼭 ���� �ִ� peristalsis�� ȣ���Ǵ� ��ó�� ���̴� ���� �� �ֽ��ϴ�.)
- Non-achalasia���� POEM�� �� ��쿡�� ȯ�� selection�� �ξ� �����ؾ� �մϴ�. Diffuse esophageal spasm�� manometry �Ұ��� GERD������ �Ͻ������� ���� �� �����Ƿ� ���ܿ� �����ؾ� �մϴ�. Non-achalasia���� POEM�� �ϸ� LES pressure�� ������ �꿪���� �����Ͽ� ������ GERD ������ ��ȭ�� �� �ֽ��ϴ�.
- Spastic motility disease���� ice water�� ����Ͽ� contraction�� �����ϸ� ġ����� ������ ������ �� �� �ֽ��ϴ�.
[���ƿ� ����� comment] Dysphagia�� ���� non-achalasia spastic disease ȯ�ڿ��� circular muscle contraction�� �ֵ� ������ �����Դϴ�. IRP�� ���ٰ� POEM�� �ϸ� ������ ���� ���ϴ� ��찡 ���� �� �����Ƿ� �켱 PPI�� �Ἥ ���� ȣ�� ���θ� ���� ���� ���ڽ��ϴ�.
[������ ����] Non-achalasia spastic disorder���� body peristalsis�� �ϰ� LES myotomy�� ���� ������ ���� �� ������... body�� LES�� ����κ��� ��� ������ �� �ֽ��ϱ�?
[������ ������ �亯] Incisor�κ����� �Ÿ��� �Ǵ��� �� �ۿ� ������, ��Ȥ oblique�� muscle fiber�� ���̸� LES�� ������ �� ������ �Ǵ��� �� �ֽ��ϴ�.
![]() 12) �� 7ȸ NOTES �������� (2017-7-8)
12) �� 7ȸ NOTES �������� (2017-7-8)
(1) POEM for achalasia - �赵�� (����ƻ꺴��)
Learning curve
- Learning rate of 8-13 cases - �赵�� �����Բ����� 13��° POEM���� �� ���� Ȯ���� �ٸ��ٴ� ������ �Ҵٰ� �մϴ�.
- Learning curve plateaus around 16-20 cases
- Efficacy after 40 cases
- Mastery after 60 cases
�ü� 1-5�� ������ ���� ������ �ּ�ȭ�ϱ� ���� ���� ������ �ʿ��մϴ�. �ü� �Ϸ� ���� �Կ��ϴµ�, �ü� ���� ���ð� �˻縦 �����Ͽ� ���� ���� ���Ĺ� ���θ� Ȯ���ϰ� �ʿ��ϸ� ���� ���Ĺ��� �����ؾ� �մϴ�.
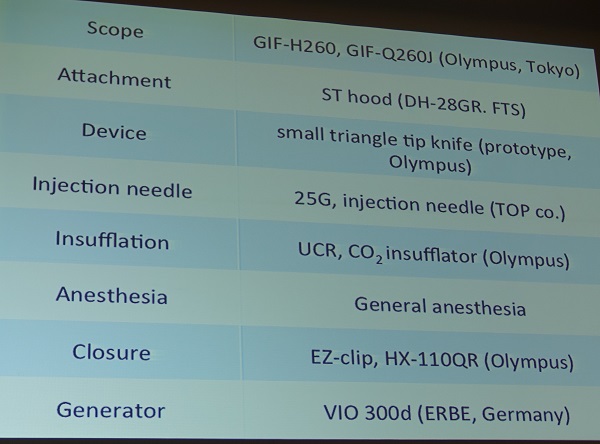
�ü� �غ� Anesthesia General / positive pressure ventilation Insufflation system UCR CO2 insullator Scope / attachment Water jet function / Transparent cap Generator VIO 300D (ERBE) Knife TT / IT / Hook / Hybrid Injector needle Injector catheter with needle or spray tip Injection fluid Normal saline glycerol, sodium hyarulonate, indigocarmine, epinephrine Closure Endoscopic clips
Nat Rev Gastroenterol Hepatol. 2015
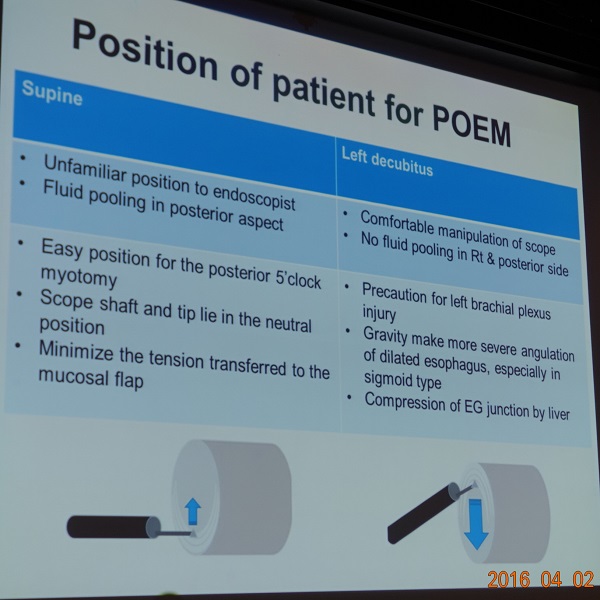
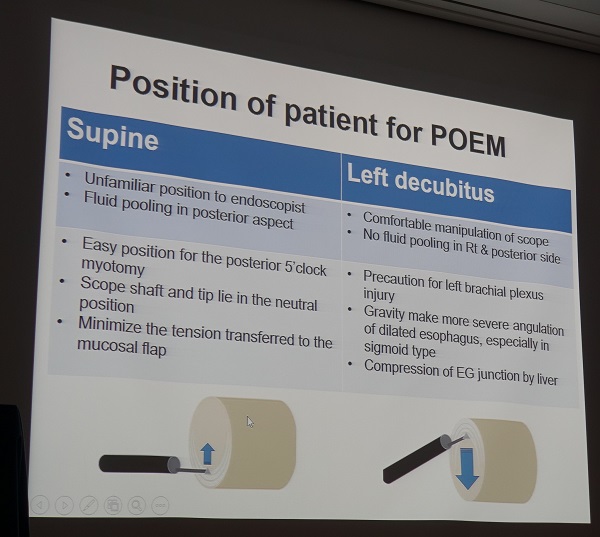
ȯ���� �ڼ� Supine Left decubitus ���ð� �ǻ翡�� �ͼ����� ����
�ĺ��� ��ü ����
Post. myotomy�� ����
Mucosal flap���� �ּ����� ��� �������ð� �ٷ�� ������
����, �ĺ��� ��ü ���� ����
Left brachial plexus �ջ� ���� ����
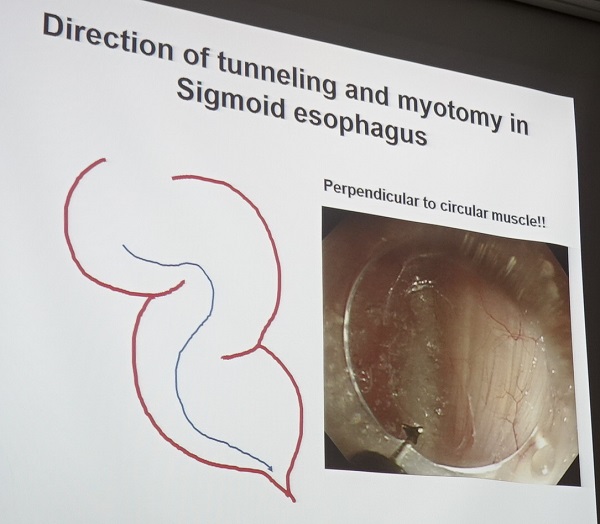
Sigmoid esophagus�� ��� �߷��� �� ���� ������ ����
���� ���� GEJ �й�
Submucosal tunneling ��ɰ� ������ Circular muscle fine fiber�� ���� ������ ����� ���� �Ѵ�.
Circular muscle fiber ������ ���� �������� �ͳθ��� �ؾ� �ϸ�, sigmoid esophagus�� ��� ���� ���ϴ�.
Achalasia ������ ���� �β���Ƿ� ���� õ���� �̳��� ����.
������ �ͳ� ����� ���� �ջ� ��������.
- Circular muscle�� ���� ������ ���� �ڸ��� �Ѵ�.
- ������ ���� ���ջ��� ����� ������ ��ġ�� ������, ���� �ջ��� õ���� �߱��Ѵ�.
- �ͳ��� ������ ������ ���� ������ �����ϰ� �Ѵ�.
������ �ͳ��� �������� �����ϸ�, ���� �е��� ������ �����Ͽ�, ū ������ ���ؼ��� ������ ������ �ϴ� Ư���� ���ǰ� �ʿ��ϴ�. �� �й��� ������ �� ��Ƽ� ���� õ���� ���輺�� ����.
Landmarks of EGJ ������ ������ ��������
������ ������ �ٲ�� (pallisade pattern → net-work pattern in gastric side)
���ð� ���� �� Ǫ�� ����
2���� ���� ��� �� �ͳ� ���� trasillumiation
Nat Rev Gastroenterol Hepatol. 2015
Myotomy ��ɰ� ������ Longitudinal fiver�� �ڸ��� �ʴ� �������� circular muscle myotomy�� �ϱ� ���ؼ��� inter-muscle space�� �����ϱ���� �ܰ������� �������� �����ؾ� �Ѵ�.
Standard myotomy �ѱ���: 10-12cm, including 2-3cm cardiomyotomy
Selective myotomy�� ��Ȯ�� �� �� ���� ���� ���ɽ����� full thickness myotomy�� �ܰ������� �����ϴ� ���� �ʿ��ϴ�. Incomplete cardiomyotomy�� ġ�� ���п� ���� ����� ���� ���� �����̱� �����̴�.
[2017-7-8. ������ ����]
POEM�� ������ ���õ� ���ð� �ǻ簡 �����ؾ� �ϴ� ����� ������ �����̴ּµ���, ESD�� ���� �������� �ʴ� ���� �ǻ���� ESD���� POEM�� �ξ� ���� �ü��̶�� ���ϰ� �ֽ��ϴ�. �������� ��� �����Ͻô�����?
[2017-7-8. �赵�� ������ �亯]
ESD ���������� �ſ� �����ϰ� ��쿡 POEM�� �����մϴ�. ���� ESD ������ ���ų� ���� ���� Ȥ�� �ε� �ǻ���� POEM�� ������ ����� ������ �մϴ�. Myotomy�� selective�ϰ� ���� �ʰ� �밭 TT knife�� �� �ڸ��� �ֽ��ϴ�.
�ĵ� ESD�� POEM�� ��ȣ �������� �ü��Դϴ�. POEM�� �����Կ� �־� �ĵ� ESD ������ ũ�� ������ �Ǿ����ϴ�. �ĵ� ESD�� �����Կ� �־� POEM�� ���Ͽ� �˰� �� �Ϻ� ������ ���� ���ذ� ������ �Ǿ����ϴ�. �ĵ� ESD�� POEM�� ��� �����ϸ鼭 ���� �Ʒ��� ��� �˰ԵǾ��ٴ� ������ ���ҽ��ϴ�.
