EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [EBV-associated gastric cancer] - 終
[EBV-associated gastric cancer] - 終
1. Introduction
2. EBV-associated gastric cancer의 임상적 특성
3. ESD for EGC with EBV infection
4. EBV and Helicobacter pylori coinfection
5. Cases
6. References
![]() 1. Introduction
1. Introduction
EBV
EBV-associated gastric cancer
 링크
링크
The Cancer Genome Atlas (TCGA, 2014)
* 참고: Epstein-Barr virus 관련 위암 이봉은. Korean J Helicobacter Up Gastrointest Res 2021 (PDF)
![]() 2. SMC Monday GI conference 2017-5-15. EBV-associated gastric cancer의 임상적 특성 (임상강사 홍지택)
2. SMC Monday GI conference 2017-5-15. EBV-associated gastric cancer의 임상적 특성 (임상강사 홍지택)
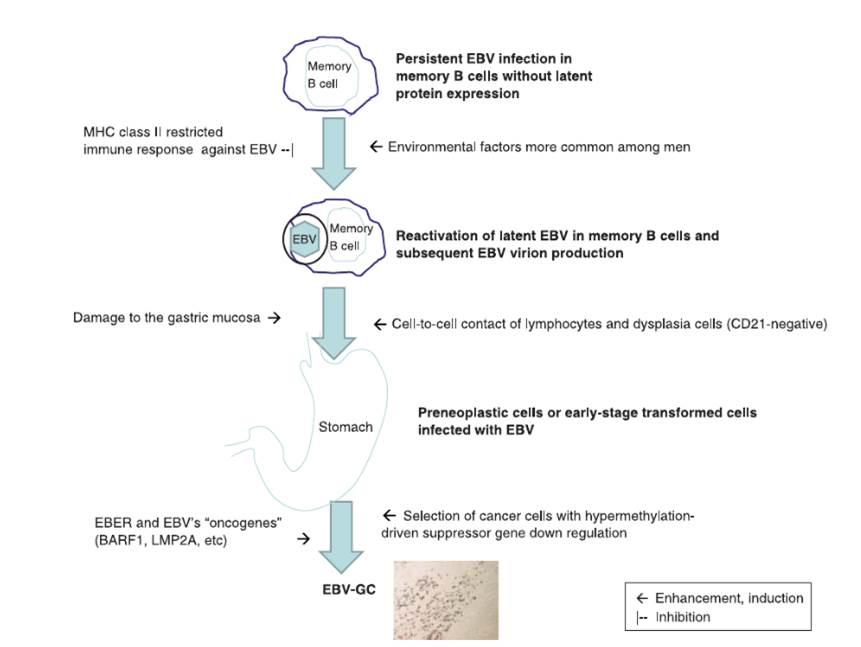
Cell free virus는 감염능력이 낮으나 한 세포에서 다른 세포로 옮기는 효율은 훨씬 높습니다.
Latent protein 발현 양상에 따라 세 가지 type을 나눌 수 있습니다. 위암은 latency type I과 type II과 관련된 것으로 생각됩니다. 처음에는 latency type III로 시작하다가 latent protein 발현을 down regulation 하여 latency type II와 type I으로 변형됩니다.
Remnant gastric cancer에서의 감염율이 그냥 proximal gastric cancer보다 훨씬 더 많습니다. Billroth II에서 더 높다고 합니다.
![]() 3. ESD for EGC with EBV infection
3. ESD for EGC with EBV infection
일본에서 흥미로운 논문이 발표되었습니다.
EBV positive EGC는 예후가 좋으므로 ESD 후 depth of invasion이 깊어도 경과관찰을 할 수 있다는 이야기인데... 고려해볼만 하다고 생각합니다.