![]() (2) POEM for treatment of other esophageal motility disorders - ���� (��õ���б� �溴��)
(2) POEM for treatment of other esophageal motility disorders - ���� (��õ���б� �溴��)
Achalasia�� subtype�� ���� ġ���ħ�� ���� �� �ֽ��ϴ�.
Digestion 2017;95:29 - PDF 0.5M
Spastic or hypercontractile esophagus�� ���� POEM�� �־ LES myotomy�� �ؾ��ϴ°� ������ �ֽ��ϴ�. Inoue �������� ���� achalasia�� ������ �� �ְ�, POEM ���� �ĵ� ü���� ineffective peristalsis�� ���� dysphagia�� regurgitation�� �����ϹǷ� �̸� LES myotomy�� �ϴ� ���� ���ڴٴ� �ǰ��� �� ���� �ֽ��ϴ�).
[2017-7-8. ������ ����]
2017�� Digestion���� �Ǹ� ����(Digestion 2017;95:29-35)�� �ο��Ͻø鼭, achalasia �� type II�� ���ؼ��� balloon dilatation�� first choice�� �����̴ּµ���, ���� ������ learning curve�� ����� ����� ��� POEM�� �������� ȿ���� ������ �� ��� achalasia�� first choice�� POEM�� ��õ�ϴ� �������� ���� ������ �˰� �ֽ��ϴ�.
[2017-7-8. ���� ������ �亯]
Balloon dilatation�� POEM�� randomized study�� ������ ��������, POEM�� �����ϴ� ��������� POEM����, balloon dilatation�� �����ϴ� ����� balloon dilatation���� �����ϰ� �ִ� ��Ȳ�Դϴ�. ���� ��κ� POEM���� ġ���ϰ� �ֽ��ϴ�.
[2017-7-8. ������ comment]
POEM ���Ⱑ Ȯ���Ǿ��� ������, ����μ��� Ư���� ��� �ƴϸ� type�� �����ϰ� ��� achalasia ġ���� primary choice�� POEM�� �����ϴ� ���� Ÿ���� �� �����ϴ�.
![]() (3) Complications of POEM - ������ (������б� �ǰ�����)
(3) Complications of POEM - ������ (������б� �ǰ�����)
��� (WHO-UMC causality categories) Definite (certain) No other cause Probable Other cause unlikely Possible Other causes possible Unlikely Other causes more likely
Gas-related complications Spontaneous empyema 31.6% Capno/pneumomediastinum 10-22% Capno/pneumothrax 11% Capno/pneumothrax requiring decompression 2.7% Capno/pneumoperitoneum 30.6% Capno/pneumoperitoneum requiring decompression 8.0%
Mucosal injury-perforation (mediastinal or peritoneal leak) (major) = 0.3% Mediastinitis Insufficient data Peritonitis Insufficient data Retroperitoneal abscesses 2 cases reported Pleural effusion Insufficient data Pneumonitis Insufficient data GI fistula Insufficient data Fever Insufficient data
Rare complications Delayed postoperative bleeding 1.1% Hematoma within the tunnel Submucosal infection Mortality 0.025%(1/4000) ������� POEM�� ���õ� ����� 1���� �����Ǿ� �ֽ��ϴ�.
������ �����Բ����� POEM �� ���� reflux ������ ȣ���� ȯ�ڸ� �Ұ��Ͽ� �ּ̽��ϴ�. POEM �������� full thickness myotomy�� �Ǿ��� ȯ���ε� PPI response�� �������ϴ�. ���ð濡�� pyloric ring contraction�� ���ӵ� ����̾��� gastric emptying study���� delayed emptying�� �������ϴ�. Full thickness myotomy�� ���õ� vagus nerve damage�� �ǽ��Ͽ� pyloric ring �ֺ��� Botox injection�� �Ͽ��� ��� ������ ȣ���Ǿ����ϴ�.
![]() 13) Live demonstration
13) Live demonstration
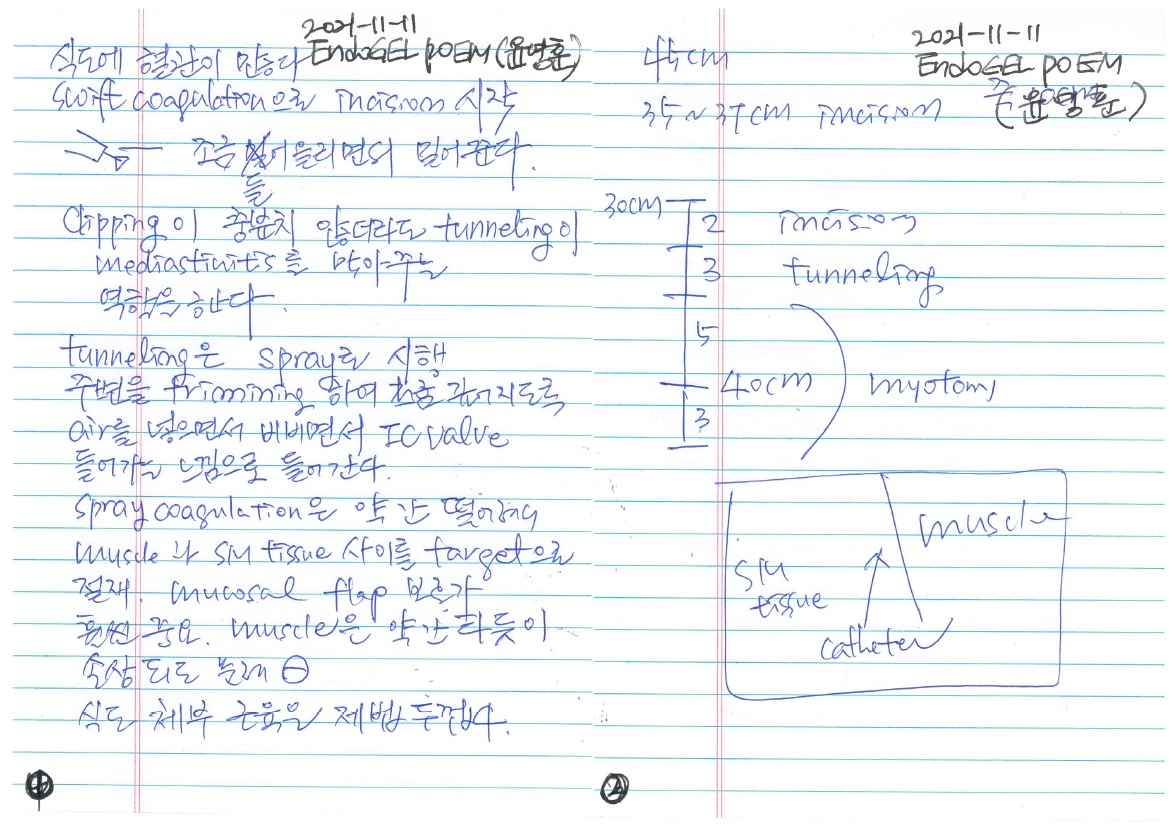
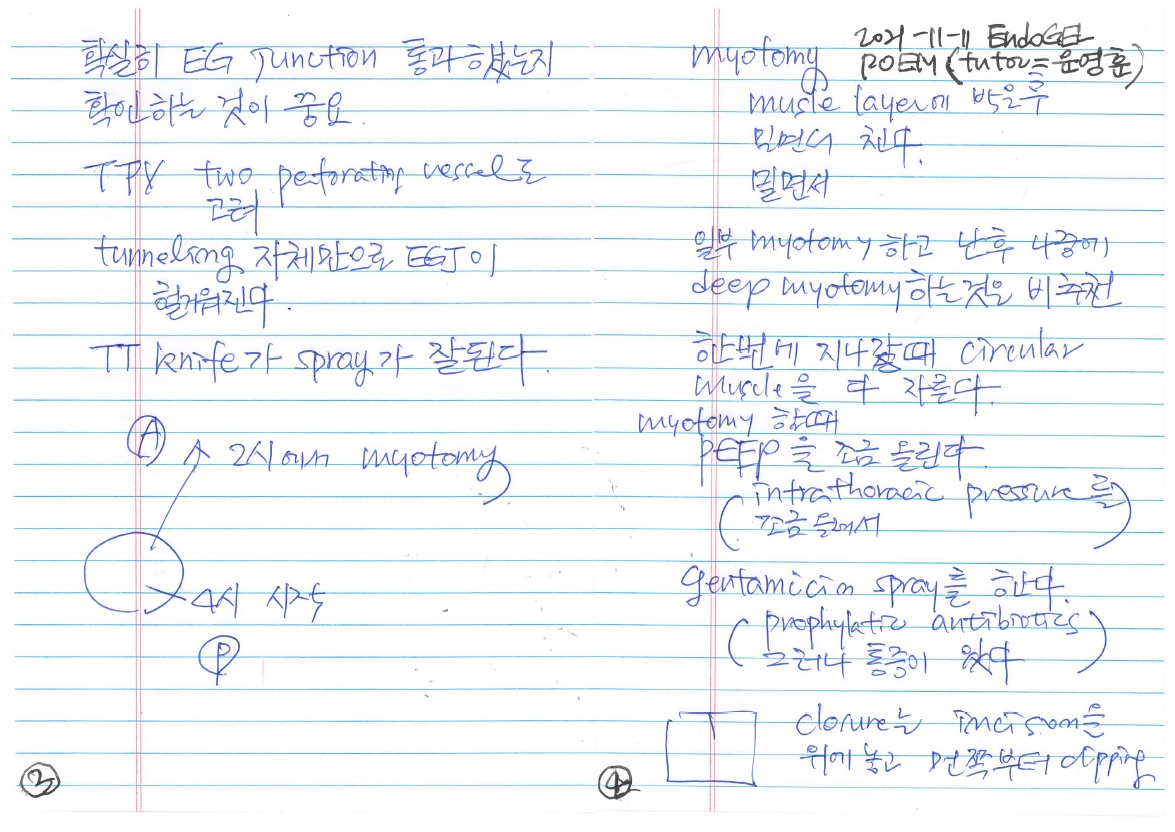
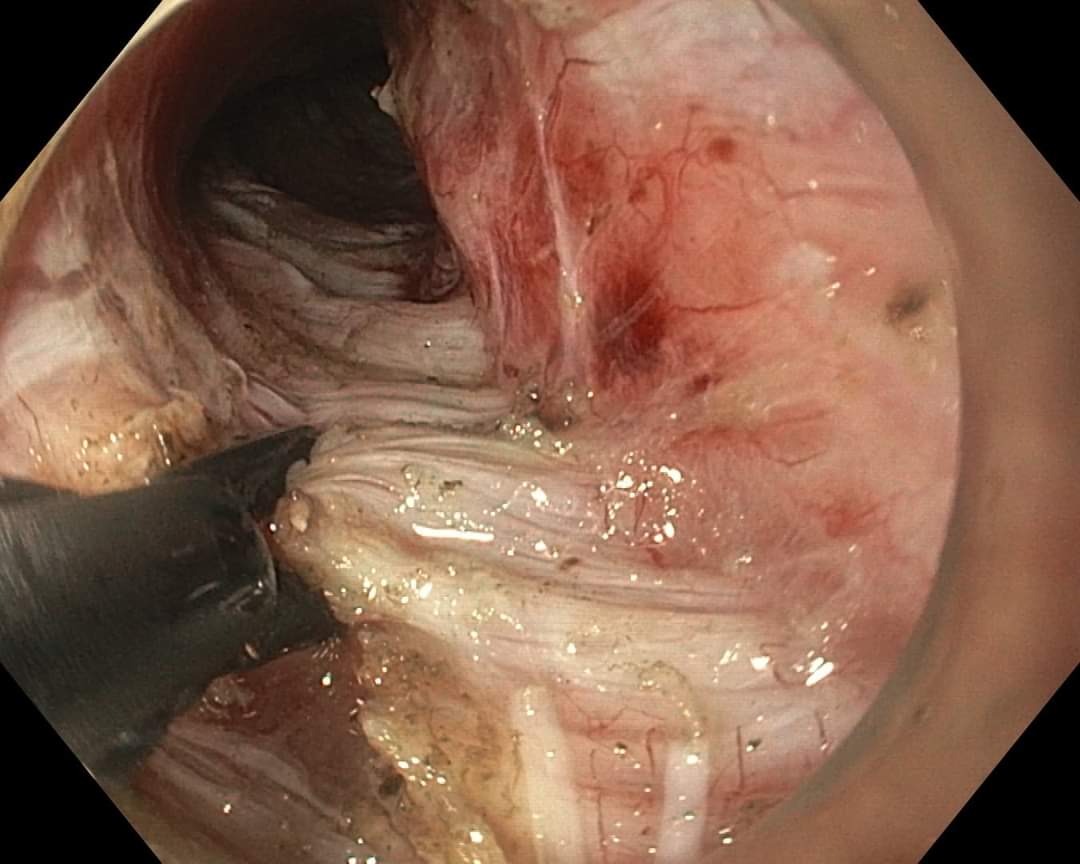
���ֿ�: Supine position���� �ü��ϰ� �ֽ��ϴ�. (Left decubitus�� 3�ð� �̻� �ü��ϴٺ��� palsy�� �� �� �ֱ� �����Դϴ�) Normal salin 100cc�� hyaluronic acid 1 ampule�� ��� ����ϴµ�, hyaluronic acid �� ���ϸ� ���Ⱑ ���� ���� ������ �ֽ��ϴ�. Blue dye�� ���ϰ� ���� perforating vessel�� �� ���̱� ������ dye�� ���ϰ� ����ϰ� �ֽ��ϴ�. Dual knife�� �̿��Ͽ� spray coagulation mode, effect 2, 40 watt�� ����մϴ�. Spray mode�� non-contact ����̹Ƿ� Dual knife�� needle�� ������ ������ �ʰ� submucosal dissection �� �� �ֽ��ϴ�. Pneumoperitoneum�� ���ϸ� ȯ���� ���°� �� �������� ������ angiocath�� �̿��Ͽ� ������ gas�� �����ϰ� �ֽ��ϴ�. Pneumomediastinum���� ��Ȥ tension pneumothorax�� ���Ͽ� ���� chest tube�� �ؾ� �ϴ� ��찡 �ֽ��ϴ�. Diaphragm level���� (��Ȥ ���� achalasia���� stenosis�� �ִ� ����) ������ ���� �����ϱ� ������ ���ð� ������ ����� �� �ֽ��ϴ�. (1) cap�� ���� �ü��ϰų�, (2) �κ����� myotomy�� ���� ������ �ִ� ����� �� �� �ֽ��ϴ�. Cardia�� ���� submucosal tissue�� loose�����µ�, �̶����ʹ� ������ �� ���� pre-emptive coagulation�� �ϴ� ���� �����ϴ�. �Ϻ� �Ļ������� POEM �ü��Ḧ 15���� ������ ������ �����Դϴ�. ���������� ȯ�ڰ� ���� ����� �Ѿ� 400-500���� ���� ���� �� �����ϴ�. (�ٸ� �����Ե��� �ü��� 200-350���� ������� �����ϼ���) �Ϻ������� �Ļ������� POEM �ü��Ḧ 15���� ������ ���س��Ҵٰ� �մϴ�. ���������� Myotomy�� FineMedix ���� hook knife, Swift coagulation���� �ü��Ͽ����ϴ� (FineMedix ���� hook knife�� �� �����ϴٰ� �մϴ�). �ĵ��� selective myotomy�� �ϴ��� longitudinal muscle�� �Բ� �����Ǵ� ��찡 �����ϴ�. EG junction �κ��� ���������� full thickness myotomy�� �ϱ �մϴ�. Type I�� ��� circumferential muscle�� ���� ��� ������ ������ full thickness myotomy�� �DZ �մϴ�. Tunneling�� õõ�� myotomy�� ���� ������ �����ϰ� �ֽ��ϴ�. ���⸦ ���� �ְ� ���� �ӵ��� myotomy�� �ؾ߸� pneumomediastinum, pneumoperitoneum�� ������ ����, Ȥ�� ���ϴ��� ���Ⱑ ���� �� ȯ�ڰ� ���� ȸ���˴ϴ�. ���ֿ� �������� POEM �� reflux�� ���Ͽ� 2������ antireflux endoscopic treatment�� �Ͽ��ٰ� �����ϼ̽��ϴϴ�. POEM �ʱ incision�� horizontal�� ������ ����Ͽ��µ� ���� closure�� ������ٰ� �մϴ�. ������ �� longitudinal�ϰ� incision�� �ϱ� �빮�� clipping�� ����� ���� ���� ���� �� �����ϴ�.
ȫ����: �ü� �ð��� ������� edema�� �������� �� �ü��� �Ҹ��� ���� ���� ���� �� �ֽ��ϴ�. Muscle�� ������ tunelling�� �Ǿ�� ������ �� ������ �ǰ�, preemtive coagulation�� �� ������ ���� �������� �����ؼ� �����Ͽ��� mucosal thermal injury�� ���� �� �ֽ��ϴ�. Intraoperative EndoFlip�� routine���� �ϰ� �ֽ��ϴ�. Myotomy�� �����ϰų� �������� �ʾҴ��� ���� �� �ֱ� �����Դϴ�.
����: submucosal tunneling�� �� ������ muscle�� ������ �����Ͽ� �ü��ϴ� ���� �����ϴ�. ������ preemptive coagulation�� �� �������� ������ ������ thermal injury�� ���� �� �ֽ��ϴ�. Body������ selective myotomy�� �ϴµ� full myotomy�� ���� �ʵ��� �ణ superficial�ϰ� �����ϰ� EG junction ���������� circumferential muscle myotomy�� �� �� ���� longitudinal muscle�� ���� ��� ������ ������ full myotomy�� �˴ϴ�. Incision�� closure �� �� �� ù clip�� �� ����ֿ��� �մϴ�.
������: TT knife, Spray coagulation, effect 2, 60 watt�� ����ϰ� �ֽ��ϴ�. Spray coagulation�� non-contact ����̸�, ǥ������ �������� ȿ�����̹Ƿ� TT knife�� �����մϴ�. �ƻ꺴�� �赵�� �������� IT nano�� ����ϰ� �ִµ�, ���� tip�� �־� ���� ������ ������ �� �����Ƿ� ���� ������ ������ �� �ֽ��ϴ�.
[������ comment]
Achalasia�� ������ȯ�̰� ������ �ټ� ��ȣ�Ͽ� �ǽ����� ������ �����ϱ� ��ƽ��ϴ�. �����ִ� ȯ�ڰ� �ֽ��ϴ�. ���� �м����� ���� ���Ͽ� achalasia�� ���� �������� �������鼭 ���� ���� achalasia ȯ�ڰ� �߰ߵǰ� �ֽ��ϴ�. ������ ���� incidence�� ���� ���̹Ƿ� ����ó�� ȯ�� ���� ���� ���� ���� �ƴմϴ�. �Դٰ� POEM ���� ���Ͽ� ȿ�������� ġ��� �� �����Ƿ� ��ġ�� �����մϴ�.
�Ϻ������� achalasia ���ʰ� ���� �߰ߵǰ� POEM���� ġ��� �� �ֱٵ�� ���� ���ܵǴ� ���ʰ� �����ϰ� �ִٰ� �մϴ�. �ų� ���� ���ϴ� achalasia�� ���� �ʱ� ������ �����ִ� ȯ�ڵ��� �߱��Ͽ� ��� ġ���ϸ� ��ȯ�� �پ�� �� �ۿ� ���� �����Դϴ�.
POEM�� ���� ������ �ü��̹Ƿ� learning curve �̽��� ������, �Ƿ��� �����ϱ� ���ؼ��� �ų� ���� �� �̻��� �ü��� �ؾ� �Ѵٴ� ���� �����Ǿ�� �� ���Դϴ�. �츮���� achalasia ȯ�ڰ� �����Ƿ� POEM �ü��ڵ� �� ���̸� ����մϴ�. ġ��ð濡 �����ִ� �ǻ簡 ���� �������� �Ҽ��� POEM�� �ü��ϴ� ���� ���� ���� �ƴմϴ�. ��� center�� �����ϴ� ���� �ʿ��մϴ�. ū ������ �ʿ�� �����ϴ�. ���� �����̶� POEM �ü��� ���ɸ��� �ü��ڰ� ȯ�ڸ� ��Ƽ� ���� center�� ����� �˴ϴ�. �ϳ �ѵθ� �ü��� ���̸� �ƿ� �������� �ʴ� ���� ���ڴ��� ���� �� �ǰ��Դϴ�. ���� ���� POEM �ü��� ���� �ʰ� �ֽ��ϴ�. �� ���������� �ξ�� �������� ��� �ü��� �ϰ� ��ʴϴ�.
[�̱��� ������ private comment]
������ ������ �ǰ��� Ÿ���ϴٰ� �����մϴ�. ȯ�ڵ� ���� ������ ��� center�� �����ϴ� ���� ���ڽ��ϴ�. ���� ��� achalasia ȯ�ڸ� �Ƿ��� �ʿ䰡 ���� �� ������ �ʽ��ϴ�. ���� ������ ���ǿ��� �Ұ��� Digestion�� ����(Digestion 2017;95:29-35)�� ���� type II�� ���� ������ balloon dilatation���� ġ���ϰ�, POEM�� �� �ʿ��� ȯ�ڸ� POEM center�� �Ƿ��ϴ� ������ ������ �� �����ϴ�.