![]() 4. EBV and Helicobacter pylori coinfection
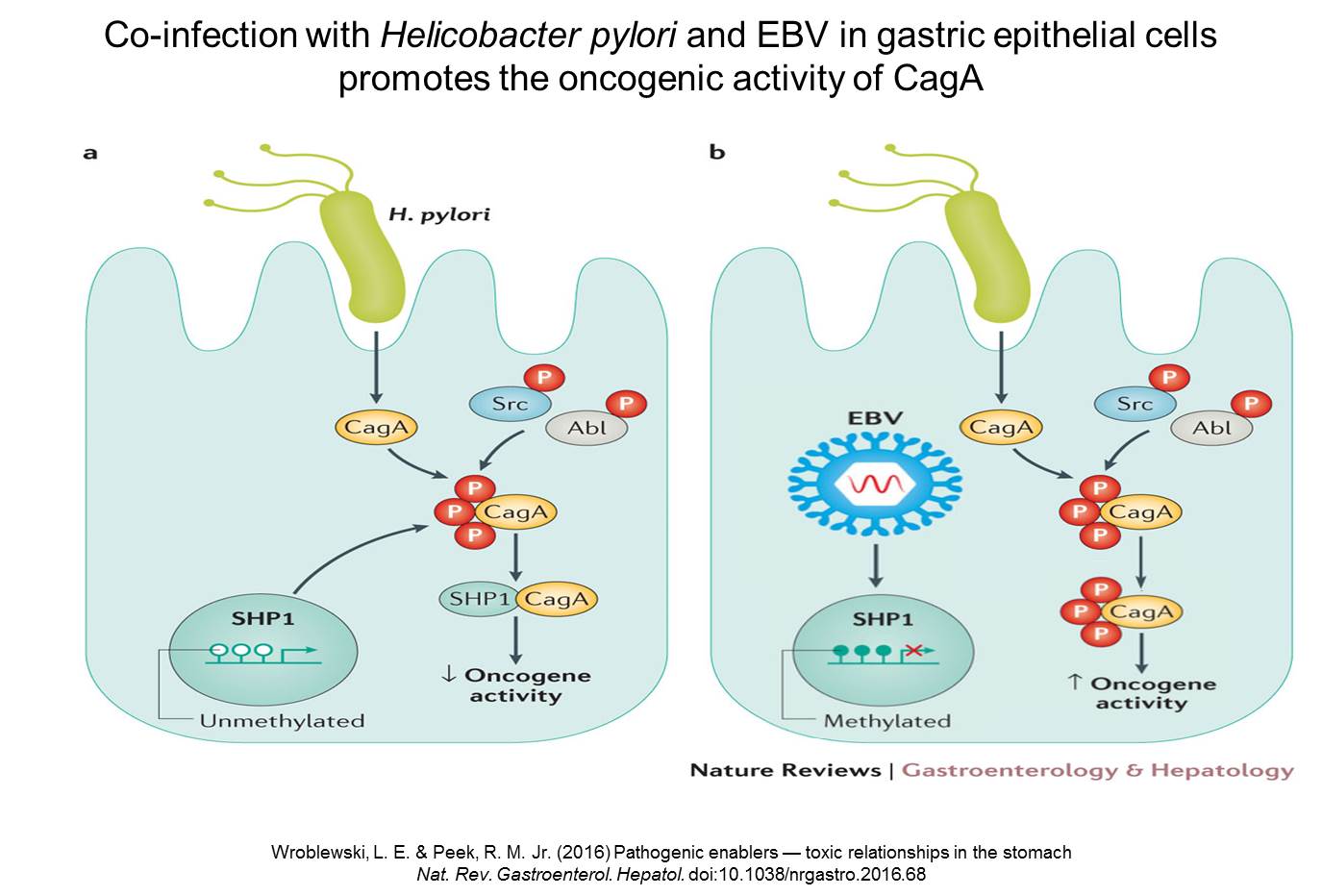
4. EBV and Helicobacter pylori coinfection
Although EBV and H. pylori coinfection might synergistically increase the risk of developing gastric cancer, EBV infection seems to be an important factor for determining the clinical phenotype in EBV +/HP+ gastric cancer. (참고: 2023년 Gut Liver editorial)
![]() [Cases]
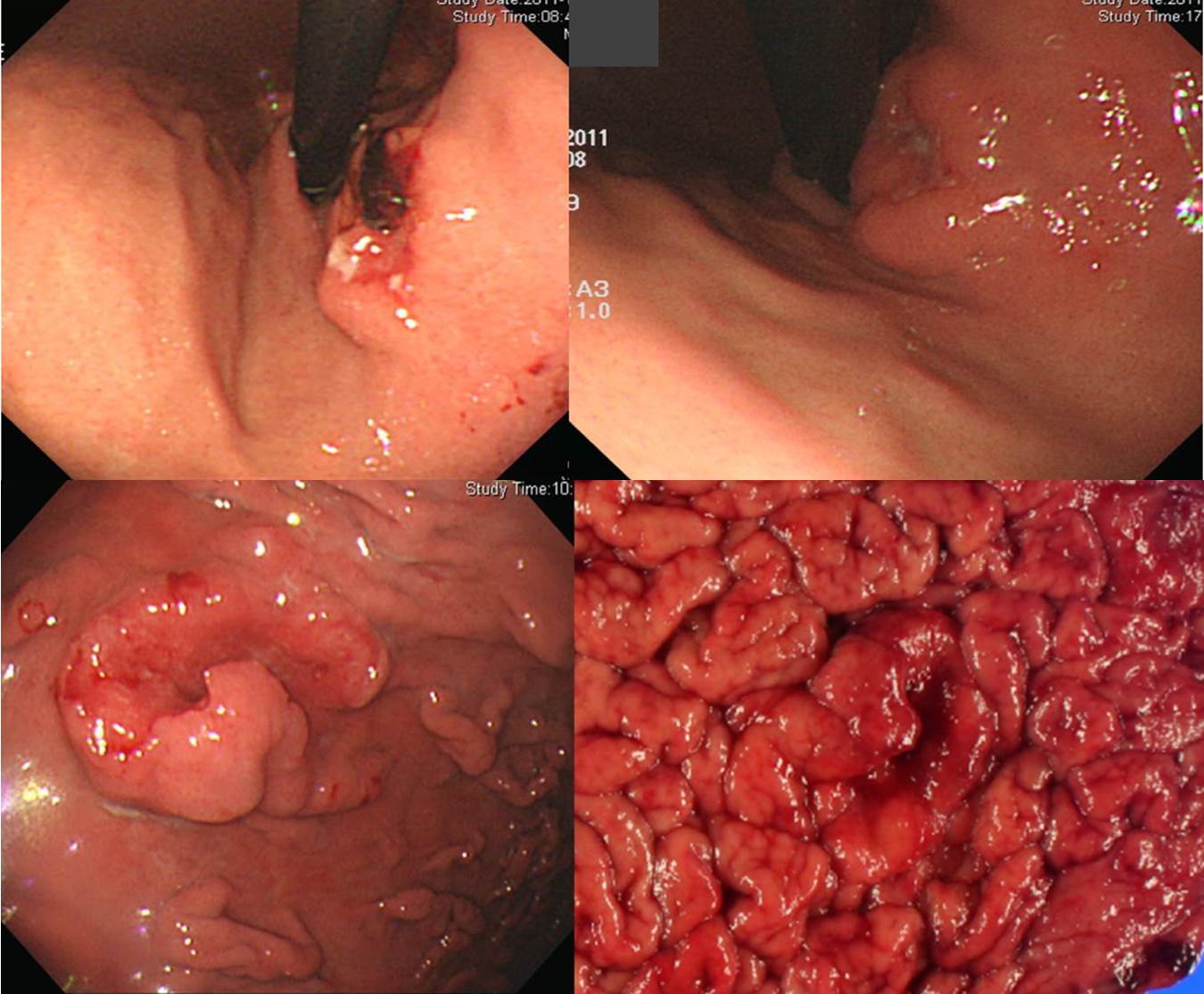
[Cases]
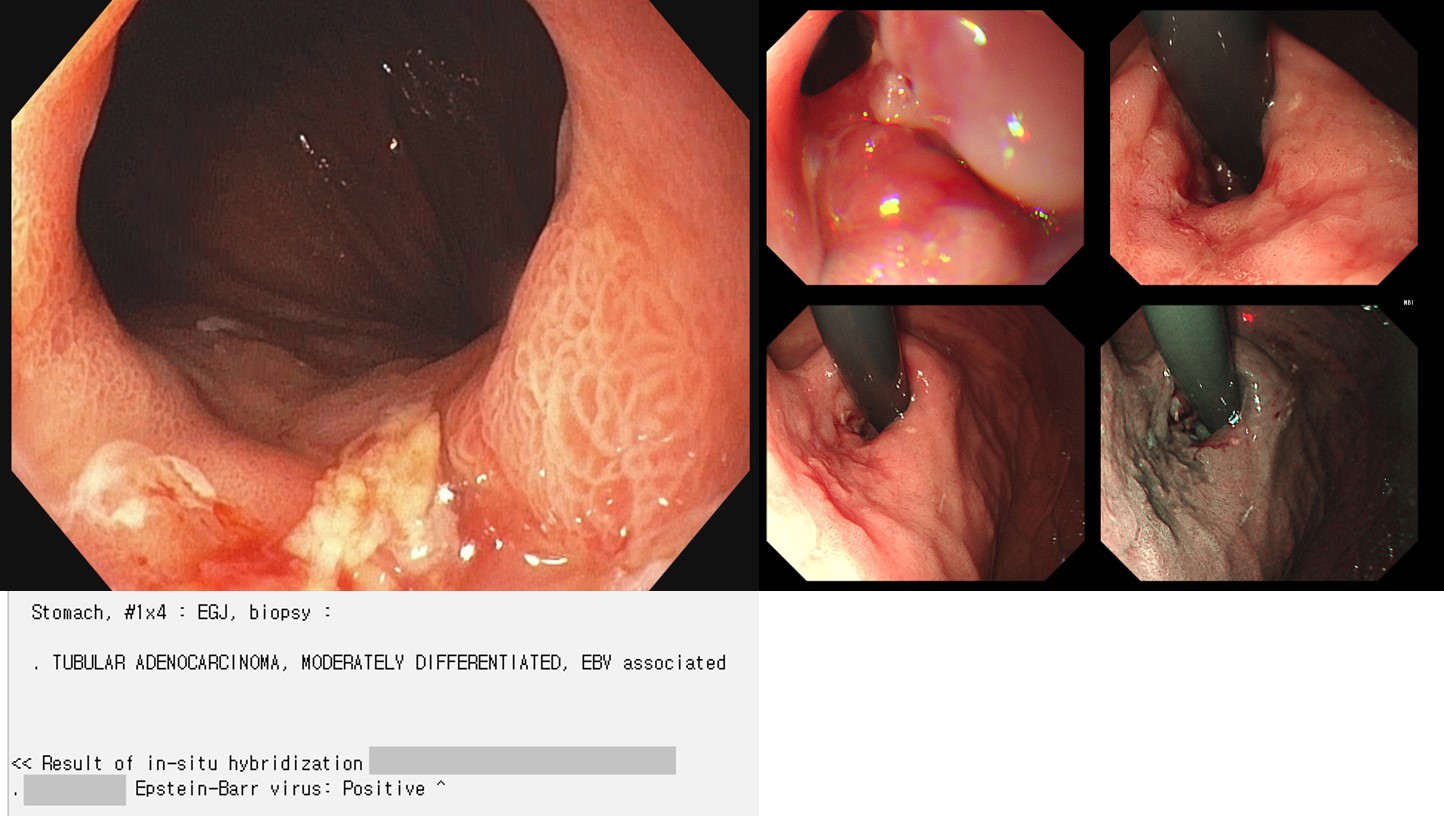
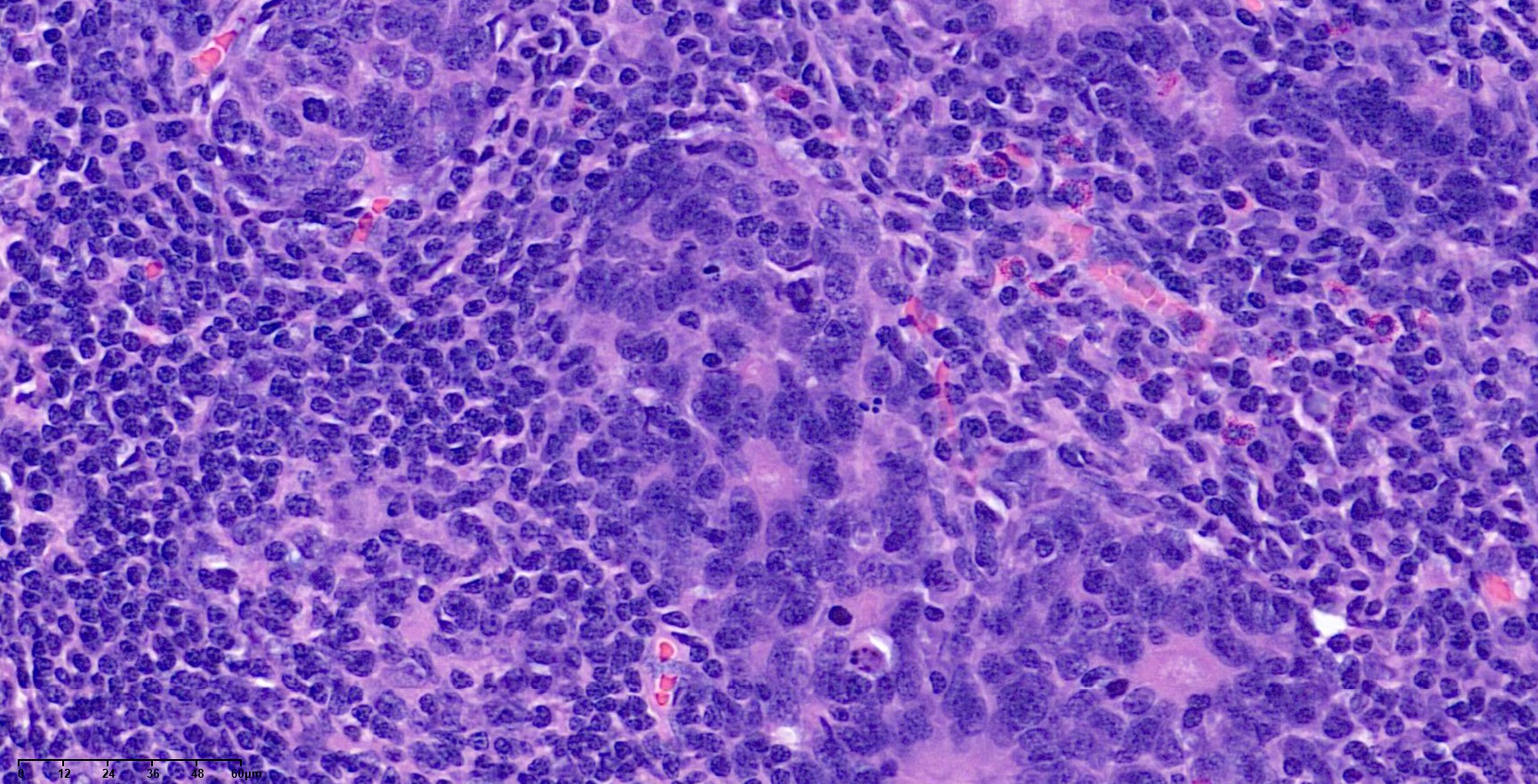
EBV-associated gastric cancer is usually diagnosed by careful pathologic examination and immunohistochemistry