![]() 14) 2018-5-10. �Ϻ����ð���ȸ Inoue ������ ����
14) 2018-5-10. �Ϻ����ð���ȸ Inoue ������ ����
Showa ���п����� 2008�� 9�� 8�� ù �ü� �� 2018�� 2�� 15�ϱ��� 1621���� �ü��� �ߴٰ� �մϴ�.
�۳� IDEN���� �����־� ū ������ �־��� �� ������ �ٽ� �����־����ϴ�.
2008�� 9�� 8�Ϻ��� 2017����� �Ϻ����� POEM�� 2,998�� �ü��Ǿ����ϴ�. Major center�� Showa ���� (1515��, 50.5%), Fukuoka ���� (249��), Kobe ���� (182��), Nagasaki ���� (139��)�����ϴ�.
Inoue �������� double scope method�� �̿��Ͽ� LES�� distal margin�� Ȯ�������ν� incomplete mytomy�� ���ϴ� ����� �ڼ��� �����Ͽ����ϴ�.
���ð� fundoplication ����� �Ұ��Ǿ����ϴ�. �̸��� POEF (anterior partial fundoplication)���µ� ���ð����� peritoneal space�� �� �� clip�� endoloop�� �̿��Ͽ� anterior partial wrap�� ����� ����̾����ϴ�. POEM�� �ϸ鼭 POEF�� ���ÿ� ����(POEM + Fundoplication)�ϸ� �ü� �� ������ ���ٰ� �մϴ�. DeMeester score�� �־ ����� ���Ǽ��� ���� �� �ִٰ� �մϴ�. POEM�� �Ͽ� ��â ������ �� endoscopic fundoplication�� �Ͽ� �ణ �����ָ� ������ ���ٴ� ���ε�... �����ڸ� ���ְ� ���ְ��ε�... �̷��Ա��� �� �ʿ䰡 ������ �;����ϴ�.
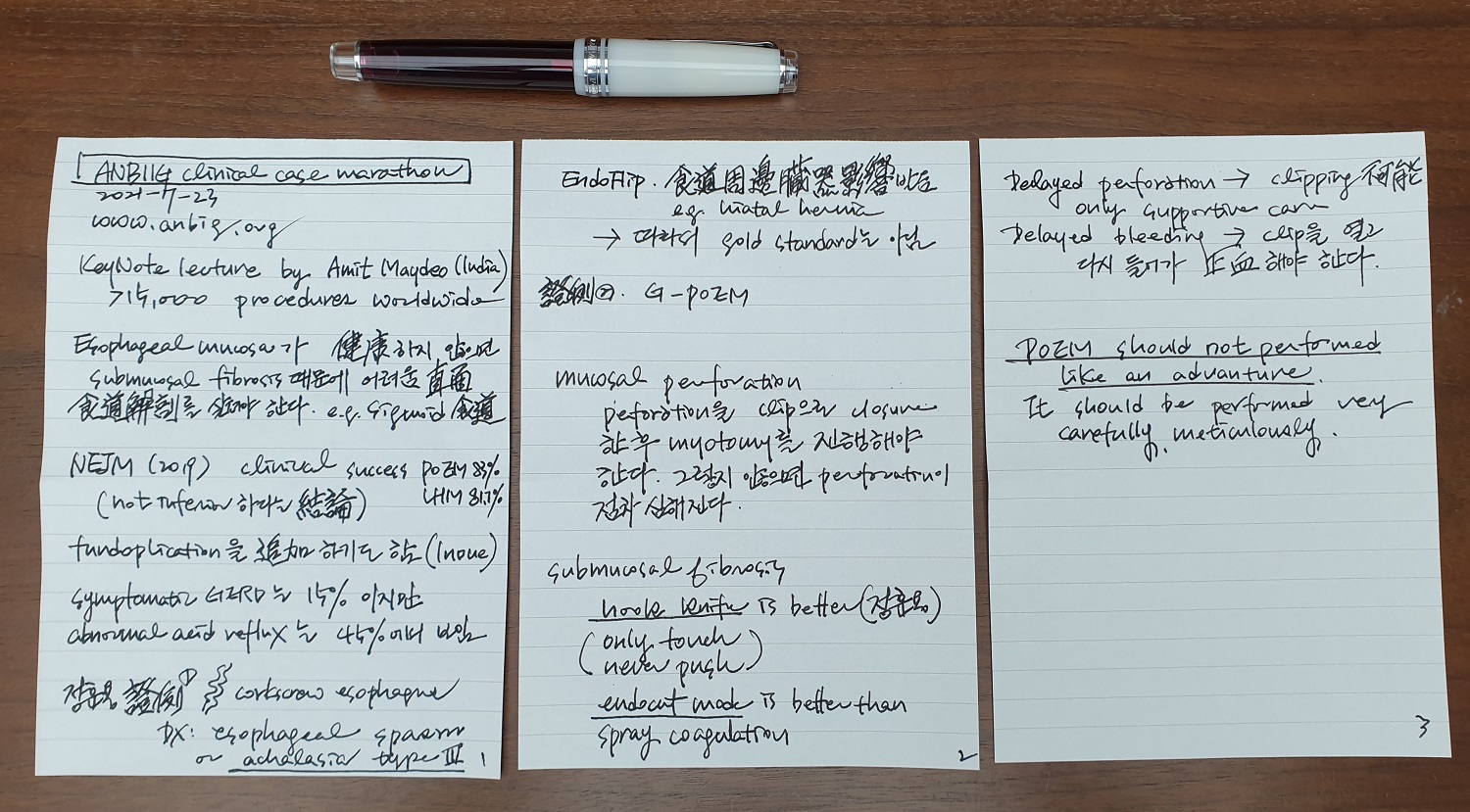
15) 2021-7-23. ANBIIG sympoisum for POEM
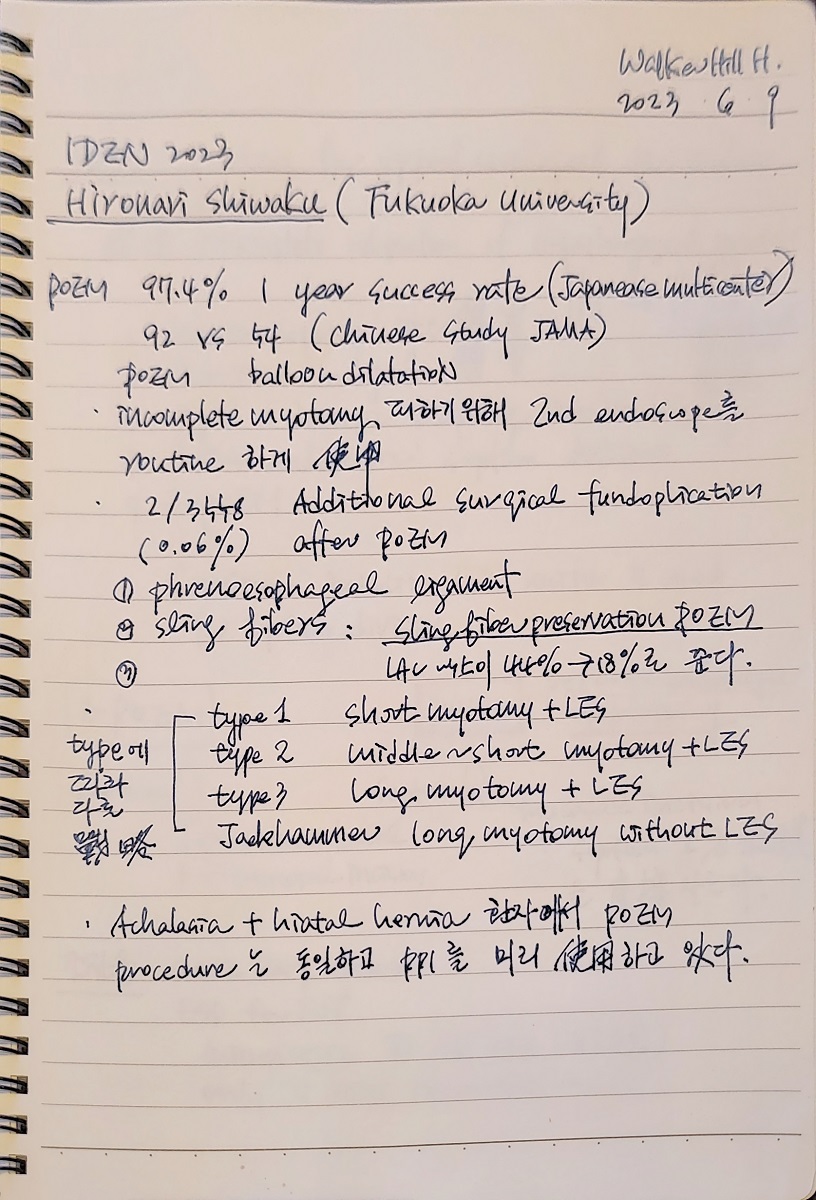
16) 2023-6-9. IDEN 2023
17) 2024-11-14. KDDW. ��ȿ�� ������ ����.
KSGE Log-in �
![]() 6. POEM training
6. POEM training
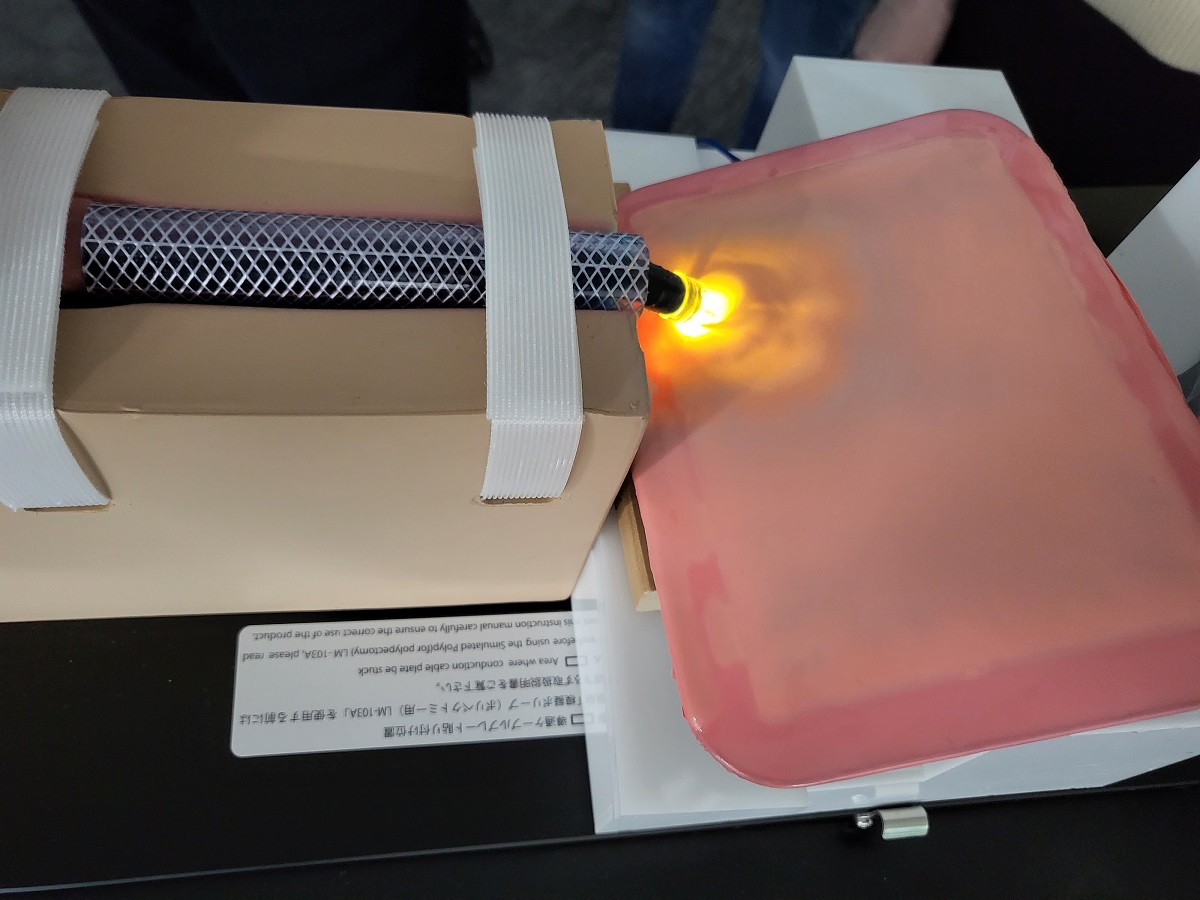
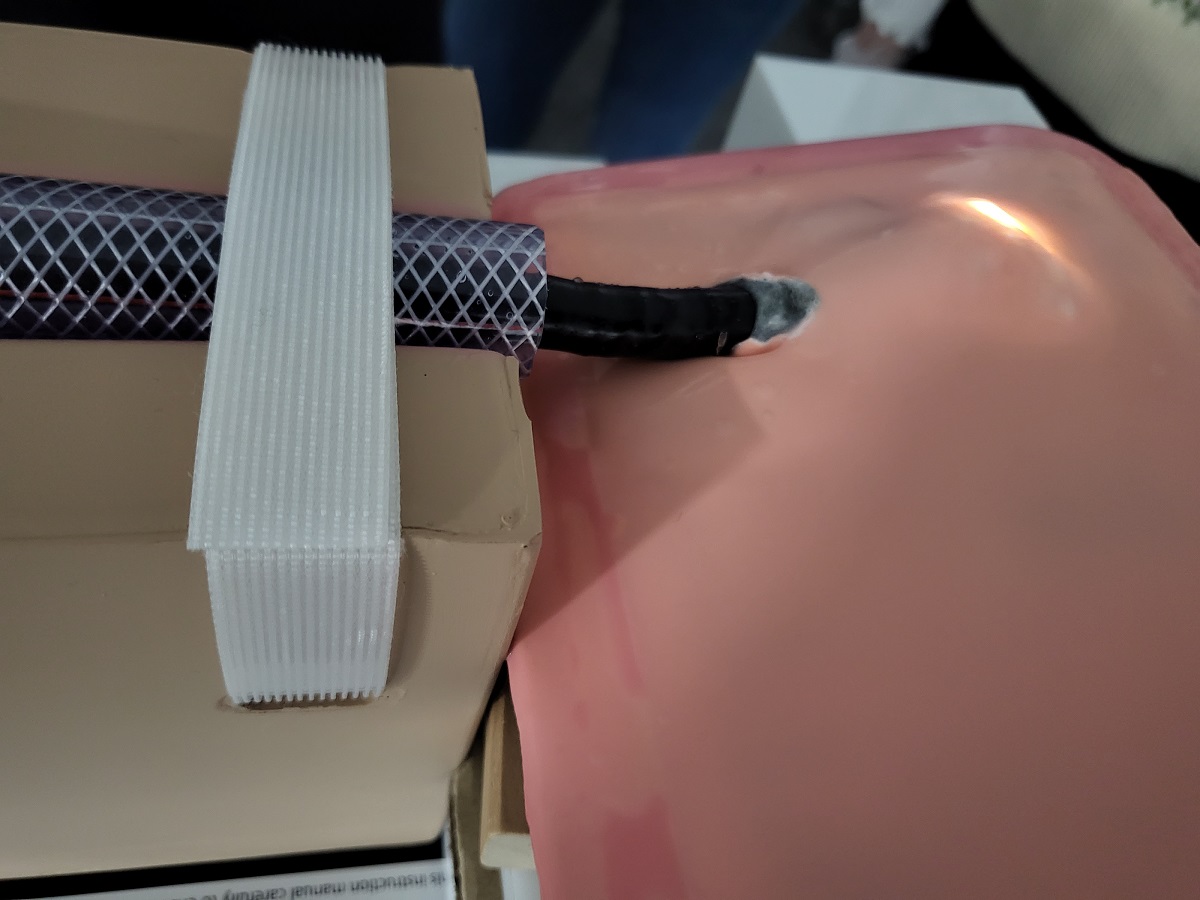
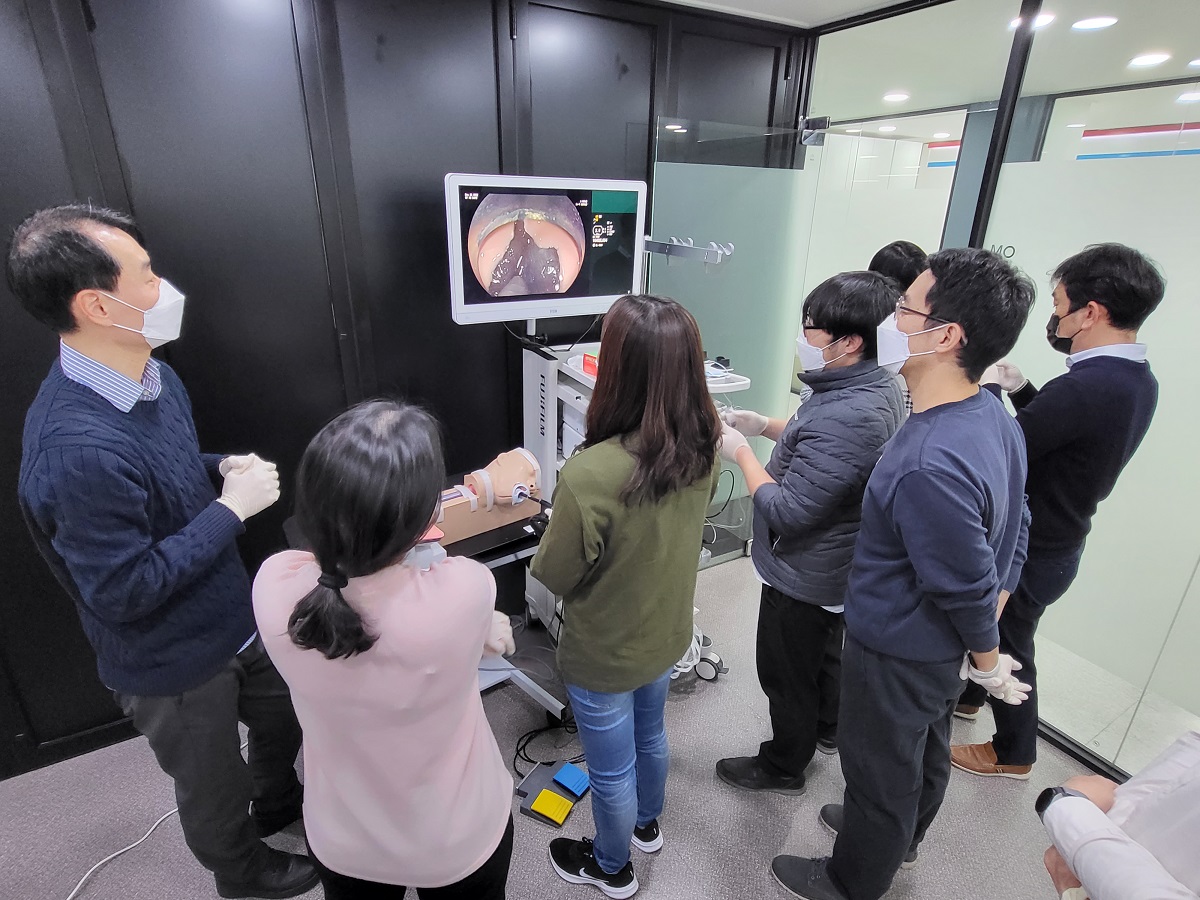
���ο� �ü��� ���� ���ؼ��� �ϴ� �������� �ü��� �����ϰ� simulator�� �̿��Ͽ� �Ʒ��ϸ� �����ϴ�. 2019�� Tokyo Live Inoue ������ POEM live�� ��õ�մϴ�.
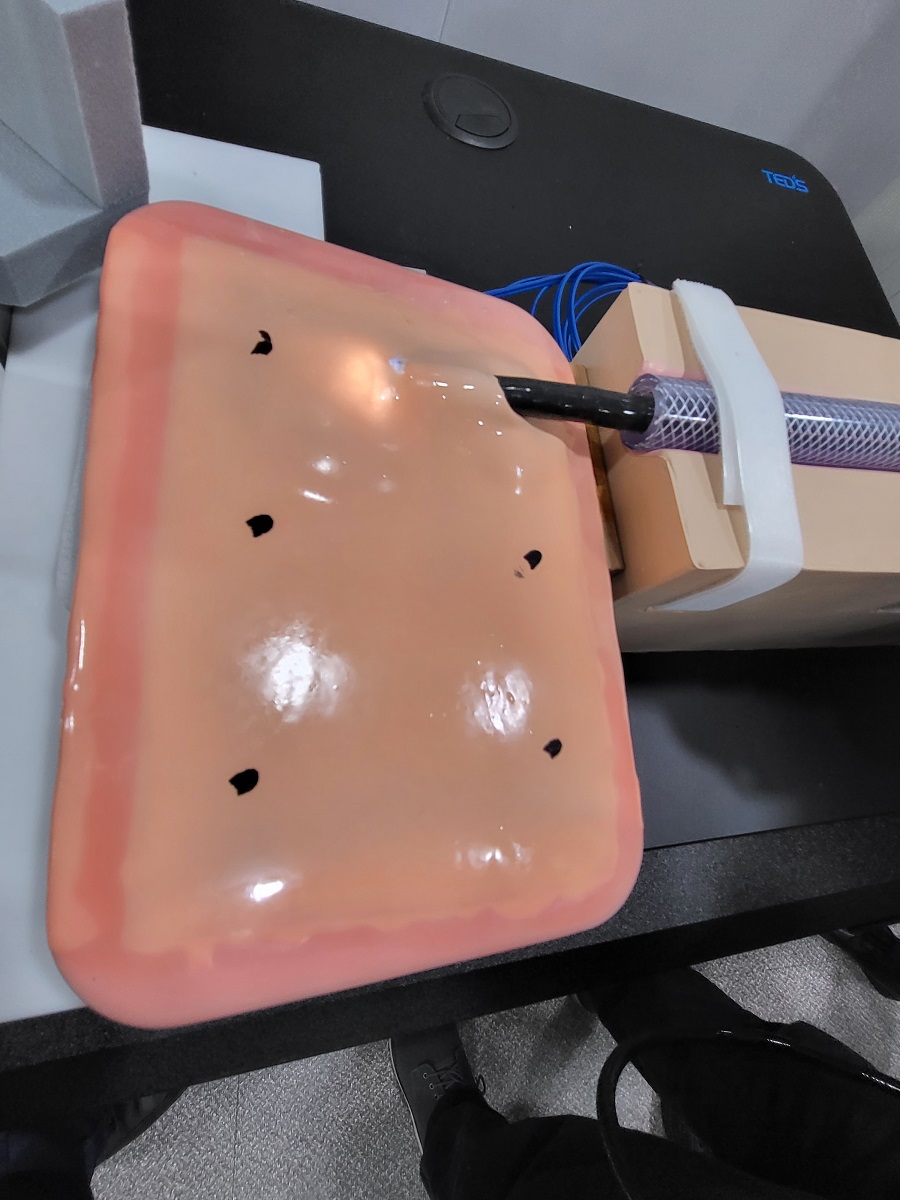
EndoGEL�� �̿��� POEM ������ �����մϴ�. �Ʒ��� EndoGEL ȸ�翡�� ������ �������Դϴ�.