after gastrectomy. In this case, however, association with EBV was found by forceps biopsy specimen.
Stomach, radical total gastrectomy: Early gastric carcinoma
1. Location : upper third, Center at cardia (Siewert II) and lesser curvature
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, poorly (solid) differentiated
4. Histologic type by Lauren : indeterminate
5. Size : 4.5x2.8 cm
6. Depth of invasion : invades submucosa (sm3) (pT1b)
7. Resection margin: free from carcinoma, safety margin: proximal 0.2 cm, distal 20.2 cm
8. Lymph node metastasis : metastasis to 1 out of 25 regional lymph nodes (pN1) (perinodal extension: absent) (1/25: "1", 1/1; "2", 0/0; "3", 0/7; "4", 0/5; "5", 0/0; "6", 0/1; "7", 0/2; "9", 0/6; "8a", 0/1; "11p", 0/0; "12a", 0/1; "4sb", 0/0; "11", 0/1)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Associated findings : gastritis cystica profunda
13. Peritoneal cytology : negative
14. AJCC stage by 8th edition: pT1b N1
. c-erbB-2(HER2) : Negative ( 1+ )
. Epstein-Barr virus in-situ hybridization: Positive (Inflamed / TSP - High)
Early gastric carcinoma
1. Location : body, postero greater curvature
2. Gross type : EGC type IIb
3. Histologic type : tubular adenocarcinoma, moderately differentiated (EBV-positive)
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 34 mm (2) vertical diameter, 29 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion : 600 ㎛) (pT1b)
7. Resection margin : free from carcinoma(N), safety margin : distal 3 mm, proximal 200 ㎛, anterior 4 mm, posterior 2 mm, deep 100 ㎛ (sm only)
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
13. in situ hybridization: Epstein-Barr virus : Positive (CLR, Crohn's-like reaction)
![]() [References]
[References]
1. EndoTODAY Lymphoepithelioma-like carcinoma
2. Epstein-Barr virus 관련 위암 이봉은. Korean J Helicobacter Up Gastrointest Res 2021 (PDF)
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.