YouTUBE ������
Myotoma ���� ����
2021�� 6�� 22�� �ξ�� �������� ��ð� �츮���� ���ʷ� EndoGEL POEM hands-on workshop�� �����Ͽ����ϴ�. EndoGEL ESD�� ����� �غ� �Ͽ��� �߰��� �ʿ��� ���� (1) ���ð� ���� ���� ������ ���� air/water bottle, (2) ����ĸ, (3) injection catheter, (4) saline �̾����ϴ�.
ȸ�翡���� EndoGEL�� �������� ��ġ��Ų ���¿��� ������ ���� ���ϰ� �ֽ��ϴ�. Anterior approach�� �������ϴ�.
�츮�� Koken simulator�� EndoGEL ESD training station�� ��ġ�ϰ� plate�� ������ ���� ���� �ٴڿ� ���� �ü��߽��ϴ�. Posterior approach�� �������ϴ�.
EndoGEL ESD�� �� ���� ������ �ʿ��մϴ�. ���� ���ð� system�� air/water bottle�� ��ġ�Ͽ����ϴ�.
���� cap�� �ʿ��մϴ�. Finemedix���� �ߺ�ǰ�� ����Ͽ����ϴ�.
ª�� ���� Olympus���� POEM ���� injection�� ����Ͽ����ϴ�.
Triangle tip�� ���� ���ð� water jet ����� ������ Olympus���� POEM ���� TT knife�� ����Ͽ����ϴ�.
ERBE ESU setting�Դϴ�. Endo Cut Q�� initial cutting���� ����ϰ� �ٸ� ��� step�� Spray Coag�� �̿��Ͽ����ϴ�. Myotomy �ܰ迡���� ����� ���� �������ϴ�.
�ξ�� �����Բ��� submucosal injection �� ù incision�� ���ϴ� �������� �����Դϴ�. �� ���� ���� �غ� �� ������ �������ϴ�.
Mucosal cutting
Incision �� tunneling�� ���Ͽ� ó������ ���������� �����ϴ� ����Դϴ�. �� �������� ���� ������ �ʿ��߽��ϴ�.
Intial submucosal layer introduction
Tunneling�� �ణ ����Ǿ����ϴ�.
Short tuneling
Tunneling�� ������ ����Ǿ����ϴ�.
Long tuneling
Initial myotomy
Short myotomy
Long myotomy
��� �ü��� ��ġ�� clipping�� �Ͽ����ϴ�.
Closure
�ξ�� �������� demonstration �ü��� ���� �� fellow �����Ե��� �ü��� �־����ϴ�. ������ ������ �������ֽ� �ξ�� �����Բ� ����帳�ϴ�.
EndoGEL POEM hands-on�� ��ġ�� �ξ�� ������ ���ͺ�
[2021-11-11] ��2ȸ EndoGEL POEM hands-on workshop
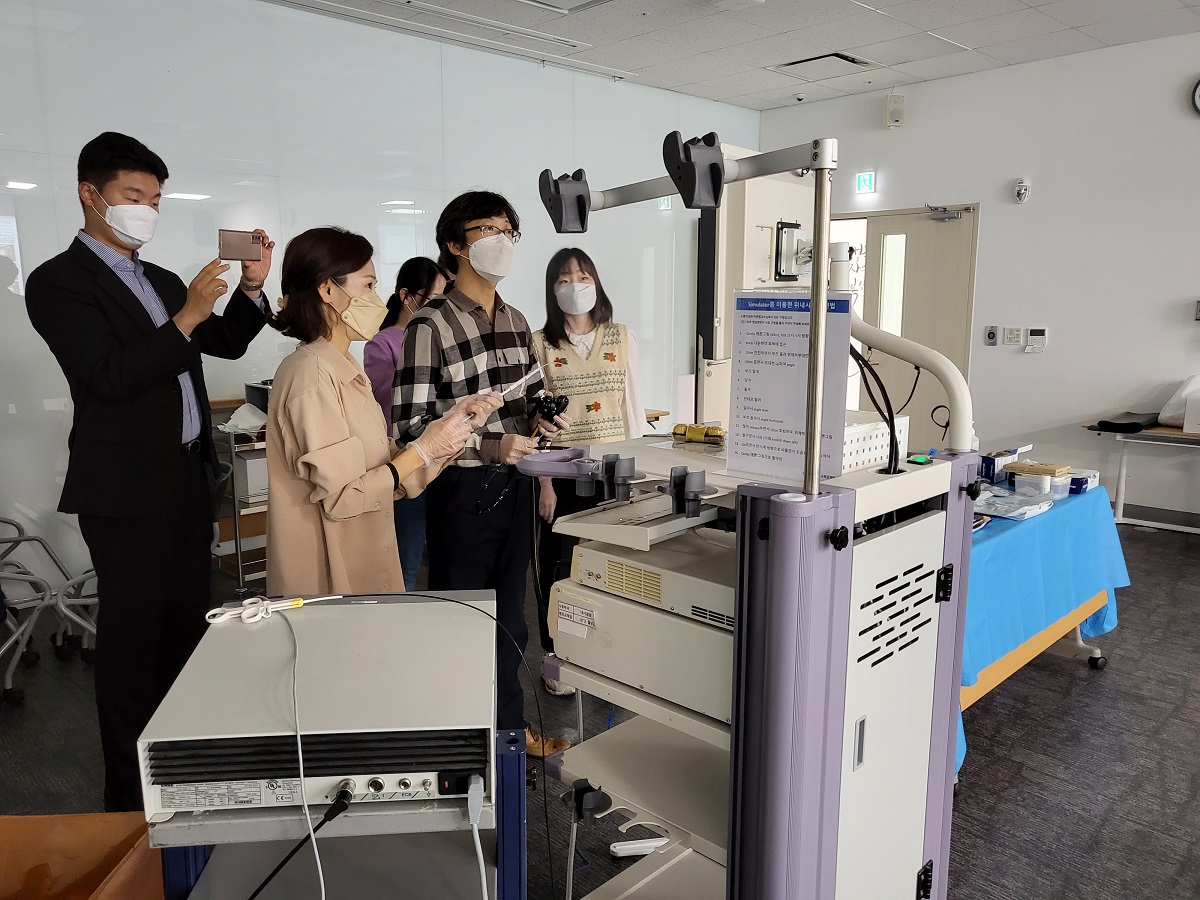
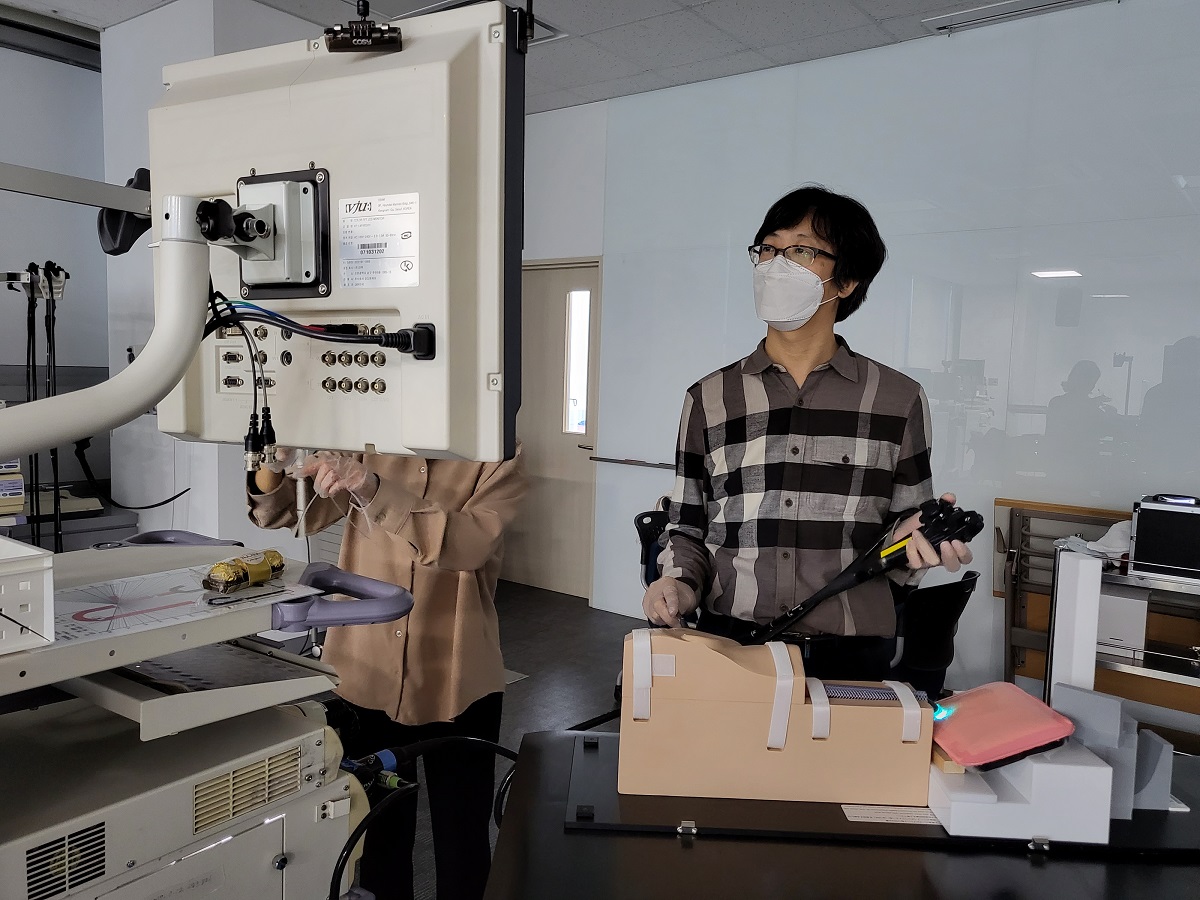
�Z�� COEX �α� Fujifilm ���ð� �Ʒýǿ��� �������б� ��������������� ������ �������� tutor�� ��ð� �Z���ﺴ���� ��������������� 2���� fellow �����Ե��� ������� ��2ȸ EndoGEL POEM�� �����Ͽ����ϴ�. ���� ȯ���� POEM�� ����� ����� ������ simulation�ϴ� ���� ���̶�� �����մϴ�. �ĵ��� ��Ƽ� POEM ������ ����� live pig ��� POEM �������ٴ� �ξ� �� ���Ҵٴ� �����̾����ϴ�. �����ε� ���������� EndoGEL POEM hands-on training�� ������ �����Դϴ�. ù ������ click�Ͽ� �������� ���ñ� �ٶ��ϴ�.
[2021-12-11] ��3ȸ EndoGEL POEM hands-on workshop
�Ͽ��� �Z�������� 9�� SMC �ӻ�ùķ��̼Ǽ��Ϳ��� �Z���ﺴ�� ��ȭ�⳻�� ���� �������� tutor�� ��ð� �Z���ﺴ�� fellow �����Ե��� ������� ��3ȸ EndoGEL POEM hands-on workshop�� �����Ͽ����ϴ�. ���ݱ����� �ӻ�ùķ��̼Ǽ��� �̿��� ��ҿ��� EndoGEL ESD workshop�� �����Ͽ����� �̹��� ó������ �ӻ�ùķ��̼Ǽ����� ���α��� ������ ���Դϴ�. �� ���α��� �ʿ��� ���� ���� ���Ǹ� ������ �ֽ� SMC �ӻ�ùķ��̼� ���� �����п��� �������� ������ ������ �帳�ϴ�. ������ʹ� �Ͽ��� SMC �ӻ�ùķ��̼Ǽ��Ϳ��� ���������� EndoGEL POEM hands-on workshop�� ������ �����Դϴ�.
������ ��翡�� Olympus �������� �����Ͽ����ϴ�. ���� Olympus �۵� training center K-TEC������ EndoGEL POEM hands-on woskrhop�� ������ �� �ִٰ� �մϴ�.
* EndoGEL POEM ����� ���� ��� ���� (�������簳�߽� �������, PDF)
[2022-5-28] ��4ȸ EndoGEL POEM hands-on workshop
�Ͽ��� �Z�������� 9�� SMC �ӻ�ùķ��̼Ǽ��Ϳ��� �Z���ﺴ�� ��ȭ�⳻�� ���� �������� tutor�� ��ð� POEM workshop�� �����Ͽ����ϴ�. �ſ� ���� feedback�� �ҽ��ϴ�. ��� �����ϼ̽��ϴ�.
[2022-11-5] ��5ȸ EndoGEL POEM hands-on workshop
�Ͽ��� �Z�������� 9�� SMC �ӻ�ùķ��̼Ǽ��Ϳ��� �Z���ﺴ�� ��ȭ�⳻�� �ξ�� �������� tutor�� ��ð� POEM workshop�� �����Ͽ����ϴ�.
[2025-11-5] ��8ȸ EndoGEL POEM hands-on workshop
�ξ�� �����Բ��� 8��° EndoGEL POEM hands-on workshop�� �� ������ �ּ̽��ϴ�. �����մϴ�. �۳ air ���� �����Ͽ� ��ô ������µ� �ݹ����� �� �Ǿ��ٰ� �ϴ� �����Դϴ�.
�� �п��� feedback�� �ҽ��ϴ�.
[P] �� ������δ� �۳�� submucosal tunneling �� �þ� Ȯ���� �� �ȵ� ������ ���Ǵµ�, �̹����� ���ð� �۱� ����� �۵��Ǿ� �þ� Ȯ���� �Ǿ��� suction�� ���� �۵��Ͽ����ϴ�. ESU �� �� �۵��߽��ϴ�. ����¿� �ռ� �� ���� �� �ξ�� ������ �ü��� �����ߴ� ���� �ִµ�, �̹� ����¿��� �������� �ü������� ���� ���ص��� ������ �� �����ϴ�.
[K] �����θ� ���ٰ� �ѹ� �غ��ϱ� ������ �� ������, Endogel�� ���ʹ� �ٸ��� �ĵ� �ü��� �������� �ǹ��̿��µ� ���� ������ ���� �ʾҰ� �ξ�� �������� ������ �� �ҽ��ϴ�. �����Բ��� �������� POEM �ü��� ���� �ѹ��̶� �� ���� ��õ�Ͽ� ������ �����ϰ��� �մϴ�.
[B] �۳�� ���Ͽ� ���� ������ ��Ȱ�ؼ� �۳⺸�� �� ����Ǿ��� ������ �Ǿ��ٰ� ������ϴ�. ESU �ΰ� �� �ϳ��� �� �ȵǾ �Ŀ��� ��û �÷��� �ߴµ� ESU �� �� �� ���ο� ������, �� �ȵ� ������ �ڴٰ� �߽��ϴ�.
EndoGEL POEM�� �� ���� ��� ���� ���ص��� ���� �� �ֽ��ϴ�. EndoGEL POEM ���Ŀ� ���� ȯ�� �ü��� ���� ���� ������ �˴ϴ�. Hands-on�� observation�� ��� ȿ���� �ֽ��ϴ�.
![]() [Cases]
[Cases]
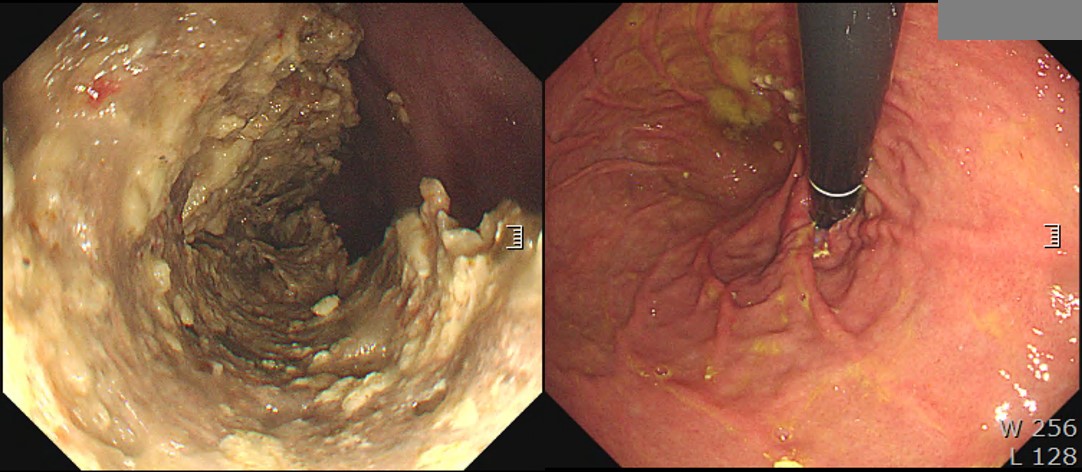
5�Ⱓ ��ģ ������ �־��� ���� ü���� ������ ���Դϴ�. ���� ���ð� �� ������ �ĵ������� ���� �� �ִٰ� �մϴ�. ����, ���ð� ������ �ڼ��� ���� EG junction�� tight �ϰ� �Ϻνĵ��� �þ ����Դϴ�. �ĵ� ������ �ִ� ������� �� ���� �Ұ��� ���̸� achalasia�� �ǽ��� �� �־�� �մϴ�. Timed barium esophagography���� �������� �Ұ��� �־����ϴ�. HRM���� LES relaxation�� ���� ������ �ʰ� panesophageal pressurization�� ���̰� �־ �������� type II achalasia�Դϴ�. POEM���� ġ���Ͽ����ϴ�. Inner circular muscle�� ���ø��� ������ �����鼭 push�Ͽ� �����ϰ� �ֽ��ϴ�. LES������ full thickness resection�� �� �ִ� ���� ȿ�����Դϴ�. ���� pneumoperitoneum�� �ణ ����� ���� ū ������ �����ϴ�. (�ξ�� ������)
![]() [FAQs]
[FAQs]
[2015-5-5. �ֵ��� ����]
Endotoday�� ���� �� �������� ���� �ֵ��� 1���Դϴ�. Achalasia�� ���� POEMġ��� �̷��� ����̳� ȿ������ ���鿡�� ������ �ŷ����� ġ������ �� �����ϴ�. ���� ���������� ���ο� ġ�������� �õ��� ���� setting ���Դϴ�. ��� �������� �鿡 ���� �������� �ǰ��� ��Ź�մϴ�.
1. POEM�� �ᱹ ���Ÿ����Ͽ��� �����ϴ°��� ������ �� �մϴ�. ������ ������ achalasiaȯ�ڿ��� ���Ÿ��븦 �����ϴ°��� ������ �ǽ��� ������ ���ð濡 ���� morbidity�� ���̰� �������.
2. ������ ��� å���ϴ� ���� �������. ���� �˱�δ� ���� POEM�� ��������ε� ������ ���� �� �����ϴ�. Ȥ�� ��� ���� �ٸ� �����Ե��� ��� ��ó�ϰ� �������. ���ο� ġ������ �õ��Կ� �־� ����ü�谡 ���� �߿��� ��ֹ��� �Ǵ� ������ ����մϴ�.
[2015-5-6. ������ �亯]
POEM�� ���� �Ͻô� �����Բ� �����Ͽ� �Ʒ��� ���� �亯�� �ҽ��ϴ�.
"���� ȯ�ڿ��� ���Ÿ����� ������ ���� �� �����ϴ�. ���� �Ϲ����� �ܰ� ������ �� ���� ȯ���� ���Ÿ��� ���輺���� ���� ������ ������ �ʽ��ϴ�. �� �߿��� ������ �����պ����Դϴ�.
�ü��� Ư���� ������ ���̴� ������ minimal mediastinitis�� ���ߵ� �� �ۿ� ����, �ü� �� �������� ���� ������� ���� �������� �ʾƼ� �̷� ���� 2������ �����պ����� ���� ���ɼ��� �ֽ��ϴ�. ���� ��ȯ�� ���� ������ ������ �����ϰ�, ����� ������ �����Ͽ� ���赵�� �Ǵ��ؾ� �ϰڽ��ϴ�.�̹��� ���Ƿ������� �� Ż���� �Ǿ��� ������ ��а� - �� �ɸ��� �� �� ������ - �մ��� ������ ���� �� ���� �����Դϴ�. ��κ��� �������� ���ð� dz�� Ȯ��� � �ؿ��Ͽ� ������ �ް� �ֽ��ϴ�. ���Ǵ� �� ��ῡ ���� ������ �ذ���� �ʾҽ��ϴ�. ��ȸ���� �̷��� Ȱ���ϰ� ������ ���̰� �ִµ���, �� ������ �ذ�� ��̰� ������ �ʾ� ��Ÿ��� ���Դϴ�.
���� �ٽ� ����غ���, POEM�� ���Ÿ����Ͽ��� �ϴ� ���� ���ڽ��ϴ�. ���� �ڵ�� ��� balloon dilatation �ڵ�� �����ϰ� ��� �����Ե��� ���� �� �����ϴ�.
�츮���� ���ο� �ü��� �����ϴ� ���� �ſ� ����� ���� �Ǿ� ���Ƚ��ϴ�. �ǻ���� ������ ������ ���뼺�� ������ �� �־�� ȯ�ڿ��� �ּ�,�ֽ��� ġ�Ḧ ������ �� �ֽ��ϴ�. ���� �̰� �Ұ����մϴ�. ȯ�ڰ� ���ص� �Ұ����մϴ�. ������ ���� ���� �ҹ��̶�� ���ֵDZ� �����Դϴ�. ���Ƿ����� ������ �ƾ߸� �ü��� �� �ִ� ���� ������ �����̴ϱ��...... �ѽ��� ���Դϴ�. ��ȣ���� �ŷڰ� �ʹ� ���� ���� �����ϱ��?
������ �� �����鼭 �ּ��� ġ�Ḧ �ϱ�� �ſ� ��ƽ��ϴ�. ������ ���� ������ �������� ġ��, ��Ȥ ���� ġ�Ḹ �� �� �ִ� ���� �츮������ �����Դϴ�. ���� �ǻ簡 ������ risk�� ���ȴ� ��쿡�� ÷�� ġ�Ḧ �� �� �ִٴ� ���� ���̳� �˴ϱ�? ���� ���� �е��� ���� �ϰ� �ֽ��ϴ�. ȯ�ڸ� ���Ͽ� �Ⲩ�� ������ �����ϴ� ���� �����Ե��� �����մϴ�.
�츮���� �ǻ���� ��(POEM, peroral endoscopic myotomy)�� ���� ���� ��(poem, ��)�� ������� ������...
[2016-10-8. ������ �߰�]
�ֱ� ��å�籹�� ȸ�ǿ��� POEM�� ����Ǿ��ٰ� �մϴ�. ������ ���� ���� �����ϰ� �ü��� �� �ְ� �� �� �����ϴ�.
[2019-11-28. �ֵ��� ����]
40�� ���� ���� ���ð��Դϴ�. �����ð��, GE junction�� ���̴� �� ����, ��Į������ �ǽɵǾ� ���ǵ帳�ϴ�. ���� ���� �� ������ ����Ұ� �ణ�� �ĵ��� ���� �ܿ��� ������ ���� ���� ���ٰ� �Ͽ����ϴ�. ���� ���ð濡�� ��Į������ �ǽɵǸ�, ���к����� �Ƿ��ؾ� �ϴ��� �ñ��Ͽ� ���ǵ帳�ϴ�.

[2019-11-28. ������ �亯]
���� �����Դϴ�. ��Į������ ���ð� �Ұ��� ���ؼ��� �� ���� �����帰 �� �ֽ��ϴٸ�, ��� ��κ��� nonspecific�ϰ� ����� ������ ���� �ʽ��ϴ�.
Endoscopic findings of achalasia
- Dilation of the esophagus. Dilated esophagus may droop to both sides of the spine. Severely dilated esophagus can be curved.
- Food remnant in the esophagus. A lot of fluid can be found.
- Whitish coating of the mucosa caused by adhesion of the remained food inside of the esophagus and thickening of the mucosa.
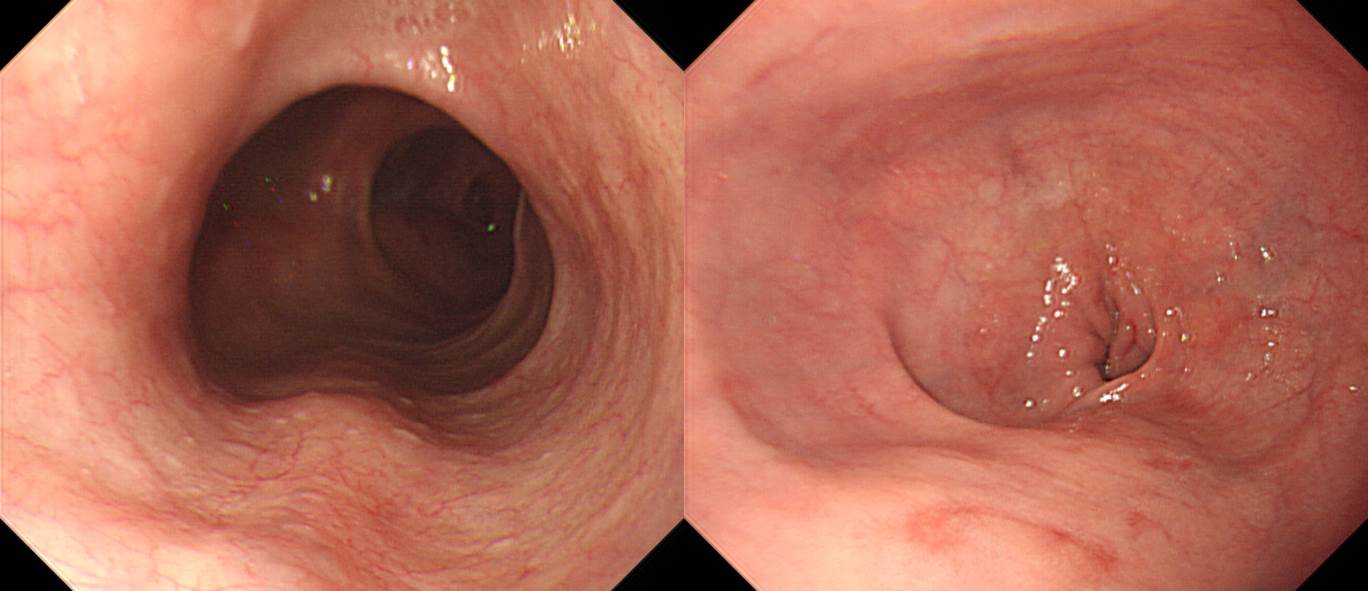
- Esophago-gastric junction is normal or slightly tight. There is no evidence of sliding hiatal hernia. The SCJ does not move upward by deep inspiration. Endoscope passes through the tight segment with some resistance.
- Rosette-like esophageal folds
- Abnormal contraction of the esophagus. Sometimes, simultaneous contraction is seen.
- In retroflection, the endoscope is tightly wrapped by the cardia mucosa.
- Pinstripe pattern (PSP)
���ٸ� ������ ���� ���� ���ð濡�� �쿬�� �̿� ���� �Ұ��� �ǽɵ� �� ��� �ؾ� �ϴ��� �����ϼ̴µ���... ������ ����� �������� ���ٸ� �� �̻� �� ���� �����ϴ�. ������ ���ٴµ� ���� �� �ʿ��ϰڽ��ϱ�? "������ �� �����ϱ�?"��� open question���� ����Ƶ� ������ ��Ű�� ����� �ʴ���, ������ �ɸ����� �ʴ���, ���� ������ ���� �������� �ʴ���, ü���� �������� ���� ��ü������ ����� �� ���� �� �� ���� �� �����ϴ�.
ȯ���� �������� SC junction ������� ������ �������� (���ſ��� minimal change��� �ҷ����� ��) �ӻ��� ���Ǵ� ���� ���� �� �����ϴ�.
������... �Ʒ� ȯ�ڴ� ���� chest CT���� �쿬�� achalasia�� �߰ߵǾ��� ����Դϴ�. ����Ҵ��� �������� dysphagia�� ���� ������ �־��ٰ� �߽��ϴ�.
[2021-10-31] Facebook���� POEM myotomy�� clutchcutter (Fujifilm)���� �ϴ� ���� ���ҽ��ϴ�. ������ �� �����ϴ�. ������ �����Դϴ�.
[2022-12-22] Fujifilm EndoGEL POEM (�� ������)
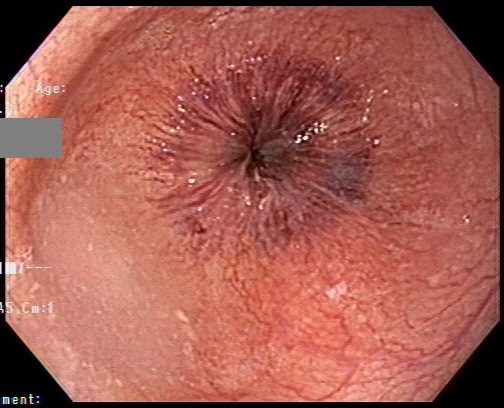
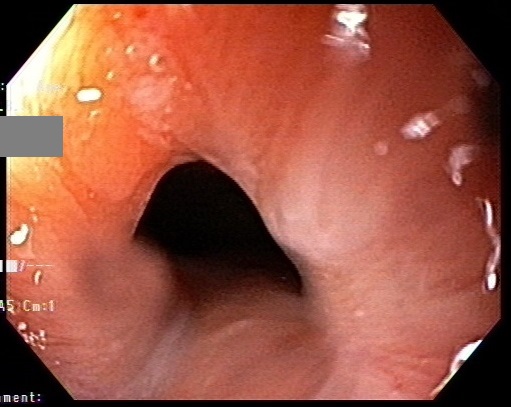
[2023-6-2. SMC ����ȸ ����]
Sigmoid type achalasia���� POEM�� ��������, ���� ������ ��� �������� �ñ��մϴ�.
[2023-6-3. ������ �亯]
���� ����ȸ������ sigmoid type achalasia���� POEM�� ȿ���� ���� �� �ִ� ������, �� POEM �� Ȯ��� �ĵ��� ȸ������ ���� �� �ִ� ���̶�� comment�� �־����ϴ�.
���� ���� POEM �ü��� ������ �ʰ� ������, ���忡 ������ sigmoid type achalasia������ POEM�� ����� ȿ���� �ִٰ� �մϴ�. �ٸ� ���� ���� ���� ���� �� ȿ���� ���� �� �ִ� ������ �����ϸ� ��� �ͽ��ϴ�.
Per-oral endoscopic myotomy (POEM) for a sigmoid type of achalasia: short-term outcomes and changes in the esophageal angle Surg Endosc 2020
Peroral endoscopic myotomy for advanced achalasia with sigmoid-shaped esophagus: long-term outcomes from a prospective, single-center study Surg Endosc 2015
![]() [References]
[References]
1) Anorectal manometry �ǵ� - SMC manual (2007)
2) ���ɰ˻� �ǵ� - ������ SMC manual (2007)
PDF 0.5M
3) POEM ��ȣ ���� 2017 - ���ο�. ��ȣ ����
4) 2024�� 8�� 18�� KSGE ���ð� ���̳� �赵�� ������ ���� log-in �
© �Ͽ����ð汳�� �ٸ����ð濬���� ������. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.




{kind=link}